

Abstract
Background:
Primary cardiac angiosarcoma is rare, but it is the most aggressive type of cardiac malignant tumor. When disease is confirmed it is often late in its stage resulting in a poor prognosis.
Case presentation:
We reported a 52-year-old woman who complained of dyspnea for 2 months and dry cough for 10 days. Computed tomography (CT), 18F-fluorodeoxyglucose (18F-FDG), positron emission tomography-computed tomography (PET-CT), and transthoracic echocardiography showed a space-occupying lesion 7 cm × 5 cm × 5 cm in the right atrium. Malignant cells can be seen in pericardial fluid by pericardiocentesis in local hospital, but not be diagnosed definitely. We conducted CT-guided biopsy of the tumor and observed the necrotic tissues. An exploratory thoracotomy was performed and histological examination confirmed angiosarcoma. Unable to be surgical excision due to infiltrating widely, the patients received chemotherapy with docetaxel for 2 cycles and the disease was progressive. Antiangiogenesis-targeted therapy was combined with chemotherapy for 3 months. Unfortunately, the tumor was still in progress. She died of respiratory failure, survived for 10 months.
Conclusion:
It is difficult to diagnose the primary cardiac angiosarcoma in early stage. Chemotherapy and target therapy are very limited in this case. Surgery remains the preferred treatment for patients with primary cardiac angiosarcoma. More efforts should be carried out on the effective diagnosis and multimodality treatment for this malignant disease.
Keywords: chemotherapy, diagnosis, primary cardiac angiosarcoma, target therapy
1. Introduction
Primary cardiac angiosarcoma is the most aggressive malignant primary cardiac tumor. The most common sarcomas are tumors of vascular origin, in particular, angiosarcoma.[1] Angiosarcomas usually originate in the right atrium and frequently occur with nonspecific symptoms, such as dyspnea, cough, heart failure, arrhythmias, and so on.[2] Delayed diagnosed is associated with a poor prognosis. There are no clearly guidelines recommended to current management of cardiac angiosarcoma. Radical resection followed by adjuvant radiotherapy represents the standard treatment to the limited disease.[3,4] In case of advanced stage, integrated with chemotherapy and radiotherapy may lead to shrinkage of the mass. Taxanes have been reported shown antitumor activity in angiosarcoma.[5–7] In view of target therapy, little has been reported. Here we reported a 52-year-old woman who diagnosed with advanced cardiac angiosarcoma and lost the opportunity of radical resection. Then, she did chemotherapy and antiangiogenesis-targeted therapy positively. The result was disappointing and she survived for 10 months.
2. Case presentation
A 52-year-old woman admitted to our hospital who complained of dyspnea for 2 months and dry cough for 10 days without any obvious causes. She was healthy previous and without family history. Transthoracic echocardiography revealed a large amount of pericardial fluid. Dyspnea was alleviated by pericardiocentesis and malignant cells can be seen in pericardial fluid, but not be diagnosed definitely. Positron emission tomography-computed tomography (PET-CT) revealed a large defined enhancing soft tissue in the right atrium, considering the malignant lesion. Also, increased 18F-fluorodeoxyglucose (18F-FDG) uptake was observed in midsternum, likely due to metastasis (Fig. 1). A subsequent chest computed tomography (CT) scan showed a large size tumoral lesion (approximately 7 cm × 5 cm × 5 cm) that its origin was right atrium, invading near fiber pericardium (Fig. 2). Transthoracic echocardiography showed solid occupation in the anterolateral of right atrium, tricuspid regurgitation in small quantities (Fig. 3). Tumor markers were detected that the CA125 was 97.9 U/mL, neuron-specific enolase (NSE) was 24.47 ng/mL. In order to make a correct diagnosis, the CT-guided biopsy was conducted for the tumor and the necrotic tissues were found. Considering higher risk would be accompanied by puncture again, an exploratory thoracotomy was performed after consultation by multidisciplinary team. Opening the pericardium, we could see extensive adhesion between the pericardium and the heart. After cardiopulmonary bypass was established, we separated right atrium from the pericardium difficultly. The tumor was located at the anterior inferior wall of the right atrium, rich vascularized, hard and uneven (Fig. 4). Because of extensive involvement, the tumor was unresectable. A 5 mm × 5 mm tissue was removed for pathology. Although we ligatured the base before we removed the tissue, bleeding continued, it was stopped after performing pressing hemostasis for 30 minutes. The pathology diagnosis was angiosarcoma. The immunohistochemistry results were as follows: CD34(+), CD31(+), F8(+), Ki67 10% to 30%(+), p53(−), CD68(−), SMA(−), HMB45(−), CK(−), MelanA(−), LCA(−) (Fig. 5). Ten days later, the patient began to receive chemotherapy with docetaxel for 2 cycles and the disease was progressive. Radiotherapy was declined in view of its cardiotoxicity. Bevacizumab was combined with chemotherapy for 3 months. Unfortunately, the tumor was still in progress. She died of respiratory failure, survived for 10 months. This case report was performed with the signed informed consent from the family of the patient, and the personal information of the patient was made anonymous.
Figure 1.
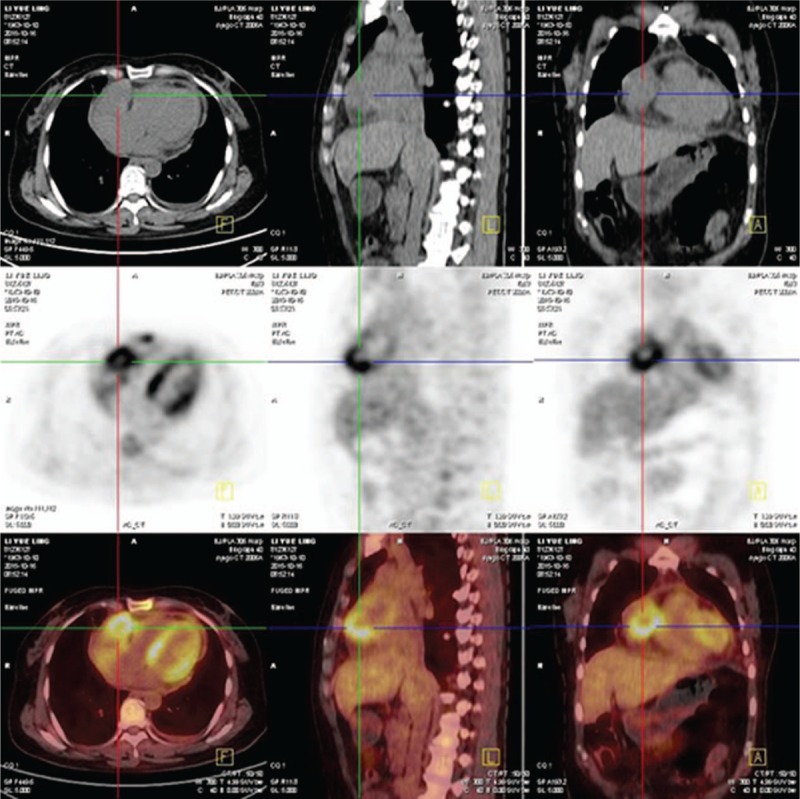
PET-CT showed high metabolic activity in the right atrial mass.
Figure 2.
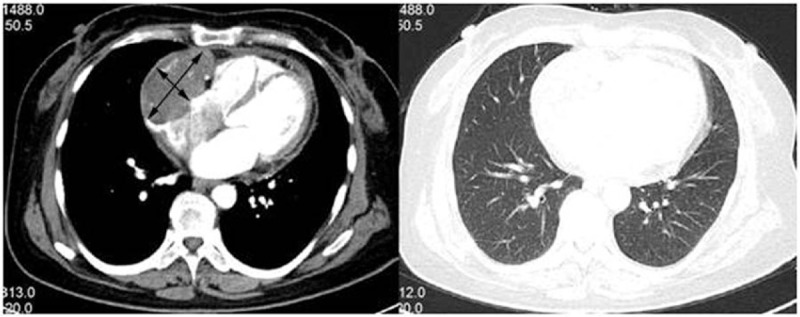
Chest CT scan showed a large size tumoral lesion (approximately 7 cm × 5 cm × 5 cm).
Figure 3.

Transthoracic echocardiography showed solid occupation in the anterolateral of right atrium.
Figure 4.
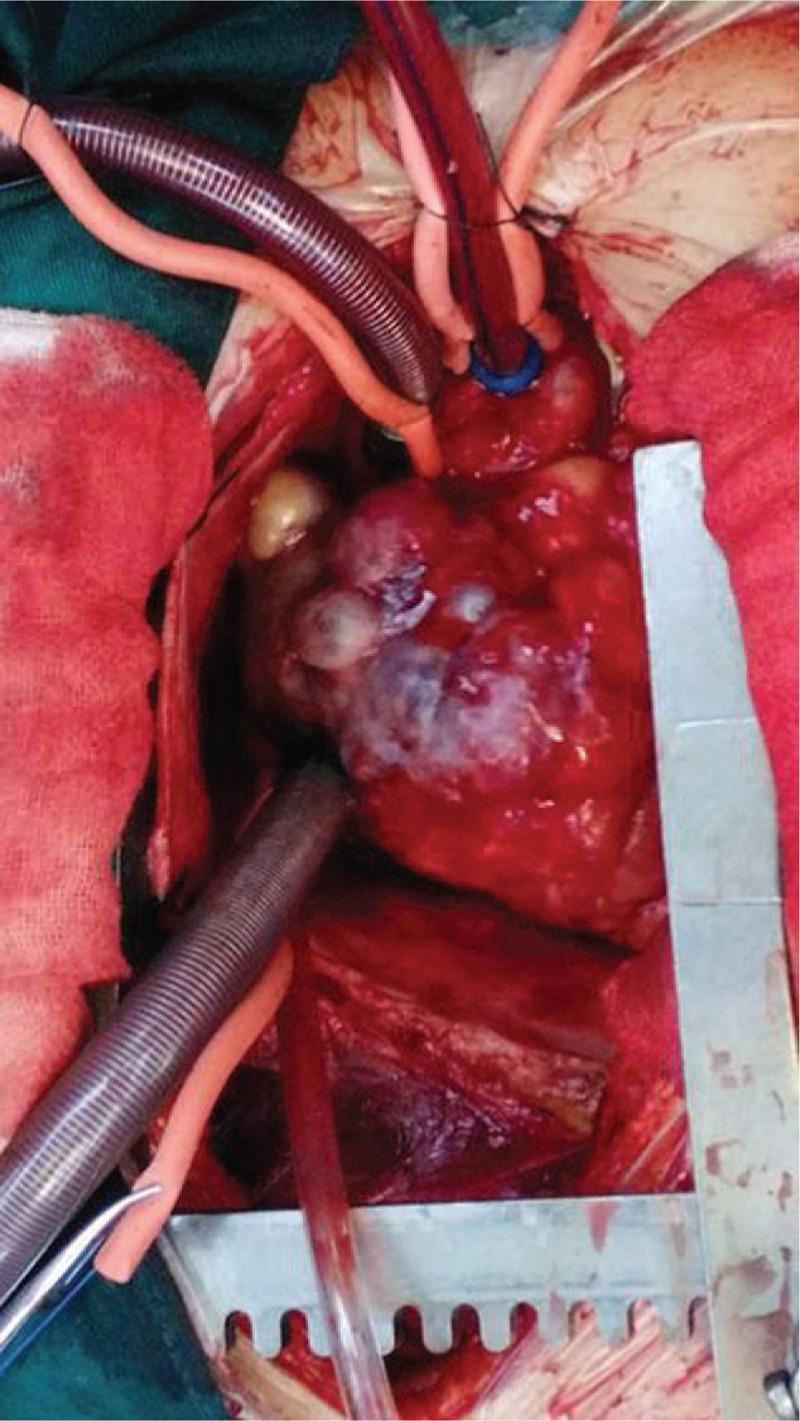
The tumor was located at the anterior inferior wall of the right atrium, rich vascularized, hard and uneven.
Figure 5.
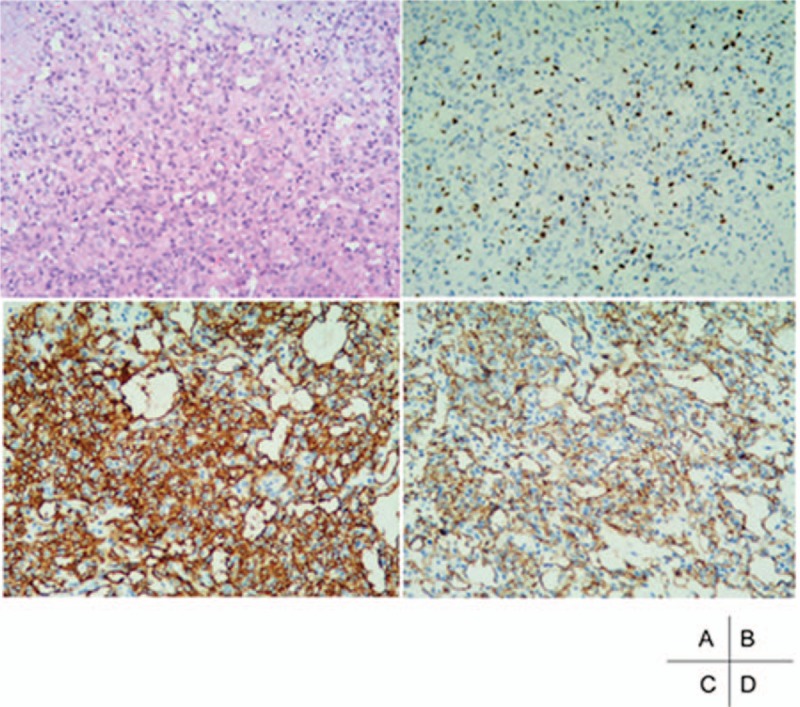
(A) Hematoxylin and eosin staining displayed atypical spindle shaped and epithelioid tumor cells (×10). Immunohistochemical staining the tumor cells are stained with Ki-67, CD34 and CD31 (×10, B–D).
3. Discussion
The incidence of primary cardiac neoplasm is approximately 0.0001% to 0.030%, 25% are malignant, and cardiac angiosarcoma is the most common pathological type.[8] Cardiac angiosarcomas usually originate in the right atrium, and the most common sites for metastasis are the lung and the pericardium.[9] Transthoracic echocardiography is usually the initial diagnostic tool for cardiac tumors, which has a sensitivity of 93% for detecting cardiac masses. Kupsky et al have reported that the absence of a stalk was a universal finding that may help distinguish angiosarcoma from benign, primarily pedunculated such as myxom and papillary fibroelastoma.[10,11] CT scanning is a valuable supplement tool to echocardiography. Magnetic resonance imaging (MRI) is often used to detect tissue characterization and tumor infiltration.[12]18F-FDG PET-CT could be used to noninvasively determine malignant tumors with a sensitivity of 100%.[13] However, MRI, CT, or PET-CT cannot replace biopsy for the final diagnosis. Literatures have ever been reported that pericardial fluid analysis in 15 cases (88%), and the results were negative for malignancy in all.[11] Pericardiocentesis frequently yields bloody or necrotic tissues, cytology is often negative involvement.[14,15] Just as we have done, pericardiocentesis and CT-guided biopsy were all failure. Cardiac angiosarcoma was diagnosed after exploratory thoracotomy. Immunohistochemistry staining of CD31 and CD34 confirmed endothelial origin. Ki67 was used as a prognostic factor. High values (≥10%) have been statistically correlated with poor survival outcome.[16]
Surgical resection remains the first-line treatment of choice. Unfortunately, many patients lost their operating opportunities when found it. Adjuvant therapies, including chemotherapy and radiotherapy are all debatable. No randomized controlled trials have been performed to provide evidence to these adjuvant therapies. With regard to targeted therapy, Imatinib[17] is not found to be an active agent against advanced sarcoma in phase II trials. Sorafenib[18] exerts activity against angiosarcoma, with 3.8 and 14.9 months progression-free survival and overall survival, respectively. Bevacizumab[19] is effective for angiosarcoma with 57% (13/23) patients showing a response and no progression. This patient experienced chemotherapy with docetaxel which has been reported antitumor activity in angiosarcoma.[5–7] The efficacy was evaluated as progression after 2 cycles. Bevacizumab was combined with chemotherapy for 3 months to this patient. Unfortunately, the tumor was still in progress. She survived for 10 months and died. The literatures have reported that the prognosis of cardiac angiosarcoma is generally poor, with survival ranging from 6 to 12 months after the diagnosis has been established.[20] Although, this case responds poorly to chemotherapy and targeted therapy, some of limited cases, after radical resection, a multidisciplinary approach with adjuvant chemotherapy, radiotherapy, and targeted therapy may improve overall survival even reaching 33 months.[21–23]
Primary cardiac angiosarcoma is rare and difficult to diagnosis at its early stage. Most patients lost their operation opportunities. There are no practical guidelines for management advanced disease in particular an evidence-based advice. Primary cardiac angiosarcoma is largely resistant to chemotherapy and/or radiation and the vast heterogeneity within the tumor. The exact benefit and its place in a multimodality treatment regimen are still under investigation.
Footnotes
Abbreviations: 18F-FDG = 18F-fluorodeoxyglucose, CT = computed tomography, MRI = magnetic resonance imaging, NSE = neuron-specific enolase, PET-CT = positron emission tomography-computed tomography.
The authors have no conflicts of interest to disclose.
References
- [1].Silverman NA. Primary cardiac tumors. Ann Surg 1980;191:127–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Kim CH, Dancer JY, Coffey D, et al. Clinicopathologic study of 24 patients with primary cardiac sarcomas: a 10-year single institution experience. Hum Pathol 2008;39:933–8. [DOI] [PubMed] [Google Scholar]
- [3].Penel N, Lansiaux A, Adenis A. Angiosarcomas and taxanes. Curr Treat Options Oncol 2007;8:428–34. [DOI] [PubMed] [Google Scholar]
- [4].Fury MG, Antonescu CR, Van Zee KJ, et al. A 14-year retrospective review of angiosarcoma: clinical characteristics, prognostic factors, and treatment outcomes with surgery and chemotherapy. Cancer J 2005;11:241–7. [DOI] [PubMed] [Google Scholar]
- [5].Ram Prabu MP, Thulkar S, Ray R, et al. Primary cardiac angiosarcoma with good response to Paclitaxel. J Thorac Oncol 2011;6:1778–9. [DOI] [PubMed] [Google Scholar]
- [6].Suderman D, Cooke A, Wong R, et al. Treatment of cardiac angiosarcoma with radiation and docetaxel: a case report with partial response and prolonged stable disease. J Thorac Oncol 2011;6:834–5. [DOI] [PubMed] [Google Scholar]
- [7].Hata A, Katakami N, Fujita S, et al. Angiosarcoma arising from right atrium: remarkable response to concurrent chemoradiotherapy with carboplatin and paclitaxel. J Thorac Oncol 2011;6:970–1. [DOI] [PubMed] [Google Scholar]
- [8].Minichillo S, Pantaleo MA, Nannini M, et al. Efficacy of weekly docetaxel in locally advanced cardiac angiosarcoma. BMC Res Notes 2015;8:325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Meng Q, Lai H, Lima J, et al. Echocardiographic and pathologic characteristics of primary cardiac tumors: a study of 149 cases. Int J Cardiol 2002;84:69–75. [DOI] [PubMed] [Google Scholar]
- [10].Riles E, Gupta S, Wang DD, et al. Primary cardiac angiosarcoma: a diagnostic challenge in a young man with recurrent pericardial effusions. Exp Clin Cardiol 2012;17:39–42. [PMC free article] [PubMed] [Google Scholar]
- [11].Kupsky DF, Newman DB, Kumar G, et al. Echocardiographic features of cardiac angiosarcomas: the Mayo Clinic Experience (1976–2013). Echocardiography 2016;33:186–92. [DOI] [PubMed] [Google Scholar]
- [12].Campanile A, Tavazzi G, Alam MH, et al. An unexpected finding in an asymptomatic patient with atrial fibrillation: cardiac angiosarcoma. Lancet 2016;387:e29. [DOI] [PubMed] [Google Scholar]
- [13].Rahbar K, Seifarth H, Schafers M, et al. Differentiation of malignant and benign cardiac tumors using 18F-FDG PET/CT. J Nucl Med 2012;53:856–63. [DOI] [PubMed] [Google Scholar]
- [14].El-Osta HE, Yammine YS, Chehab BM, et al. Unexplained hemopericardium as a presenting feature of primary cardiac angiosarcoma: a case report and a review of the diagnostic dilemma. J Thorac Oncol 2008;3:800–2. [DOI] [PubMed] [Google Scholar]
- [15].Oshima K, Ohtaki A, Kano M, et al. Primary cardiac angiosarcoma associated with cardiac tamponade: case report. Jpn Circ J 1999;63:822–4. [DOI] [PubMed] [Google Scholar]
- [16].Meis-Kindblom JM, Kindblom LG. Angiosarcoma of soft tissue: a study of 80 cases. Am J Surg Pathol 1998;22:683–97. [DOI] [PubMed] [Google Scholar]
- [17].Chugh R, Wathen JK, Maki RG, et al. Phase II multicenter trial of imatinib in 10 histologic subtypes of sarcoma using a Bayesian hierarchical statistical model. J Clin Oncol 2009;27:3148–53. [DOI] [PubMed] [Google Scholar]
- [18].Maki RG, D’Adamo DR, Keohan ML, et al. Phase II study of sorafenib in patients with metastatic or recurrent sarcomas. J Clin Oncol 2009;27:3133–40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Agulnik M, Yarber JL, Okuno SH, et al. An open-label, multicenter, phase II study of bevacizumab for the treatment of angiosarcoma and epithelioid hemangioendotheliomas. Ann Oncol 2013;24:257–63. [DOI] [PubMed] [Google Scholar]
- [20].Vander Salm TJ. Unusual primary tumors of the heart. Semin Thorac Cardiovasc Surg 2000;12:89–100. [DOI] [PubMed] [Google Scholar]
- [21].Park WK, Jung SH, Lim JY. Cardiac angiosarcoma on the right atrium: two cases. Korean J Thorac Cardiovasc Surg 2012;45:120–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Wang M, Fu G, Jiang H, et al. Multimodality treatment for cardiac angiosarcoma. Intern Med 2014;53:1949–53. [DOI] [PubMed] [Google Scholar]
- [23].Jang Y, Kim J, Shim JW, et al. Primary cardiac angiosarcoma: a prolonged response to surgical resection followed by concurrent chemoradiotherapy with docetaxel. Springerplus 2016;5:648. [DOI] [PMC free article] [PubMed] [Google Scholar]