

Supplemental Digital Content is available in the text
Keywords: body mass index (BMI), caesarean section, combined spinal-epidural anesthesia, complications, obesity
Abstract
Background:
Up to 40% of women gain excessive weight during pregnancy. Obesity complications and risks in parturient women undergoing cesarean section (CS) with different anesthetic methods remain unknown. This study aimed to assess the safety and risk of obese women undergoing CS delivery with various perioperative anesthetic methods.
Methods:
Seven hundred ninety parturient women underwent CS under general anesthesia (GA), intraspinal anesthesia including epidural anesthesia (EA) and combined spinal-epidural anesthesia (CSEA). They were divided into morbid (n = 255), severe (n = 274), and non-obesity (n = 261) groups. This study is registered with ClinicalTrials.gov (number NCT03002636).
Result:
Between 2013 and 2016, 790 pregnant were assessed. Compared with the non-obesity group, there were significantly more fetal distress and higher body mass index (BMI) in the morbid obesity group (P = .0001 and P = .001, respectively). Significantly more patients showed preeclampsia, multifetation, amniotic fluid abnormality, and high bleeding amounts in the morbid obesity group compared with the non-obesity group (P = .0001, P = .048, P = .017, and P = .018, respectively); more patients were administered EA and GA compared with the non-obesity group (P = .0001 and P = .0001, respectively). More post-anesthesia care unit (PACU) patients were found in the severe obesity group no more than the non-obesity group. Significantly increased anesthesia puncture times for 5 > n ≥ 3 and n ≥ 5 were obtained in the morbid obesity group (P = .0001 and P = .0001, respectively), with more patients in the puncture sitting position, compared with the non-obesity group (P = .0001).
Conclusion:
GA, EA, and CSEA are safe and effective in severely or morbidly obese patients. Morbidly obese parturient show increased likelihood for fetal distress, PACU, sitting position puncture, puncture difficulty, and other pregnancy complications. There were more anesthesia puncture times in morbidly obese patients.
1. Introduction
The increased prevalence of obesity in the general population extends to women of reproductive age. Over the past decades, obesity incidence has tripled,[1] and the number of obese patients undergoing caesarean section has also increased. Diseases associated with obesity such as diabetes, severe preeclampsia, cardiopulmonary diseases, and obstructive sleep apnea reduce the margin of safety of anesthetic drugs.[2] Simas et al[3] found that more than one-third of pregnant women are overweight or obese. In the most severe form, obesity may be associated with respiratory compromise that can be exacerbated by the physiological demands of pregnancy.[4]
Large studies reporting complications and risks in parturient women undergoing CS for morbidly obese individuals are scarce. Complications and risks in obese parturient women under CS with different anesthetics and newborn during the perioperative period also remain unclear. Therefore, this study aimed to explore the safety and risk of perioperative anesthesia in obese pregnant women undergoing CS with general anesthesia (GA), epidural anesthesia (EA), or epidural anesthesia combined with spinal anesthesia.
2. Materials and methods
2.1. Patients
The present study was approved by the Research Ethics Board of International Peace Maternity and Child Health Hospital, Shanghai Jiao Tong University, School of Medicine. It complied with the “Personal Information Protection Act” in International Peace Maternity and Child Health Hospital, School of Medicine, Shanghai Jiao Tong University. The study was performed in International Peace Maternity and Child Health Hospital, with patients enrolled from January 1, 2013 to September 30, 2016. A total of 892 individuals were assessed for eligibility. The patients were divided into 3 groups: morbid obesity (n = 260), severe obesity (n = 280), and non-obesity (n = 270) with body mass index (BMI) >40 kg/m2, 30 kg/m2 ≤ BMI ≤ 40 kg/m2, and BMI < 30 kg/m2, respectively. BMI was calculated for each patient by using the formula kg/m2 based on patient reported height and weight at the initial visit. The inclusion criteria were ASA Physical Status grade ΙΙ–ΙΙΙ and nulliparity. Patients with the following conditions were excluded from the study: scoliosis, congenital heart disease, lung, liver, kidney diseases, and increased intracranial pressure (ICP). When intra-vertebral anesthesia produced insufficient or excessively high blockade, GA was used as a rescue technique. A total of 790 patients completed the protocol and their data were analyzed. Twenty women did not complete the protocol for baseline characteristics. To ensure an objective assessment of risk for CS, statistical analysis was restricted only to nulliparous patients.
2.2. Anesthesia
The patients underwent GA, EA, or combined spinal-epidural anesthesia. We undertook a number of measures to effect blinding and minimize the risk of bias. The clinical doctor performing different anesthesia mode and observing the patient were blinded to the group allocation. Data collection was done by the same doctor who was unaware of the group allocation. Patients were provided with trial details sufficient to allow for informed consent, but they didn’t know the study outcomes or the hypotheses of the investigators. The research assistant was provided relevant details to facilitate recruitment, consent of patients, and coordination of testing. While the randomization schedule was concealed, the research assistant could not be blinded to participant assignment due to the nature of the intervention. It is conceivable that the research assistant was aware of the purpose of the trial, although there were no conflicts of interest with respect to study outcomes. How to chose the method of anesthesia? It depends on clinical doctor's experiences and preferences based on relative safety as possible. Sometimes GA is a remedial measure. GA was induced in rapid sequence, with Sellick maneuver and the administration of propofol, remifentanil, and succinylcholine. Intubation was performed by video laryngoscopy, and anesthesia was maintained with sevoflurane and remifentanil. Epidural puncture was carried out in the following conditions: sudden decrease in pressure during needle insertion; catheter inserted with ease and without resistance; sufficient and definite epidural analgesia without subdural- and subarachnoid blocks. A test dose of 4 mL 2% lidocaine was administered through the epidural catheter, and followed 5 minutes later by an initial loading dose of 8 mL 2% lidocaine. Combined spinal-epidural anesthesia was administered by inserting a standard lumbar anesthesia needle (E/SII Single-use Puncture set for Local Anesthesia, Shanghai Shangyi Kangge Medical Instrument Co. Ltd, Shanghai, People's Republic of China) into the subarachnoid space before catheter insertion into the epidural space of L2,3 or L3,4. Success of this method was reflected by the cerebrospinal fluid flowing from the spinal needle's hub, and anesthesia was induced by a bolus infusion of 0.5% bupivacaine (1.5–2 mL). Then, the spinal needle was pulled out and the catheter inserted into the epidural space. After confirming correct placement with a test dose, 2% lidocaine was maintained by intermittent infusion (6–9 mL/45 min). For operational needs, oxygen saturation was maintained above 98%, and a bolus dose of phenylephrine (100 μg) or ephedrine (6 mg) was administered as needed, to maintain a target mean arterial pressure of 70 mmHg.
GA was carried out by intravenous propofol at 2.0 to 2.5 mg/kg, remifentanil at 1 μg/kg and suxamethonium at 1.5 to 2 mg/kg; intubation in rapid sequence induction was administered, with delivery to the fetus within 10 minutes of anesthesia. Then, the operation was completed under anesthesia maintenance with sevoflurane, remifentanil, and cisatracurium at 2 to 4 mg.
In EA, after completing epidural puncture in 2% lidocaine to maintain anesthesia, we ensured a sensory block up to T6 level and a lidocaine consumption of 12 to 15 mL.
For combined spinal-epidural anesthesia (CSEA), lumbar anesthesia combined needle was administrated in the L2 to L3 or L3 to L4 interspace in the CSEA group, with an initial spinal dose of 0.5% bupivacaine 7.5 mg. Then, epidural catheters were placed into the epidural space, ensuring a sensory block up to T6 level at a minimum, with additional epidural infusion if needed.
2.3. Intraoperative monitoring
The following pregnancy outcomes were evaluated: heart rate (HR), electrocardiography (ECG) data, systolic arterial blood pressure (SAP), diastolic arterial pressure (DAP), mean aortic pressure (MAP), and pulse oxygen saturation (SPO2). Constant supply of oxygen (3 L/min) was performed in all patients. The numbers of patients referred to emergency care were recorded as well as those with fetal macrosomia (birth weight >4000 g), gestational diabetes mellitus (GMD, elevated glucose challenge test and at least 2 abnormal values in the glucose tolerance test), CS history, fetal distress, age ≥35 years, prenatal fever, arrhythmias, heart abnormalities, gestational hypertension (blood pressure 140/90 mmHg without evidence of chronic hypertension), preeclampsia (criteria for gestational hypertension and significant proteinuria), multiple pregnancy, precious child, amniotic fluid abnormality, large amounts of bleeding, neonate Apgar score (1 min), and Apgar score (5 min). The numbers of EA, GA, post-anesthesia care unit (PACU), and intensive care unit (ICU) patients were recorded for the duration of hospital stay and anesthesia puncture times (n) of 5 > n ≥ 3 and n ≥ 5 in the non-obesity, severe obesity, and morbid obesity groups. In addition, we also recorded the numbers of puncture patients in the sitting position in all groups.
2.4. Statistical analyses
The SPSS 17.0 software (IBM Analytics, Armonk, NY, 10504-1722) was used for analysis. Women with BMI <30 were used as the non-obesity group. Data were tested for normality. Assuming normal distribution, student t test (2-tailed) was used to compare continuous data, and Chi-squared or Fisher exact test was used for categorical data. BMI, Apgar score, and bleeding amounts are mean ± standard deviation (SD), and assessed by analysis of the variance (ANOVA). P < .05 was considered statistically significant.
3. Results
Between January 1, 2013 and September 30, 2016, a total of 892 women were assessed for eligibility, and 810 women received allocated interventions (Fig. 1). The experimental records were lost for 5 women of the morbid obesity group, 6 of the severe obesity group, and 9 of the non-obesity group (Fig. 1). A total of 790 patients finally completed the protocol. Anesthetic and obstetric outcome variables were extracted from medical records and analyzed.
Figure 1.
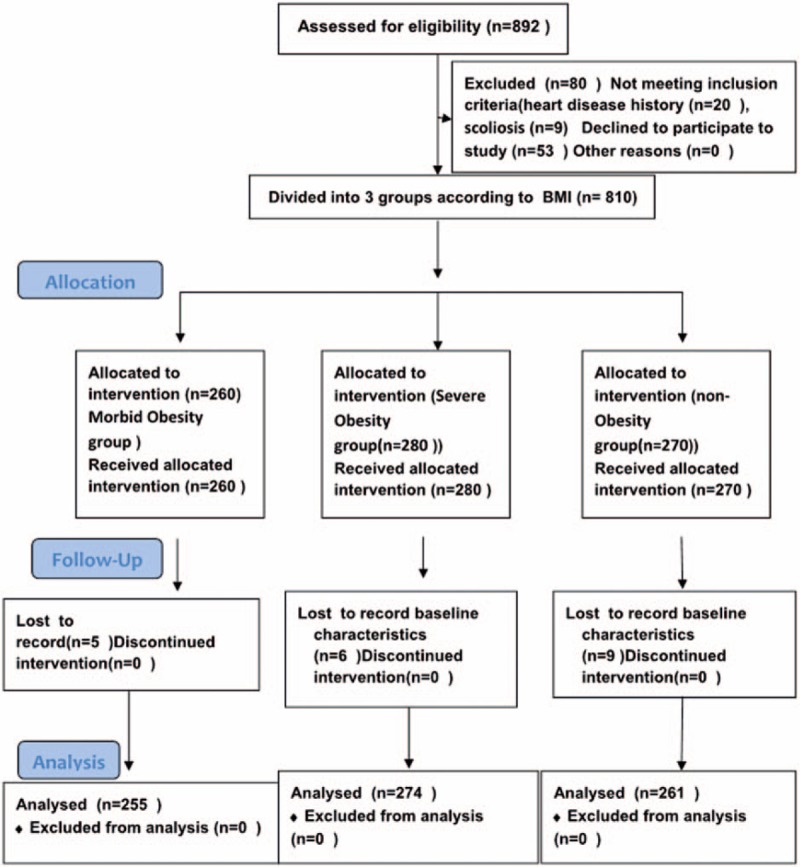
Between January 1, 2013 and September 30, 2016, a total of 892 women met inclusion criteria, including 810 women received allocated intervention (Fig. 1). The medical records of 5, 6, and 9 women were lost in the morbid obesity, severe obesity, and non-obesity groups, respectively. A total of 790 patients completed the protocol, and 20 women did not complete it for missing baseline characteristics.
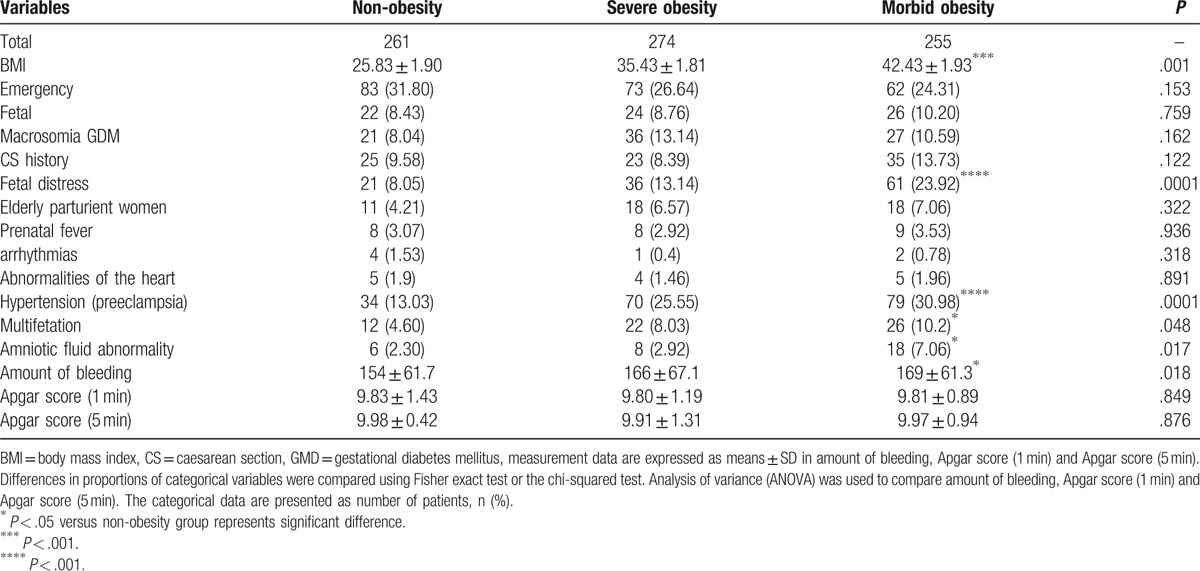
Baseline data for the women who completed the protocol are shown in Table 1. Clinically, mean birth weights were similar among control, obese, and morbidly obese patients. Compared with the non-obesity group, significantly more fetal distress and higher BMI was found in the morbid obesity group (P = .0001 and P = .001, respectively). Significantly more patients had preeclampsia, multifetation, amniotic fluid abnormality, and large bleeding amounts in the morbid obesity group compared with the non-obesity group (P = .0001, P = .048, P = .017, and P = .018, respectively). Among the 3 groups, there were no obvious differences in emergency room care, fetal macrosomia, GDM, CS history, age of parturient women, prenatal fever, arrhythmias, heart abnormalities, multifetation precious child, amniotic fluid abnormality, Apgar score (1 min) and Apgar score (5 min).
Table 1.
Baseline characteristics of the patients for 3 groups.
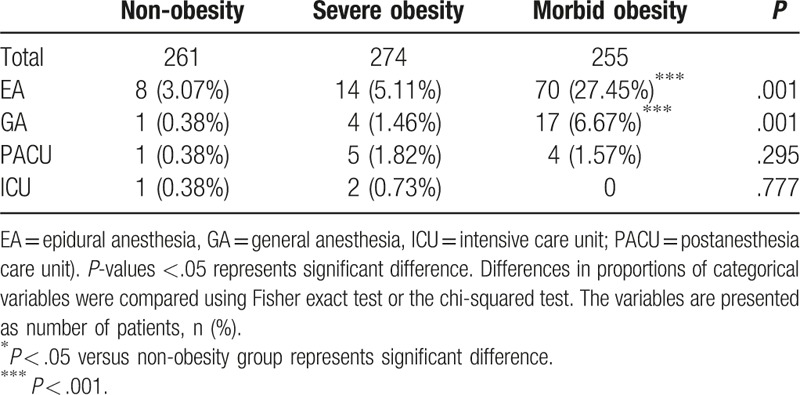
Compared with the non-obesity group, there were significantly more patients that underwent epidural anesthesia and GA in the morbid obesity group (P = .0001 and P = .0001, respectively). In the morbid obesity and severe obesity groups, the proportion of PACU patients was no more than that of the non-obesity group. Among the 3 groups, there were no significant differences in the percentage of ICU patients (P = .777). These data are summarized in Table 2.
Table 2.
Different anesthesia modalities in the 3 groups.
Compared with the non-obesity group, there were significantly more anesthesia puncture times of 5 > n ≥ 3 and n ≥ 5 in the morbid obesity group (P = .0001 and P = .0001, respectively), as shown in Table 3. In addition, significantly more patients in the puncture sitting position were found in the morbid obesity or severe obesity group than in non-obesity women (P = .0001).
Table 3.
Intraspinal anesthesia puncture numbers in 3 groups.

4. Discussion
This work primarily assessed the effects and risks of anesthetic techniques on fetomaternal outcomes in obese patients undergoing CS in a tertiary care teaching hospital in Shanghai. In this study, clinical doctors also assessed whether neuraxial anesthesia or GA is safe and effective in morbidly obese parturient women. It is known that choice of suitable anesthetic methods contributes in guaranteeing the safety of mother and fetus. It is obviously not convenient for clinical doctor to treat patients showing respiratory complications, with puncture and intubation difficulties in obese patients during the perioperative period. Previous studies showed that obesity is associated with higher maternal age,[1,3] higher parity,[2,3] and preexisting medical conditions.[3]
In this prospective cohort study, we further demonstrated that there were significantly more patients suffering from fetal distress in the morbid obesity group compared with non-obesity individuals. Many pregnant women with morbid obesity were more prone to hypoxia and breathing difficultly, which partially explain fetal distress. Significantly more patients suffered from multifetation and amniotic fluid abnormality in the morbid obesity group compared with non-obese women. Meanwhile, more patients had preeclampsia in obese parturient cases than controls; there was a higher incidence rate of patients with preeclampsia in the morbid obesity group. In the non-obesity group, bleeding amounts were decreased compared with those of the morbid obesity group. Previous findings showed that blood loss during CS in morbidly obese women is expectedly greater than in normal-weight women. In this group of women, blood loss of >1000 mL was 34.9% versus 9.3% in non-obese women,[5] corroborating the current study.
Meanwhile, in our study, the morbid obesity group showed no obvious differences in emergency, fetal macrosomia, GDM, CS history, age of parturient women, prenatal fever, arrhythmias, heart abnormalities, multifetation precious child, amniotic fluid abnormality, Apgar score (1 min) and Apgar score (5 min) in comparison with the non-obesity group.
We further demonstrated that women were not more likely to develop pregnancy-induced complications such as GMD, prenatal fever, and amniotic fluid abnormality in the morbid obesity group compared with non-obese patients. However, these results could be changed by larger sample size, and there were no significant differences in CS history, emergency CS, fetal macrosomia, age of parturient women, arrhythmias, heart abnormalities, multiple pregnancy, and precious child in the morbid obesity group in comparison with non-obese women.
A previous study showed that obesity is an independent risk factor for adverse obstetric outcome and significantly associated with increased cesarean delivery rate.[6] Wataba et al[7] found that patients with a prepregnancy BMI ranging from 18 to 23.9 have the least pregnancy related complications. Meanwhile, underweight women show a higher risk of low birth weight infants, which increases the rate of infant hospitalization.[8] Larsen et al[9] showed that the frequency of macrosomia increases with a high BMI. The risk of macrosomia depends not only on the prepregnancy BMI[10] but also on weight gain during pregnancy.[11]
In our study, there were significantly more patients that underwent epidural and GA in the morbid obesity group compared with the non-obesity group. In the morbid obesity group, PACU patients were more than those of the severe obesity and non-obesity groups. In this study, placement of epidural catheter in morbidly obese patients was technically challenging. There were more anesthesia puncture times in morbidly obese patients compared with the non-obesity group. Just as CS took an extended period of time, the initiation time of anesthesia was also increased compared with non-obese parturient patients. According to the ASA Practice Guidelines for Obstetric Anesthesia,[12] the decision to choose a particular anesthetic technique should be individualized and based on anesthetic, maternal, and fetal risk factors, maternal preferences, and the clinical doctor's judgement. It is known that early or threatened labor, antepartum hemorrhage, emergency CS, previous CS, and preeclampsia are significant determinants of GA in CS deliveries, and spinal anesthesia is the most common mode of anesthesia for CS deliveries in Taiwan.[13]
This study found no significant differences in Apgar score (1 min) and Apgar score (5 min) for the morbid obesity group compared with non-obese patients. Ajuzieogu et al[14] and Moodley et al[15] found similar neonatal outcomes irrespective of anesthesia administered; in addition, Ajuzieogu et al[14] showed that maternal mortality rates are similar after spinal and GA modes. GA should be preferred, as well as spinal anesthesia combined with epidural anesthesia, which has quick onset with very short time of fetus disengagement and high Apgar score.
There were significantly more anesthesia puncture times of 5 > n ≥ 3 and n ≥ 5 in morbidly obese patients compared with the non-obesity group. Significantly more patients in the puncture sitting position were found in the obese patients compared with the non-obesity group. The risk of difficult intubation increased in obese patients. Neuraxial techniques are the preferred anesthetic techniques for CS in obese parturient women, and can be technically challenging,[16] since maternal airway management is very difficult. The physiological changes of pregnancy cause airway oedema, difficult positioning, reduced oxygen reserves, and increased oxygen consumption. Many unsuccessful attempts to endotracheal intubation can worsen airway management so that facemask ventilation becomes impossible, and could lead to disability or death cases. Therefore, there might be qualitative or quantitative deficiency in hormonal regulation of labor in morbidly obese parturient women. More research is required to better understand the effects of morbid obesity on labor. Obese patients should be monitored carefully in the postoperative period, because of increased risk of postoperative complications in morbidly obese parturient women.[16,17]
Local and general anesthetic modalities for cesarean section in morbidly obese parturient women are associated with increased maternal and perinatal complications.[18] A previous study demonstrated that morbidly obese parturient women have an increased likelihood for initial failed epidural, subsequent epidural replacement, inadvertent dural puncture, and cesarean section, with difficult intubation under emergent conditions.[18]
Previous findings revealed that early preoperative assessment, epidural insertion, and replacement for failed local anesthesia/analgesia, along with GA preparation and difficult airway intubation, could decrease potential complications in morbidly obese parturient women.[18] Obviously, obesity caused increased puncture difficulty with more patients adopting the sitting position. The incidence of nerve injury is 0.10% to 0.27% in the Department of Obstetrics, and 0.34% to 0.58% after intraspinal anesthesia in Western countries[19–21]; this remains unclear and underreported in China. Large studies assessing anesthetic outcome in morbidly obese parturient women are lacking. The current study evaluated anesthetic and obstetric outcomes in morbidly obese and matched control parturient women; parturient patients showed no obvious neural complications. The optimal anesthetic technique for CS in women with severe preeclampsia remains controversial. Local and regional anesthesia modalities are equally acceptable for CS in morbidly obese women. Staikou et al[22] showed that neonatal oxygenation and acid–base statuses are better preserved when GA is administered for CS in comparison with regional anesthesia; Apgar scores and neonatal outcomes were not affected by the anesthetic technique. CSEA has become an increasingly popular anesthetic technique for repeated cesarean sections.[23] We think that GA should be preferred, as well as spinal anesthesia combined with epidural anesthesia, which has quick onset with very short time of fetus disengagement and high Apgar score. We can choose them according to clinical situation and obese patient's breath difficulty level, fetal risks, and the clinical doctor's experiences.
However, a previous study showed that the advantages of this intraspinal technique are not routinely made available to morbidly obese patients because of the lack of appropriately long needles.[23] Post-anesthesia monitoring and management also require specific nursing expertize; postoperative complications, including hypoventilation and hemodynamic collapse have been described.[24] Interestingly, obstetric surgery has emerged as a global health priority; morbidly obese pregnant women with BMI >40 kg/m2 are at increased risk of pregnancy complications and significantly increased CS rate. Preanesthetic evaluation and scheduled cesarean is optimal but not always possible, and it is very critical for clinical doctor to ensure the safety of mothers and infants.[25,26] Women with a BMI >50 kg/m2 have much greater risk for cesarean wound complications. Avoidance of subcutaneous drains and increased use of transverse abdominal wall incisions should be considered in massively obese parturient patients to reduce operative morbidity.[27] Compared with control patients, initial epidural anesthesia failure was significantly more likely in morbidly obese women, requiring epidural catheter replacement. Previous studies showed that morbidly obese women have a higher rate of epidural anesthesia failure, and are likely to have difficult intubation. Inability to recognize landmarks, difficulty in implementing regional block, and erratic spread of the anesthetic solution contribute to the elevated failure rate.[28–30] This leads to elevated incidences of antepartum medical disease, prolonged CS operation times, serious postoperative complications, and long hospital stays. Epidural anesthesia is feasible; however, the high initial failure rate necessitates early catheter placement, critical block assessment, and catheter replacement when indicated, as well as provision for alternative airway management.[31] Keerath and Cronje[32] demonstrated that spinal anesthesia is a preferred anesthetic technique for CS in patients with severe preeclampsia (see Supplemental Digital Content, S1 File. Informed consent in English.(Doc), S2 File. Clinical studies checklist in English.(Doc); ).
There are several limitations associated with the study. First, it was a prospective cohort single-center trial, and a multicenter prospective trial is more convincing to verify the safety and risk of various perioperative anesthetic methods in obese women undergoing CS delivery. Secondly, we only assessed nulliparous patients, with other patients group were not included, for example, pluriparas and gemelliparas, and sample composition might have affected the research results. Thirdly, umbilical cord blood of the fetus was not assessed, which can help evaluate clear neonatal oxygenation and the acid–base status, this variable should be included in future study protocols.
In summary, the 3 anesthesia modalities were safe and effective in severely or morbidly obese patients. There were more patients suffering from fetal distress in the morbid obesity group. Many pregnant women with morbid obesity were more prone to hypoxia and breathing difficultly, which partially explain fetal distress. There were more intraspinal anesthesia puncture times in morbidly obese patients. Therefore, caution should be used to further explore the perioperative safety if larger data for obese patients and multicenter interpretation of the aforementioned situations are intended.
Supplementary Material
Acknowledgments
The authors would like to thank all nurses of the operation room of our hospital for assisting in patients recruitment. We gratefully acknowledge financial support from the Youth Talent Fund from International Peace Maternity and Child Health Hospital, Shanghai Jiao Tong University, School of Medicine (2014), and the Perinatal Potential Subject (To International Peace Maternity and Child Health Hospital, Shanghai Jiaotong University School of Medicine).
Footnotes
Abbreviations: BMI = body mass index, CS = cesarean section, CSEA = combined spinal-epidural anesthesia, EA = epidural anesthesia, GA = general anesthesia, PACU = post-anesthesia care unit.
Authors’ contributions: All authors contributed significantly to both the study and manuscript.
Study supervision: WC, ZY; Study design: ZY, XA; Data collection: XA,YZ.
Data analysis: QY, YZ; Data interpretation: YW, XA, ZY; Writing of manuscript: ZY, XA; Review of manuscript: ZY, WC.
Funding: The Youth Talent Fund from International Peace Maternity and Child Health Hospital, Shanghai Jiao Tong University, School of Medicine (2014) and the Perinatal Potential Subject (to the International Peace Maternity and Child Health Hospital, Shanghai Jiaotong University School of Medicine).
Competing financial interests: The authors declare no competing financial interests.
Clinical Trial Registration: This clinical study has been registered at http://clinicaltrials.gov/ct2/show/NCT03002636 (NCT03002636).
The authors have no conflicts of interest to disclose.
Supplemental Digital Content is available for this article.
References
- [1].Donohoe CL, Feeney C, Carey MF, et al. Perioperative evaluation of the obese patients. J Clin Anesth 2011;23:575–86. [DOI] [PubMed] [Google Scholar]
- [2].Lemmens HJ. Perioperative pharmacology in morbid obesity. Curr Opin Anaesthesiol 2010;23:485–91. [DOI] [PubMed] [Google Scholar]
- [3].Simas TA, Liao X, Garrison A, et al. Impact of updated Institute of Medicine guidelines on prepregnancy body mass index categorization, gestational weight gain recommendations, and needed counseling. J Womens Health (Larchmt) 2011;20:837–44. [DOI] [PubMed] [Google Scholar]
- [4].Bader AM. Chestnut D. Neurologic and neuromuscular diseases. Obstetric Anesthesia: Principles and Practice 3rd ed.Pennsylvania: Elsevier Mosby; 2004. 872–91. [Google Scholar]
- [5].Perlow JH, Morgan MA. Massive maternal obesity and perioperative cesarean morbidity. Am J Obstet Gynecol 1994;170:560–5. [DOI] [PubMed] [Google Scholar]
- [6].Weiss JL, Malone FD, Emig D, et al. Obesity, obstetric complications and cesarean delivery rate—a population-based screening study. Am J Obstet Gynecol 2004;190:1091–7. [DOI] [PubMed] [Google Scholar]
- [7].Wataba K, Mizutani T, Wasada K, et al. Impact of prepregnant body mass index and maternal weight gain on the risk of pregnancy complications in Japanese women. Acta Obstet Gynecol 2006;85:269–76. [DOI] [PubMed] [Google Scholar]
- [8].Murakami M, Ohmichi M, Takahashi T, et al. Prepregnancy body mass index as an important predictor of perinatal outcomes in Japanese. Arch Gynecol Obstet 2005;271:311–5. [DOI] [PubMed] [Google Scholar]
- [9].Larsen CE, Serdula MK, Sullivan KM. Macro-somia: influence of maternal overweight among a low-income population. Am J Obstet Gynecol 1990;162:490–4. [DOI] [PubMed] [Google Scholar]
- [10].Sebire NJ, Jolly M, Harris JP, et al. Maternal obesity and pregnancy outcome: a study of 287 213 pregnancies in London. Int J Obes Relat Metab Disord 2001;25:1175–82. [DOI] [PubMed] [Google Scholar]
- [11].Johnson JW, Longmate JA, Frentzen B. Excessive maternal weight and pregnancy outcome. Am J Obstet Gynecol 1992;167:353–70. [DOI] [PubMed] [Google Scholar]
- [12].American Society of Anesthesiologists Task Force on Obstetric Anaesthesia. Practice guidelines for obstetric anesthesia: an updated report by the American Society of Anesthesiologists Task Force on Obstetric Anesthesia. Anesthesiology 2007;106:843–63. [DOI] [PubMed] [Google Scholar]
- [13].Lai HY, Tsai PS, Fan YC, et al. Anesthetic practice for Caesarean section and factors influencing anesthesiologists’ choice of anesthesia: a population-based study. Acta Anaesthesiol Scand 2014;58:843–50. [DOI] [PubMed] [Google Scholar]
- [14].Ajuzieogu OV, Ezike HA, Amucheazi AO, et al. A retrospective study of the outcome of cesarean section for women with severe pre-eclampsia in a third world setting. Saudi J Anaesth 2011;4:15–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Moodley J, Jjuuko G, Rout C. Epidural compared with general anaesthesia for caesarean delivery in conscious women with eclampsia. Br J Obstet Gynaecol 2001;108:378–82. [DOI] [PubMed] [Google Scholar]
- [16].Lamon AM, Habib AS. Managing anesthesia for cesarean section in obese patients: current perspectives. Local Reg Anesth 2016;16:45–57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Garabedian MJ, Williams CM, Pearce CF, et al. Extreme morbid obesity and labor outcome in nulliparous women at term. Am J Perinatol 2011;28:729–34. [DOI] [PubMed] [Google Scholar]
- [18].Vallejo MC. Anesthetic management of the morbidly obese parturient. Curr Opin Anaesthesiol 2007;20:175–80. [DOI] [PubMed] [Google Scholar]
- [19].Allison CL, Howell S. Neurological complications in obstetric regional anaesthesia. Anesth Intensive Care Med 2013;8:331–2. [Google Scholar]
- [20].Kowe O, Waters JH. Neurologic complications in the patient receiving obstetric anesthesia. Neurol Clin 2012;30:823–33. [DOI] [PubMed] [Google Scholar]
- [21].Sviggum HP, Jacob AK, Arendt KW, et al. Neurologic complications after chlorhexidine antisepsis for spinal anesthesia. Reg Anesth Pain Med 2012;37:139–44. [DOI] [PubMed] [Google Scholar]
- [22].Staikou C, Tsaroucha A, Vakas P, et al. Maternal and umbilical cord oxygen content and acid-base balance in relation to general, epidural or subarachnoid anesthesia for term elective cesarean section. Clin Exp Obstet Gynecol 2013;40:367–71. [PubMed] [Google Scholar]
- [23].Kuczkowski KM, Benumof JL. Repeat cesarean section in a morbidly obese parturient: a new anesthetic option. Acta Anaesthesiol Scand 2002;46:753–4. [DOI] [PubMed] [Google Scholar]
- [24].Mhyre JM, Riesner MN, Polley LS, et al. A series of anesthesia-related maternal deaths in Michigan, 1985–2003. Anesthesiology 2007;106:1096–104. [DOI] [PubMed] [Google Scholar]
- [25].Sobhy S, Zamora J, Dharmarajah K, et al. Anaesthesia-related maternal mortality in low-income and middle-income countries: a systematic review and meta-analysis. Lancet Glob Health 2016;4:e320–7. [DOI] [PubMed] [Google Scholar]
- [26].Machado LS. Cesarean section in morbidly obese parturients: practical implications andcomplications. N Am J Med Sci 2012;4:13–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Alanis MC, Villers MS, Law TL, et al. Complications of cesarean delivery in the massively obese parturient. Am J Obstet Gynecol 2010;203:271.1–7. [DOI] [PubMed] [Google Scholar]
- [28].Endler GC. The risk of anesthesia in obese parturients. J Perinatol 1990;10:175–9. [PubMed] [Google Scholar]
- [29].Vricella LK, Louis JM, Mercer BM, et al. Anesthesia complications during scheduled cesarean delivery for morbidly obese women. Am J Obstet Gynecol 2010;203:e1–5. [DOI] [PubMed] [Google Scholar]
- [30].Whitty RJ, Maxwell CV, Carvalho JC. Complications of neuraxial anesthesia in an extreme morbidly obese patient for Cesarean section. Int J Obstet Anesth 2007;16:139–44. [DOI] [PubMed] [Google Scholar]
- [31].Hood DD, Dewan DM. Anesthetic and obstetric outcome in morbidly obese parturients. Anesthesiology 1993;79:1210–8. [DOI] [PubMed] [Google Scholar]
- [32].Keerath K, Cronje L. Observational study of choice of anaesthesia and outcome in patients with severe preeclampsia who present for emergency caesarean section. Southern Afr J Anaesth Analg 2012;4:206–12. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.