

Abstract
Background and Objectives
CDC guidelines recommend follow-up within 72 hours of diagnosis of pelvic inflammatory disease (PID) because patients with inadequate treatment are at increased risk of acute and chronic complications. Follow-up rates in adolescents after diagnosis range between 10 to 16%. The primary objective was to assess the effect of text message (TM) reminders to adolescent patients diagnosed with PID on obtaining follow-up care within 72 hours of emergency department (ED) discharge.
Methods
Single-blinded, randomized controlled trial of adolescents diagnosed with PID in the ED. Patients received standard discharge instructions or standard discharge instructions plus TM reminders. Patients in the TM group received daily, tailored TM for 4 days with a reminder to schedule and attend PCP follow-up. The primary outcome was follow-up within 72 hours of ED discharge.
Results
95 patients (48 standard; 47 TM) were randomized. 3 patients were excluded, leaving 92 patients (46 standard; 46 TM) for analysis. Baseline characteristics were similar between treatment groups. Follow-up was 15.2% in the standard group and 43.5% in the TM group. Patients receiving TM reminders were more likely to follow-up compared to the standard group (RR: 2.9; 95% CI 1.4–5.7). The absolute efficacy difference was 28.3% (95% CI 9.5–46.9) yielding NNT of 4 (95% CI 2.2–9.5).
Conclusion
Personalized TM reminders were efficacious in improving follow-up for adolescents after ED diagnosis of PID.
INTRODUCTION
Pelvic inflammatory disease (PID) affects as many as 10% of adolescent females and results in long-term complications such as infertility and chronic pelvic pain for up to 40% of these women.1,2 Adequate treatment and prevention of repeated episodes reduces the risk of these sequelae. Therefore, the Centers for Disease Control (CDC) recommends follow-up within 72 hours of diagnosis of PID to ensure clinical improvement, review safe sexual practices, and reinforce the importance of partner treatment and medication compliance.3 This follow-up appointment is particularly important for adolescents who commonly receive the diagnosis of PID in emergency departments (ED) or urgent care centers where time constraints result in limited counseling at the time of diagnosis.4,5 Unfortunately, with follow-up rates as low as 10–16%, the majority of adolescents diagnosed with PID are not receiving the recommended follow-up care, which likely contributes to the high rates of long-term complications.6,7
Lack of recommended post-ED follow-up care extends beyond patients with PID. ED providers do not provide ongoing care to patients and therefore routinely recommend follow-up with primary care providers (PCP) to ensure improvement from acute ED presentation and for ongoing management of chronic conditions. There are numerous reasons cited for patients not receiving post-ED follow-up care including lack of transportation, limited time, provider availability, and lack of perceived benefit or need.8 Interventions to improve post-ED follow-up for children and adolescents have included telephone reminders, mailed reminders, and ED providers scheduling outpatient appointments, all with limited success.8,9 One recent study in adults demonstrated improvement in follow-up rates when appointments were scheduled prior to ED discharge and patients were reminded via text message (TM) reminder the following day.10
Text messaging is used socially by the majority of adolescents and can be read privately at a convenient time, making TM a potentially ideal technology to remind patients of follow-up relating to sensitive health care issues such as PID.11,12 Prior studies have demonstrated that TM interventions are successful in promoting behavior change, improving medication compliance, and improving self-management of some chronic diseases.13–18 The primary aim of this study was to test the effect of TM reminders on adolescent patients’ adherence to the recommended post-ED follow-up visit. We hypothesized that TM reminders would improve post-ED follow-up care. The secondary aims of this study were to evaluate the feasibility of using TM reminders after ED discharge; to identify patient characteristics that are associated with follow-up; and to evaluate barriers to post-ED follow-up. Patient characteristics explored included presence of high risk behaviors and illness severity. Illness severity was as defined presence of abdominal pain, pelvic pain, or performance of abdominal imaging because abdominal imaging is generally performed on patients with more severe symptoms to exclude complications or alternative diagnoses.
METHODS
This was a single-blinded, randomized controlled trial to test the effectiveness of TM reminders in improving PCP follow-up rates in adolescent females diagnosed with PID in the ED. This study was approved by our Institutional Review Board and was registered with clinicaltrials.gov (NCT01299259).
Study Sample and Group Randomization
Patients were enrolled from an urban academic pediatric ED with an annual census of 90,000 patients between February 2012 and August 2014 when sample size goal enrollment was achieved. Adolescent females ≥ 15 years of age were eligible if they were diagnosed in the ED with PID and were determined by the attending physician to be appropriate for outpatient treatment. PID was defined using the 2006 CDC minimum criteria for PID diagnosis: lower abdominal pain or pelvic pain with no other cause identified with the presence of either cervical motion tenderness, uterine tenderness, or adnexal tenderness.3 Presence of these criteria were verified by the attending pediatric emergency medicine physician by being present during the exam or performing the exam prior to patient enrollment. Patients were excluded if they did not have a cell phone with TM capability, had a developmental disability, were non-English speaking, were pregnant, or were previously enrolled in the study. Non-English speaking patients were excluded because of the multiple points of contact requiring translation, including consent procedures, interviews in the ED, and telephone interviews. Pregnant patients were transferred to another hospital with obstetrical services for further care in accordance with our institutional policy, making them ineligible for the study. A patient log was kept during the study period to document patients screened and the reasons for exclusion.
Study Procedure
Patients meeting inclusion criteria were identified by research assistants by reviewing the ED tracking board during the hours of 8 AM and midnight, 7 days a week. Adolescent females presenting with chief complaints related to abdominal, genitourinary, or infectious symptoms were screened. Inclusion and exclusion criteria were then verified by the ED clinician caring for the patient prior to study staff approaching the patient for enrollment. In accordance with Pennsylvania state law and hospital policy, adolescents are permitted to consent to testing and treatment for sexually transmitted infections without parental consent and therefore were able to consent to participate in the study without parental consent. In addition, only verbal consent was obtained from patients due to the increased risk for a breach in confidentiality with a written consent form. During consent, study staff explained that the TM were uni-directional and emphasized that patients would not be able to communicate with providers via TM. After providing verbal informed consent, participants completed a written questionnaire (appendix 1) assessing demographic characteristics, experience with TM and cells phones, previous primary care experience, and sexual history. The questionnaire was developed by investigators by adapting the National Survey of Family Growth19 and the Parent and Teen Cell Phone Survey conducted by the Pew Research Center20 and was pilot tested for clarity with 10 patients meeting inclusion criteria prior to study initiation. Based on this feedback, the wording of a few items was clarified. Study staff administered a brief verbal survey to collect PCP name and contact information as well as patient cell phone number for a follow-up survey. All study participants provided written permission to verify follow-up. Following completion of the questionnaires, study staff then assigned patients to the intervention or control group by using a series of numbered, opaque envelopes that contained the randomization assignment that was predetermined by a computer generated randomization system. Both the control and intervention groups received standard written discharge instructions on PID which included instructions for PCP follow-up within 3 days of discharge. If a patient did not have a PCP or did not feel comfortable seeking follow-up care with her PCP for this illness, she was referred to the adolescent clinic affiliated with our institution per usual practice. The adolescent clinic accommodates patients diagnosed with PID in the ED for follow-up under the Federal Title X family planning program. Contact information for the adolescent clinic was included in standard discharge paper work. Prior to discharge, all participants received a 5 dollar gift card for their participation. After receiving standard written discharge instructions from the medical providers who were blinded to treatment allocation, patients were discharged home for standard outpatient treatment. As part of the ED’s standard discharge procedure, a faxed copy of the patient’s ED record was sent to the PCP once the physician note was completed.
The control group did not receive any additional reminders to follow-up. The intervention group received a total of 4 text messages to remind them to schedule and attend a follow-up appointment. TM were personalized with patient first name, PCP name, PCP phone number, and recommended time frame for follow-up. Study staff entered this information into a secure online-service (Remedy Health Media, New York, NY) prior to discharge from the ED. This system automatically sent TM reminders without further action of study staff on study days 2, 3, 4, and 5. The first TM was structured as follows: “Hi Mary, Please call 888-888-8888 now to make an appointment with Dr. X by Friday. This is important to make sure you are improving.” Messages were designed to include information essential to making the appointment while not revealing any potentially sensitive information such as diagnosis. Subsequent text messages also included the number of the adolescent clinic in case a patient was unable to schedule an appointment with her PCP. To minimize school interruption and maximize the patient’s opportunity to call during business hours to make an appointment, messages were sent after school hours between 3:30 PM and 4:30 PM on weekdays and at 10 AM on weekend days. Text message delivery status (received or failed) was recorded by the online system.
Study staff blinded to treatment group contacted the PCP of each patient within 2 weeks of her ED visit to verify follow-up visit. For patients who did not have a follow-up appointment with their PCP or who did not have a PCP on enrollment, we performed a review of the electronic medical record to determine if they received follow-up in the adolescent clinic. To evaluate our secondary outcomes, text message delivery logs were reviewed and all study participants were contacted by telephone 2 weeks after the ED visit for a standardized telephone survey regarding barriers to follow-up and, if applicable, Likert-scale based questions on experience with TM reminders. Barriers to follow-up were ascertained through open-ended questions that were then categorized by study staff using predetermined criteria. Patients receiving TM were also queried regarding any inconveniences that the TM caused.
Sample Size
Using a baseline follow-up rate of 10% based on prior published studies, we estimated that a sample size of 94 (47 patients in each arm) would allow 85% power to detect an increase of 25% (from 10% to 35%) in the follow-up rate. A 25% increase in follow-up was deemed as clinically significant by expert consensus. Sample size was calculated using STATA 12 (STATA, College Station, TX).
Data Analysis
We conducted both an intention-to-treat (ITT) and per-protocol analysis of the data. ITT analysis included all patients as originally allocated after randomization and was conducted for all outcomes to reflect the likely real-world conditions of discontinued cell phones and phone numbers incorrectly entered. Per-protocol analysis was conducted for the primary outcome to compare the patients who completed the treatment as originally allocated. Group differences were determined by using the two-sample t-test or Mann-Whitney U test for continuous variables and chi-square test or Fisher’s exact test to compare intervention and control groups. Univariate logistic regression was performed to determine whether there was a significant association between each of the predefined patient variables and the outcome. Statistical analysis was performed using Stata version 13.1 (Stata Corp, College Station, TX).
RESULTS
Of the 2,863 adolescent women screened for eligibility, 95 met eligibility requirements, consented and were randomized. (Figure 1). Three patients were excluded from analysis because PCP verification could not be obtained leaving 92 patients (46 standard; 46 TM) for analysis. Baseline characteristics were similar between treatment groups including markers of illness severity and prior PCP experience (Table 1).
Figure 1.
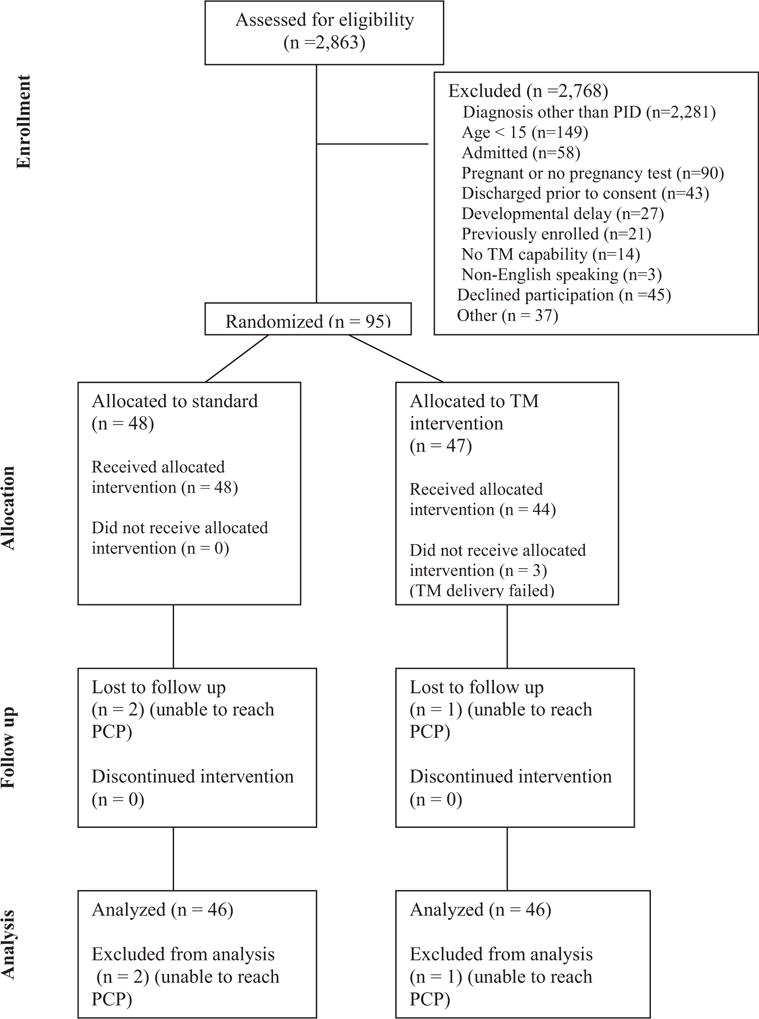
CONSORT diagram. Improving pelvic inflammatory disease follow-up from the ED: randomized controlled trial with textmessages. PID, Pelvic inflammatory disease; TM, text message; PCP, primary care provider.
Table 1.
Baseline demographics
| TM (n=47) | Control (n=48) | Difference (95% CI) | |
|---|---|---|---|
| Age (mean) | 16.5 (95% CI: 16.4–17.1) | 17 (95% CI: 16.5–17.3) | 0.5 (−0.81 to −0.19) |
| Medicaid | 26 (55%) | 24 (50%) | 5 (−14 to 24) |
| Currently in School | 41 (87%) | 42 (87%) | 0 (−13 to 14) |
| Ethnicity | |||
| African American | 42 (89%) | 42 (87%) | 2 (−12 to 15) |
| Caucasian | 1 (2%) | 3 (6%) | 4 (−6 to 15) |
| Hispanic/Latino | 2 (4%) | 2 (4%) | 0 (−10 to 11) |
| Other | 2 (4%) | 1 (2%) | 2 (−7 to 12) |
| Pelvic pain | 47 (100%) | 45 (93%) | 7 (−2 to 17) |
| Abdominal pain | 47 (100%) | 46 (95%) | 5 (−4 to 14) |
| Abdominal Imaging Performed | 29 (62%) | 23 (48%) | 14 (−6 to 32) |
| Prior Experience with PCP | |||
| Has PCP | 40 (85%) | 45 (93%) | 8 (−4 to 22) |
| PCP visit in last year | 44 (93%) | 40 (83%) | 10 (−3 to 24) |
| Are you comfortable talking to your PCP about STI? | 42 (89%) | 43 (89%) | 0 (−13 to 14) |
| PCP visit for these symptoms prior to ED visit? | 13 (27%) | 13 (27%) | 0 (−17 to 18) |
| Do you want to follow-up with your PCP for this? | 41 (87%) | 40 (83%) | 4 (−11 to 18) |
PCP: Primary care provider STI: Sexually transmitted infection
In the ITT analysis, the post-ED follow-up rate was 43.5% (20/46) in the TM group compared to 15.2% (7/46) in the control group (Table 2). The absolute efficacy difference was 28.3% (95% CI 9.5–46.9) yielding a number needed to treat (NNT) of 4 (95% CI 2.2–9.5). Patients receiving TM reminders were more likely to follow-up compared to the standard group (RR 2.9; 95% CI 1.3–6.1). The per-protocol analysis also demonstrated similar results. In the per-protocol analysis, 3 patients were excluded after randomization because they did not receive text message reminders (1 entered incorrectly, 2 cell phone service discontinued) leaving 89 patients for analysis (46 standard; 43 TM). The follow-up rate in the per-protocol analysis was 46.5% (20/43) in the TM group compared with 15.2% (7/46) in the control group (RR 3.1; 95% CI 1.4–6.5). Overall, the majority of patients (19/27) that received follow-up care were seen by their PCP (Table 3). Univariate analysis was performed and demonstrated there were no individual characteristics such as severity of illness, prior experience with PCP, or high risk behaviors that were associated with likelihood to follow-up. Reasons for not following up with PCP were varied: unable to obtain appointment (22.9%), too busy (17.1%), symptoms improved (8.6%), lack of transportation (5.7%), or didn’t realize it was important (5.7%). There were no differences in barriers to follow-up between treatment groups.
Table 2.
Follow-up Care within 72 hours of ED Visit
| Intention to treat analysis | TM (n=46) | Control (n=46) | Relative Risk (95% CI) | NNT (95% CI) |
|---|---|---|---|---|
| Attended Follow-up | 20 (43.5%) | 7 (15.2%) | 2.9 (1.3 to 6.1) | 4 (2.2 to 9.5) |
| Per protocol analysis | TM (n=43) | Control (n=46) | ||
| Attended Follow-up | 20 (46.5%) | 7 (15.2%) | 3.1 (1.4 to 6.5) | 4 (2 to 7.5) |
Table 3.
Location of Follow-up Care
| Text Message Group | Control Group | |||||
|---|---|---|---|---|---|---|
| Has PCP | No PCP | Relative risk (95% CI) | Has PCP | No PCP | Relative risk (95% CI) | |
| Follow up care with PCP | 14 | 0 | 4.7 (0.32 to 68.9) | 5 | 0 | 0.7 (0.05–10.4) |
| Follow up care with Adolescent Clinic | 4 | 2 | 0.4 (0.9 to 1.8) | 1 | 1 | 0.07 (0.01 to 0.9) |
Feasibility of TM Reminders
Of the 2,863 patients who were screened for eligibility, only 14 were ineligible for not having a cell phone that could receive TM (0.5%). Daily TM was ubiquitous in the overall study population (Table 4). Based on the reports received from the TM service, a total of 188 TM were sent in this study and 162 (86%) were delivered successfully. Patients who received TM reminders found them convenient (88%), helpful (96%), and would recommend receiving TM reminders to their friends (88%). None of the patients receiving TM reminders reported any inconveniences associated with receiving TM reminders.
Table 4.
Prior Experience with Cell Phones
| TM (n=47) | Control (n=48) | Difference (95% CI) | |
|---|---|---|---|
| Who pays for cell phone | |||
| I pay for all of the costs | 14 (29%) | 14 (29%) | 0 (−17 to 19) |
| My parents pay some or all of the costs | 26 (56%) | 27 (56%) | 0 (−18 to 20) |
| Other | 6 (12%) | 5 (10%) | 2 (−11 to 16) |
| What kind of cell phone plan do you have? | |||
| A pre-paid or pay-as-you-go plan | 4 (8%) | 5 (10%) | 2 (−11 to 15) |
| A family plan (part of a contract that covers your family’s cell phones) | 20 (43%) | 21 (44%) | 1 (−18 to 20) |
| A separate contract covering only your cell phone | 17 (36%) | 18 (37%) | 1 (−18 to 20) |
| I don’t know what kind of plan it is | 6 (12%) | 4 (8%) | 4 (−9 to 18) |
| How old were you when you got your first cell phone? | |||
| Under 10 years | 6 (13%) | 2 (4%) | 9 (−3 to 21) |
| 10 | 5 (11%) | 9 (19%) | 8 (−7 to 23) |
| 11 | 10 (21%) | 8 (16%) | 5 (−11 to 20) |
| 12 | 9 (19%) | 10 (21%) | 2 (−15 to 18) |
| 13 | 8 (17%) | 8 (17%) | 0 (−15 to 16) |
| 14 | 2 (4%) | 7 (14%) | 10 (−2 to 23) |
| 15 | 3 (6%) | 1 (2%) | 4 (−5 to 15) |
| 16 | 3 (6%) | 1 (2%) | 4 (−5 to 15) |
| How often do you send/receive text messages? | |||
| Every day | 47 (100%) | 48 (100%) | 0 (−8 to 7) |
| On an average day, how many text messages would you say that you send or receive | |||
| 1–10 text messages | 4 (8%) | 1 (2%) | 6 (−4 to 18) |
| 11–20 text messages | 4 (8%) | 4 (8%) | 0 (−12 to 13) |
| 21–50 text messages | 6 (13%) | 8 (17%) | 4 (−11 to 18) |
| 51–100 text messages | 8 (17%) | 5 (10%) | 7 (−8 to 21) |
| More than 100 text messages | 22 (47%) | 26 (54%) | 7 (−12 to 26) |
| I don’t know | 3 (6%) | 4 (8%) | 2 (−10 to 13) |
DISCUSSION
In this randomized controlled trial, we found that frequent, personalized TM reminders following an ED visit for PID improved post-ED follow-up rates for adolescents. Because of the significant health risks associated with inadequately treated PID, the post-ED follow-up appointment is essential to ensure improvement and reinforce the importance of adherence to treatment recommendations.3 Adolescents receiving this diagnosis in the ED are unlikely to have received adequate counseling regarding safer sexual practices, which is important given that repeated episodes of PID increase the risk of chronic pelvic pain and infertility, further increasing the importance of this follow-up appointment.1,4,5 There were a myriad of reasons given for not attending a follow-up appointment including inadequate PCP availability, symptom improvement, and lack of understanding of importance of follow-up. The varied reasons for not following up are similar to other studies examining post-ED follow-up care.8–10 This is the first study to our knowledge using a text messaging modality in the adolescent population to improve post-ED follow-up.
Recent studies have shown the majority of teens have a cell phone and use TM as part of their daily lives.11,12,21 This was also demonstrated in our patient population with 99.5% of screened patients having cell phones with TM capability and with the majority of enrolled adolescents reporting texting over 100 times daily. The near universal acceptance of TM among adolescents as well as the private, convenient nature of this technology makes it the ideal modality to reach these patients. As a result, studies have examined the benefits of TM for various applications in medicine including notification of test results, harm reduction for high-risk sexual behaviors, simple smoking cessation interventions, and reminders for health behaviors such as medication reminders.2,10,15,17,21,22 A recent review demonstrated the benefits of TM reminders to increase attendance at previously scheduled healthcare appointments.23 Participants were more likely to attend previously scheduled appointments when they received a reminder by text message than those who received a reminder by phone or did not receive a reminder. A study by Arora et al. evaluated the effect of TM reminders in improving post-ED follow-up in adults.10 They demonstrated improvement in follow-up rates in spite of a relatively high baseline follow-up rate. In this study, appointments were made prior to the patient being discharged from the ED. Hence, the TM was serving as a simple reminder to the patient to attend the scheduled appointment. However, this is not generalizable as many EDs do not have this capability and those that do have this capability are unlikely to be able to achieve this for patients being discharged in the middle of the night or for patients who have PCPs in a different health care system. In our study, to better approximate real world circumstances, we did not schedule appointments for patients prior to discharge. The TM served as a reminder for patients to schedule an appointment which required the patient to call to schedule an appointment and then to attend the appointment, not simply as a reminder to attend the appointment.
There are several limitations in our study. Given that this study compared frequent TM reminders to standard discharge instructions which do not include any additional reminders, we cannot conclusively determine if the improved follow-up was due to the frequent reminders or the modality of TM. However, TM reminders were intentionally selected because frequent reminders with other modalities would be impractical and less acceptable due to limitations with automaticity, increased cost, and more obtrusive nature. Another limitation is the low baseline follow-up rate in this study. Although this is consistent with previous studies, it is quite low and as a result the effect may not be as pronounced in a community with a higher baseline follow-up rate. The patients at our institution also had access to follow-up in the adolescent clinic if they were unable to schedule an appointment with their PCP which may not be true in all settings. However, both treatment groups had access to this service. In addition, our study population may not reflect that of other institutions.
In summary, TM reminders are effective in increasing post-ED follow-up care in adolescents diagnosed with PID in the ED. This study utilized daily TM reminders, however, the appropriate frequency and timing of TM reminders after an ED visit remains a knowledge gap that should be addressed prior to broad-scale implementation of this technology.
CONCLUSIONS
TM reminders are effective in increasing post-ED follow-up care in adolescents diagnosed with PID in the ED and were well-received by patients.
Supplementary Material
Acknowledgments
Funding source: MW received an Academic Pediatric Association Young Investigator Award for this study. FB received career development support from NIH NHLBI K12-HL109009, though the funders were not involved in design and conduct of the study; collection, management, analysis, interpretation of the data; preparation, review, or approval of the manuscript.
Abbreviations
- CDC
Centers for Disease Control
- PID
pelvic inflammatory disease
- TM
text message
- ED
emergency department
- PCP
primary care provider
Footnotes
Contributors’ Statement: MW, EMS, and CM conceived the study, designed the trial, and obtained research funding. MW, FB, EMS, and CM supervised the conduct of the trial and data collection. MW performed the initial analysis and interpretation of the data; FB, EMS, and CM performed subsequent analysis and interpretation of the data. MW drafted the initial manuscript and FB, EMS, and CM revised the manuscript for important intellectual content and approved final manuscript as submitted.
Meetings: Oral presentation at The Pediatric Academic Societies Meeting, April 2015, San Diego, CA, USA.
Financial Disclosure: The authors have no financial relationships relevant to this article to disclose.
Conflict of Interest: The authors have no conflicts of interest relevant to this article to disclose.
Clinical Trial Registration: (clinicaltrials.gov, Identifier: NCT01299259, https://www.clinicaltrials.gov/ct2/show/NCT01299259?term=NCT01299259&rank=1)
References
- 1.Kelly AM, Ireland M, Aughey D. Pelvic inflammatory disease in adolescents: high incidence and recurrence rates in an urban teen clinic. J Pediatr Adolesc Gynecol. 2004;17:383–8. doi: 10.1016/j.jpag.2004.09.017. [DOI] [PubMed] [Google Scholar]
- 2.Suffoletto B, Akers A, McGinnis KA, Calabria J, Wiesenfeld HC, Clark DB. A sex risk reduction text-message program for young adult females discharged from the emergency department. J Adolesc Health. 2013;53:387–93. doi: 10.1016/j.jadohealth.2013.04.006. [DOI] [PubMed] [Google Scholar]
- 3.Workowski KA, Berman S. Sexually transmitted diseases treatment guidelines, 2010. MMWR Recomm Rep. 2010;59:1–110. [PubMed] [Google Scholar]
- 4.Goyal MK, Dowshen N, Mehta A, Hayes K, Lee S, Mistry RD. Pediatric primary care provider practices, knowledge, and attitudes of human immunodeficiency virus screening among adolescents. J Pediatr. 2013;163:1711–5. e6. doi: 10.1016/j.jpeds.2013.08.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Rhodes KV, Bisgaier J, Becker N, Padowitz N, Vashi A, McNutt LA. Emergency care of urban women with sexually transmitted infections: time to address deficiencies. Sex Transm Dis. 2009;36:51–7. doi: 10.1097/OLQ.0b013e318188389b. [DOI] [PubMed] [Google Scholar]
- 6.Trent M, Chung SE, Burke M, Walker A, Ellen JM. Results of a randomized controlled trial of a brief behavioral intervention for pelvic inflammatory disease in adolescents. J Pediatr Adolesc Gynecol. 2010;23:96–101. doi: 10.1016/j.jpag.2009.06.005. [DOI] [PubMed] [Google Scholar]
- 7.Trent M, Ellen JM, Walker A. Pelvic inflammatory disease in adolescents: care delivery in pediatric ambulatory settings. Pediatr Emerg Care. 2005;21:431–6. doi: 10.1097/01.pec.0000169432.14067.eb. [DOI] [PubMed] [Google Scholar]
- 8.Zorc JJ, Chew A, Allen JL, Shaw K. Beliefs and barriers to follow-up after an emergency department asthma visit: a randomized trial. Pediatrics. 2009;124:1135–42. doi: 10.1542/peds.2008-3352. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Zorc JJ, Scarfone RJ, Li Y, et al. Scheduled follow-up after a pediatric emergency department visit for asthma: a randomized trial. Pediatrics. 2003;111:495–502. doi: 10.1542/peds.111.3.495. [DOI] [PubMed] [Google Scholar]
- 10.Arora S, Burner E, Terp S, et al. Improving Attendance at Post-Emergency Department Follow-up Via Automated Text Message Appointment Reminders: A Randomized Controlled Trial. Acad Emerg Med. 2015;22:31–7. doi: 10.1111/acem.12503. [DOI] [PubMed] [Google Scholar]
- 11.Lenhart ALR, Campbell S, Purcell K. Teens and Mobile Phones. 2010 Apr 20;2010 [Google Scholar]
- 12.Madden MLA, Duggan M, Cortesi S, Gasser U. Teens and Technology. 2013 Mar 13;2013 [Google Scholar]
- 13.Armstrong AW, Watson AJ, Makredes M, Frangos JE, Kimball AB, Kvedar JC. Text-message reminders to improve sunscreen use: a randomized, controlled trial using electronic monitoring. Arch Dermatol. 2009;145:1230–6. doi: 10.1001/archdermatol.2009.269. [DOI] [PubMed] [Google Scholar]
- 14.Arora S, Peters AL, Burner E, Lam CN, Menchine M. Trial to examine text message-based mHealth in emergency department patients with diabetes (TExT-MED): a randomized controlled trial. Ann Emerg Med. 2014;63:745–54. e6. doi: 10.1016/j.annemergmed.2013.10.012. [DOI] [PubMed] [Google Scholar]
- 15.Estepp JH, Winter B, Johnson M, Smeltzer MP, Howard SC, Hankins JS. Improved hydroxyurea effect with the use of text messaging in children with sickle cell anemia. Pediatr Blood Cancer. 2014;61:2031–6. doi: 10.1002/pbc.25177. [DOI] [PubMed] [Google Scholar]
- 16.Miloh T, Annunziato R, Arnon R, et al. Improved adherence and outcomes for pediatric liver transplant recipients by using text messaging. Pediatrics. 2009;124:e844–50. doi: 10.1542/peds.2009-0415. [DOI] [PubMed] [Google Scholar]
- 17.Dowshen N, Kuhns LM, Gray C, Lee S, Garofalo R. Feasibility of interactive text message response (ITR) as a novel, real-time measure of adherence to antiretroviral therapy for HIV+ youth. AIDS Behav. 2013;17:2237–43. doi: 10.1007/s10461-013-0464-6. [DOI] [PubMed] [Google Scholar]
- 18.Thompson MA, Mugavero MJ, Amico KR, et al. Guidelines for improving entry into and retention in care and antiretroviral adherence for persons with HIV: evidence-based recommendations from an International Association of Physicians in AIDS Care panel. Ann Intern Med. 2012;156:817–33. doi: 10.7326/0003-4819-156-11-201206050-00419. W-284, W-5, W-6, W-7, W-8, W-9, W-90, W-91, W-92, W-93, W-94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.CDC. National Survey of Family Growth. CAPI Reference Female Questionnaire. 2006–2008 [Google Scholar]
- 20.Parent/Teen Cell Phone Survey. Princeton Survey Research Associates International for the Pew Internet & American Life Project. 2009 [Google Scholar]
- 21.Dowshen N, Kuhns LM, Johnson A, Holoyda BJ, Garofalo R. Improving adherence to antiretroviral therapy for youth living with HIV/AIDS: a pilot study using personalized, interactive, daily text message reminders. J Med Internet Res. 2012;14:e51. doi: 10.2196/jmir.2015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Obermayer JL, Riley WT, Asif O, Jean-Mary J. College smoking-cessation using cell phone text messaging. J Am Coll Health. 2004;53:71–8. doi: 10.3200/JACH.53.2.71-78. [DOI] [PubMed] [Google Scholar]
- 23.Gurol-Urganci I, de Jongh T, Vodopivec-Jamsek V, Atun R, Car J. Mobile phone messaging reminders for attendance at healthcare appointments. Cochrane Database Syst Rev. 2013;12:CD007458. doi: 10.1002/14651858.CD007458.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.