

Abstract
Background
Colorectal cancer (CRC) is the most common cancer affecting both men and women. Survivors of CRC often experience various physical and psychological effects arising from CRC and its treatment. These effects may last for many years and adversely affect QoL, and they may not be adequately addressed by standard specialist-based follow-up. Optimal management of these effects should harness the expertise of both primary care and specialist care. Shared models of care (involving both the patient’s primary care physician [PCP] and specialist) have the potential to better support survivors and enhance health system efficiency.
Methods/design
SCORE (Shared care of Colorectal cancer survivors) is a multisite randomised controlled trial designed to optimise and operationalise a shared care model for survivors of CRC, to evaluate the acceptability of the intervention and study processes, and to collect preliminary data regarding the effects of shared care compared with usual care on a range of patient-reported outcomes. The primary outcome is QoL measured using the European Organisation for Research and Treatment of Cancer QLQ-C30 questionnaire. Secondary outcomes are satisfaction with care, unmet needs, continuity of care and health resource use. The shared care model involves replacement of two routine specialist follow-up visits with PCP visits, as well as the provision of a tailored survivorship care plan and a survivorship booklet and DVD for CRC survivors. All consenting patients will be randomised 1:1 to either shared care or usual care and will complete questionnaires at three time points over a 12-month period (baseline and at 6 and 12 months). Health care resource use data will also be collected and used to evaluate costs.
Discussion
The evaluation and implementation of models of care that are responsive to the holistic needs of cancer survivors while reducing the burden on acute care settings is an international priority. Shared care between specialists and PCPs has the potential to enhance patient care and outcomes for CRC survivors while offering improvements in health care resource efficiency. If the findings of the present study show that the shared care intervention is acceptable and feasible for CRC survivors, the intervention may be readily expanded to other groups of cancer survivors.
Trial registration
Australian New Zealand Clinical Trials Registry, ACTRN12617000004369p. Registered on 3 January 2017; protocol version 4 approved 24 February 2017.
Electronic supplementary material
The online version of this article (doi:10.1186/s13063-017-2245-4) contains supplementary material, which is available to authorized users.
Keywords: Colorectal cancer, Survivorship, Follow-up, Shared care, Primary care, Models of care, Protocol
Background
Colorectal cancer: high burden of illness
Colorectal cancer (CRC; also known as bowel cancer) is the most common cancer affecting both men and women (excluding non-melanoma skin cancers) [1]. Although it is the second highest cause of death from cancer (after lung cancer), many people are long-term survivors. Survivors of CRC represent the third largest group of long-term cancer survivors in the Western world (after survivors of breast and prostate cancer) [2]. In the United States, an estimated 1.4 million people have a personal history of CRC [2]. It is expected that the number of people affected by and surviving CRC will rise significantly over the next 10 years. US data suggest an almost 24% increase in the number of CRC survivors between 2016 and 2026 [2].
Survivors report a broad range of consequences from CRC and its treatment, including persistent side effects, such as fatigue [3–8]; bowel, urinary and sexual dysfunction [3, 4, 7–18]; and neuropathy [6, 10, 19]. CRC survivors may experience elevated levels of psychological distress and depression [7, 16, 18, 20–23]. Fear of cancer recurrence is common [4, 7, 8, 24, 25]. Unsurprisingly, QoL among CRC survivors may be impaired compared with the general population [3, 5, 8, 9, 12, 14, 22, 26].
In our recent SurvivorCare study [27], a randomised controlled trial (RCT) investigating the impact of a supportive care intervention for CRC survivors, when compared with members of the general Australian population, CRC survivors around the time of treatment completion reported higher levels of fatigue, pain, nausea and vomiting, appetite loss, diarrhoea, constipation and financial problems [28]. They also reported lower levels of role, cognitive and social functioning. Commonly reported issues included frequent urination (67%), problems with taste (56%) and worries about future health (71%). In survivors with a stoma, 52% reported frequent bag changes, 66% reported flatulence and 61% reported some degree of leakage of stools. For survivors without a stoma, 68% reported flatulence, 36% had some degree of leakage of stools and 70% reported frequent daily bowel movements. Sixty-five percent of men reported some degree of impotence [28].
Similar findings were seen in a study of over 21,000 CRC survivors in England who were 12–36 months from diagnosis, again underscoring that CRC survivors have ongoing, unresolved symptom issues [12]. A further study of CRC survivors reported that addressing emotional problems during follow-up was important for patients but was commonly neglected [11].
Survivors frequently report unmet needs, including for more comprehensive, coordinated care; for more information; and for psychological support [15, 25, 28–31]. Again, in our SurvivorCare study, the most commonly endorsed need was ‘I need to know that all my doctors talk to each other to coordinate my care’ (68% endorsement) [28].
Inadequacies of current follow-up care after completing treatment
The Institute of Medicine (IOM), in its report ‘From Cancer Patient to Cancer Survivor: Lost in Transition’, asserts, ‘The transition from active treatment to post-treatment care is critical to long-term health. If care is not planned and coordinated, cancer survivors are left without knowledge of their heightened risks and a follow-up plan of action’ [32]. After completing treatment, most patients have ongoing follow-up with a cancer specialist [32, 33]. Despite the known complex and distressing concerns survivors of CRC face, follow-up guidelines are focussed largely on strategies to detect recurrence or possible second cancers [34, 35]. The IOM report adds, ‘Notably absent is guidance regarding the functional sequelae that may follow surgical interventions (e.g., colostomy, bowel dysfunction, sexual dysfunction)’ [32]. Current models of care are inadequate, with limited attention given to supportive care issues, preventive care and management of comorbid illness [32, 34, 36]. Additionally, current models of specialist-based care are expensive and likely unsustainable [32, 37]. There is a mismatch between the availability of cancer services and the growing number of survivors [37]. Nevertheless, very little research has been focussed on the post-treatment care of CRC survivors [38].
Alternative models of patient follow-up
Grunfeld led the first RCTs comparing follow-up with primary care physicians (PCPs) versus specialist-based care, for breast cancer survivors [39–44]. These studies showed that disease outcomes [41, 43] and patient QoL [39] were similar, though PCP-based care was associated with improved patient satisfaction [39] and lower costs, for both patients and health services [40]. In a single, Australia-based RCT, researchers evaluated PCP follow-up versus specialist follow-up for people with CRC [45]. No compelling evidence for a difference was found.
These studies had a relatively narrow focus, primarily on the detection of cancer recurrence. Recommended survivorship care should also determine survivors’ concerns, attend to treatment side effects and comorbid illness, and ensure support, as necessary.
Shared care between primary care physicians and specialists
Despite the results of the above-described RCTs, PCP-based follow-up has not been widely adopted. Our own work involving survivors, PCPs, surgeons and oncologists indicated strong endorsement that PCPs be involved in the ongoing care of CRC survivors and provided with information to facilitate care [46].
The vast majority of cancer survivors have coexisting illness [47, 48]. Survivors who have follow-up involving primary care are more likely to receive preventive interventions and have appropriate management of comorbid illness [36].
Models of post-treatment care should address the holistic health care needs of cancer survivors with optimal cancer-specific follow-up, management of comorbid conditions, and general preventive health care [49, 50]. These models of care should optimise the expertise of different providers for the benefit of patients and efficiency of the health care system.
An alternative to the current model of oncology-based survivorship care is a shared care model, harnessing the expertise of both PCPs and specialists [51–53]. Shared care is widely used in antenatal care and in the management of patients with conditions such as asthma, diabetes and ischaemic heart disease. Few studies have evaluated shared care with cancer survivors. In our randomised phase II study involving men with prostate cancer, ProCare [54], we found distress levels, QoL and satisfaction were similar in both groups; shared care was preferred by men who had experienced it, and the shared care model was less costly [55].
Principles underpinning a novel shared care model of follow-up
The Shared care of Colorectal cancer survivors (SCORE) intervention is underpinned by considerations in the Chronic Care Model (CCM) [56] and recommendations from the IOM regarding post-treatment care [32].
Studies suggest that redesigning care using the CCM leads to improved patient care and better health outcomes [57, 58]. As recommended by the CCM, SCORE is focussed on patients, professionals and the organisation of care. Key elements include structured clinical follow-up, reminders and education for professionals, and patient education and self-management support. These strategies aim to improve continuity and coordination of care and enhance patient outcomes [59].
In its report ‘From Cancer Patient to Cancer Survivor: Lost in Transition’, the IOM outlined four essential components of post-treatment survivorship care: (1) prevention of recurrent and new cancers, and of other late effects; (2) surveillance for cancer spread, recurrence or second cancers, as well as assessment of medical and psychosocial late effects; (3) intervention for consequences of cancer and its treatment; and (4) coordination between specialists and primary care providers to ensure that all of the survivor’s health needs are met [32]. A recent review of guidelines regarding follow-up of CRC survivors highlighted that most are focussed on the detection of cancer recurrence and assessment of the medical consequences of treatment, with little attention placed on identifying and responding to other key unmet needs [34]. The aim of SCORE is to provide more comprehensive, holistic care. The principles that inform the SCORE model are described in the subsections that follow.
Communication between specialists and PCPs
A current major barrier is coordination of care between specialists and PCPs. Timely and systematic communication between specialists and PCPs is urgently required to clarify the roles and responsibilities of all, including the person with cancer [60]. We previously showed that faxing standardised information to PCPs about a patient’s chemotherapy regimen improved confidence of PCPs in managing adverse effects of treatment and increased satisfaction with shared care [61]. PCPs will be provided with timely patient-specific information and clinical guidance.
Promotion of patient involvement and engagement
The majority of Australian patients with cancer want to be involved with decision-making and wish to participate in strategies to remain well [62]. Involving patients with chronic diseases in their disease management results in better communication with physicians, improved self-reported health and reduced health distress, fewer hospitalisations, and reduced health costs [63, 64]. A systematic review of patient activation approaches has shown these strategies can alter the content of consultations and improve the identification of patients’ concerns [65]. Approaches that allow patients to list and share their concerns with their doctors, particularly if linked to practitioner interventions, showed particular promise. Patients will have a mechanism to identify and discuss concerns with their PCP.
Tailoring to specific needs of individual patients
Cancer survivors have individualised needs [28, 66]. Therefore, interventions need to be systematically tailored to each individual. Authors of a review of tailored versus standardised information interventions in the health promotion area found that tailored interventions were significantly more effective in promoting health behaviour outcomes [67]. SCORE will enable both patients (survivors) and PCPs to identify issues of concern to the individual person.
Objectives and trial design
Objectives
The objectives of the trial are to operationalise and optimise the shared care intervention; establish acceptability of the intervention, randomisation, outcome measures and study processes; obtain preliminary estimates of effects on patient-reported outcome measures and health care resource use; and to confirm the appropriateness of expansion to a definitive phase III trial.
Hypotheses
We hypothesise that, relative to usual care, shared care will be an acceptable model of follow-up with the potential to address care needs more efficiently than standard care.
Trial design
This is a randomised, parallel group trial in which patients with CRC undergoing primary treatment with curative intent will be allocated to receive either standard specialist-based follow-up care or shared follow-up care between their specialist and PCP. Clinical reviews will occur at 3, 6, 9 and 12 months. Patient self-reported measures will be done at baseline and at 6 and 12 months. The trial will be conducted in accordance with good clinical practice guidelines and the Declaration of Helsinki. The protocol is in line with the Standard Protocol Items: Recommendations for Interventional Trials guidelines [68] and the Consolidated Standards for Reporting of Trials guidelines [69] (Fig. 1, study flow diagram) (Additional file 1). The trial is registered with the Australian New Zealand Clinical Trials Registry (number 12617000004369p).
Fig. 1.
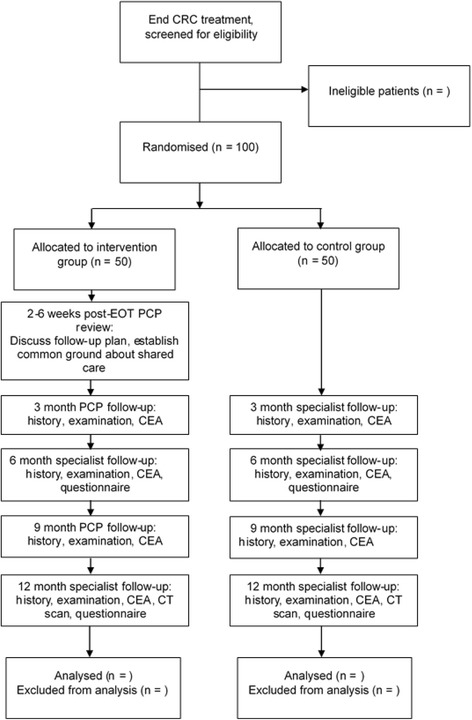
Flow diagram of patient recruitment and study conduct. CEA Carcinoembryonic antigen, CRC Colorectal cancer, CT Computed tomography, EOT End of treatment, PCP Primary care physician
Methods/design
Participants, interventions and outcomes
Study setting
The study will be conducted at the Peter MacCallum Cancer Centre, Royal Melbourne Hospital, Western Health, St Vincent’s Hospital and Austin Health, Melbourne, Victoria, Australia. Each site treats a considerable number of people with CRC.
Eligibility criteria
Inclusion: To be eligible, patients must (1) have a histologically confirmed diagnosis of colon or rectal cancer, (2) have stage I–III disease, (3) have completed treatment with curative intent with surgery with or without radiation with or without chemotherapy within 2 months, (4) be over 18 years of age, (5) be able to understand English, and (6) have a PCP who is willing to participate in the study.
Exclusion: Exclusion criteria are patients (1) with demonstrated cognitive or psychological difficulties that would preclude study participation as defined by the treatment team, (2) who are too unwell to participate in the study as determined by the patient’s treatment team, (3) who have received treatment for a prior cancer (excluding non-melanoma skin cancer), and (4) who have a PCP who is already participating in the study (to avoid contamination between randomisation groups).
Withdrawal: Participants will be withdrawn if (1) they have cancer recurrence or (2) they withdraw consent. Discontinuation because of adverse events will be at either the request of the participant or the discretion of the investigator(s).
Interventions
Participants will receive either standard specialist-based follow-up care (usual follow-up care) or shared follow-up care between specialist and PCP (shared care intervention) for a period of 12 months.
Control group
Patients in the control group will receive usual care in accordance with hospital practice. Usual follow-up care occurs at 3-monthly intervals during the first year following the end of treatment and includes patient history, physical examination, blood test for carcinoembryonic antigen, and computed tomographic scan at 12 months if recommended by the patient’s treating specialist [34, 35, 70].
Intervention group
Patients in the intervention group will receive shared care between specialist and PCP. The shared care intervention will replace two specialist appointments at 3 and 9 months with PCP appointments and add an additional PCP appointment 2 to 6 weeks following the end of treatment to re-establish contact and discuss follow-up care. At baseline, participants allocated to shared care will receive additional resources, including a tailored survivorship care plan, a ‘Living Well after Cancer’ booklet [71] and a DVD titled ‘Just Take It Day to Day’ [72]. A common issues and concerns checklist will also be administered prior to PCP clinic attendance to assist with identification of individual needs. The survivorship care plan will be prepared by the research team and approved by the treating specialist, and it will include diagnosis, treatment history, details about additional hospital services received and information about common issues experienced by CRC survivors, and information about staying well and available community services. The PCP will receive a copy of the survivorship care plan and management guidelines detailing common issues experienced by CRC survivors and how to manage these, as well as how best to contact the specialist treating team for advice or if recurrence is suspected. Both patients and PCPs will receive a reminder letter about upcoming follow-up appointments, with PCPs further reminded to provide information on patient progress and have pathology results copied to specialist.
Outcomes
The primary outcome will be overall QoL at 12 months using the European Organisation for Research and Treatment of Cancer core questionnaire (EORTC QLQ-C30) [73]. Secondary outcomes include individual aspects of QoL, unmet needs, continuity of care and satisfaction.
Individual aspects of QoL: The EORTC QLQ-C30 functional and symptom scales and the CRC module (EORTC QLQ-CR29) [74] collectively assess specific symptoms such as fatigue, anxiety and pain as well as function on several domains, including physical, role, emotional, cognitive, social, sexual, urinary and bowel.
Survivors’ unmet needs: The Short-Form Survivor Unmet Needs Survey [75] is the brief version of the Survivor Unmet Needs Survey 89-item scale. It provides a measure of cancer survivors’ unmet needs, using 30 items across 5 domains: emotional health (8 items), access and continuity of care (6 items), relationships (5 items), financial concerns (8 items) and information (3 items). Each item is scored from 0 (no unmet need) to 4 (very high unmet need) [75].
Continuity of care: The Picker Ambulatory Oncology survey comprises eight items that assess patient experience of oncology care [76]. Three items are scored ‘yes completely’, ‘yes somewhat’ or ‘no’ and five items are scored ‘never’, ‘sometimes’, ‘usually’ or ‘always’. Each of the items is fractioned to the number of positive and negative responses. A total score is derived from these positive and negative responses [76].
Satisfaction: The Patient Satisfaction Questionnaire short form, derived from the 50-item Patient Satisfaction Questionnaire, comprises 18 items assessing satisfaction [77]. Seven subscales are used: general satisfaction (items 3 and 17), technical quality (items 2, 4, 6 and 14), interpersonal manner (items 10 and 11), communication (items 1 and 13), financial aspects (items 5 and 7), time spent with doctor (items 12 and 15), and accessibility and convenience (items 8, 9, 16 and 18). Each item is scored on a 5-point Likert scale ranging from ‘strongly agree’ to ‘strongly disagree’. Agreement on some scales indicates satisfaction, whereas agreement on other scales reflects dissatisfaction. All items are scored such that high scores reflect satisfaction with medical care.
Demographics and clinical variables: A range of demographic and clinical information will be collected for each patient, including age, sex, language spoken at home, living arrangements, postcode, occupation, work status, level of income, diagnosis and stage of disease, and treatment type.
Health care resource use: Patients will be consented for access to data on medical service use via Medicare (Australia’s publicly funded universal health care system) from the Commonwealth Department of Human Services. This will provide information on the type, frequency and costs associated with medical service use by participants. Information on hospital service use will be sourced from hospital records on the basis of occurrence of events and costed using Australian Refined Diagnosis Related Groups.
Recurrence: To determine recurrence, participants are asked to provide an indication that disease recurrence is suspected; these questions were developed by Cancer Experiences Research, Peter MacCallum Cancer Centre.
Fidelity: There are two components to the fidelity section. First, participants are asked to respond whether additional specialist/PCP appointments were scheduled during the follow-up period. Second, there are eight questions that pertain to what participants remember receiving (e.g., survivorship care plan, DVD) as part of the intervention. Questions pertaining to these variables have been sourced from our previous follow-up care survey [27].
Participant time line: The assessment and appointment schedule is detailed in Fig. 2.
Fig. 2.
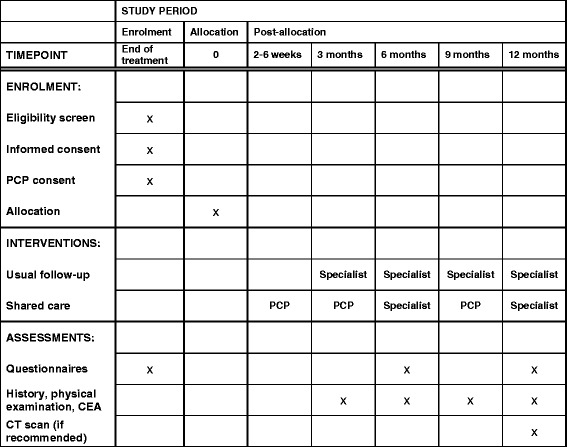
Schedule of appointments and assessment. CEA Carcinoembryonic antigen, CT Computed tomography, PCP Primary care physician
Sample size
A sample size of 100 patients (50 in each arm) will allow estimation of key parameters with adequate precision to determine the appropriateness of expansion to a definitive phase III trial. The 95% CI for a retention rate of 90% for a study of this size would range from 82% to 95%. A retention rate below 80% would constitute grounds for modifying aspects of the study prior to expansion to a definitive phase III trial. Furthermore, the 95% CIs for the mean difference between the two groups on patient-reported outcome measures would extend no further than ±0.5 SD (given a retention rate of 90%). This level of precision corresponds to what has been proposed as a minimal clinically important difference for health-related QoL measures [78]. Evidence of a substantial detriment associated with shared care as measured by a reduction of 0.6 (or worse) on a patient-reported outcome measure would be detected with 80% power (at the 2.5% one-sided level of significance). A statistically significant negative finding on the global QoL scale from the EORTC QLQ-C30 would constitute grounds for abandoning expansion to a definitive phase III trial.
Recruitment
A research team will be appointed at each site. The research team will identify and screen potentially eligible patients from outpatient clinic lists as well as chemotherapy, surgery and radiotherapy lists, with the assistance of clinicians. Eligibility will be confirmed with the treating clinician prior to approach to clarify details from medical records and to ensure the clinician is aware of the patient’s involvement with the study.
Once it has been established that a patient is potentially eligible for the trial, the research team will approach the patient and invite him or her to participate (Additional files 2 and 3). Eligible and consenting patients will complete baseline measures prior to randomisation. The patient’s preferred PCP will be contacted to confirm willingness to be involved in the trial, should the patient be randomised to the intervention arm. An opt-out approach will be used. If the PCP returns the form noting that they prefer not to participate in the study, no further contact will be made. If the PCP contacts the research team stating they would like to take part, or if the form is not returned within 1 week, consent to take part in the study will be implied.
Patients who decline to participate will be asked for their verbal consent to collect basic demographic and clinical information from their records to examine potential recruitment bias. Reasons for refusal will be recorded.
Assignment of interventions
Trial participants will be randomised to receive either shared care or usual care using a 1:1 ratio following completion of baseline measures. The randomisation sequence will be based on a minimisation scheme with stratification for site (Peter MacCallum Cancer Centre, Royal Melbourne Hospital, Western Health, St Vincent’s Hospital and Austin Hospital). The randomisation sequence will be computer-generated by the research team at Peter MacCallum Cancer Centre using a centralised randomisation database. The allocation sequence will be concealed within a management system (Microsoft Access database; Microsoft, Redmond, WA, USA) managed by a data manager who is independent of the day-to-day conduct of the trial.
Data collection, management and analysis
Data collection methods
The outcome measures will be taken at the end of treatment (baseline) and at 6 and 12 months. Recurrence will be collected at 6 and 12 months with fidelity measures being collected at 12 months. Arrangements of appointments will be self-managed by the participant throughout the trial period. Adherence to follow-up appointments will be collected through Medicare data at the end of the patient’s participation in the trial.
Statistical methods
Acceptability of the intervention, randomisation, outcome measures and study processes will be based on a comparison between the expected and observed (1) recruitment rate and (2) proportion of participants completing the study requirements. The planned recruitment rate will be evaluated against the actual recruitment rate in a descriptive fashion (e.g., as a line graph). A point estimate and 95% CI for the proportion completing the study requirements will be calculated and evaluated against a benchmark of 80%. Statistical evidence that the completion probability was inconsistent with the 80% target or that actual recruitment fell appreciably below expectations would constitute grounds for modifying aspects of the study prior to expansion to a definitive phase III trial. The effect of shared care compared with usual care on scales from the patient-reported outcome measures will be quantified by applying a mixed model for repeated measures approach to the data collected. Point estimates of effect on these scales will be presented with 95% CIs. Statistical evidence of a negative impact on the global QoL scale would constitute grounds for abandoning expansion to a definitive phase III trial. This would occur if the two-sided 95% CI for the treatment effect favoured standard care and excluded 0. (Such a result is equivalent to obtaining a significant p value at the one-sided 2.5% level of significance.)
Costs and outcomes between usual care and shared care will be compared on the basis of resources required for the delivery of care and the use of medical services by patients. The comparison of outcomes will be focussed on the difference in the proportion of patients with unmet needs allowing an indicative assessment of the cost per additional patient whose needs are met by shared care compared with usual care. Results for the EORTC QLQ-C30 will be converted to preference-based measures of QoL (the EORTC Quality of Life Utility Measure–Core 10 dimensions) [79] for use in estimating quality-adjusted life-years (QALYs). With these data, a potential difference in costs per QALY between usual care and shared care will be explored in a model-based analysis. Differences in cost data will be subject to non-parametric testing, with appropriate sensitivity analyses conducted of comparisons of costs and outcomes [80].
Monitoring
Data monitoring
The study has received ethics approval from the human research ethics committee of Peter MacCallum Cancer Centre (HREC/16/PMCC/89). No significant risks to participants are anticipated. Because the study is unblinded without drug intervention, an independent data and safety monitoring committee is unnecessary; however, the trial management committee will review the recruitment rate, the retention rate, and the data completion rate on an ongoing basis. The trial management committee includes CRC medical and surgical oncologists, PCPs, a behavioural scientist, a statistician, a health economist and a consumer.
Safety
Any adverse or unexpected outcomes which occur as a result of the trial will be documented and copies provided to site investigators and the principal investigator within 24 h. The principal investigator will proceed to report any such adverse event to the human research ethics committee.
Discussion
There is growing interest in post-treatment care in the clinical and research setting, with recognition that current service provision is both inadequate in meeting the needs of survivors and unsustainable, given the growing number of survivors and limited health workforce [32, 37]. It is internationally recognised that models of care are needed which are responsive to the needs of survivors and caregivers and representing more efficient use of limited health care resources [32, 51, 52, 81].
Numerous studies show that survivors of CRC have persisting symptoms, impaired QoL and unmet needs [3, 4, 9–12, 14–16, 18, 20, 21, 26, 28]. They also miss out on health promotion and disease prevention opportunities and appropriate management of comorbid illness [33, 36]. To our knowledge, this is the first study of shared care for people with CRC internationally. Very few studies have addressed survivorship care for CRC survivors. The present clinical trial considers a more comprehensive view of life after cancer, with a focus not just on disease and cancer recurrence but also on dealing with the consequences of cancer and promoting optimal health and well-being [34]. The aim of the intervention is to comprehensively assess needs and link people to necessary multidisciplinary care. The intervention will provide clarity for patients regarding their follow-up and give patients and PCPs the information that they need. Formalising shared care improves communication for survivors, carers and health professionals and limits the underuse and overuse of tests and services [59, 82].
Researchers in a similar study seek to assess QoL in patients with CRC and evaluate an intervention targeted at QoL deficits [83]. This study is based on a similar successful approach for breast cancer survivors [84].
A possible limitation in the SCORE design is differential participation by both CRC survivors and PCPs. We will monitor characteristics of participants and non-participants. Shared care approaches may not be preferred (or appropriate) for all people. In our previous ProCare study, of 84 patients who met eligibility criteria but were not enrolled, only 9 were due to a PCP’s decision to not participate [55].
SCORE considers important outcomes that will remain relevant in the future, including costs, health and well-being, cancer outcomes, management of consequences, illness prevention and chronic disease management. If successful, the findings derived from this study would be transferable to other groups of cancer survivors. The study may also lead to exploration of modifications of shared care protocols: less frequent reviews, remote monitoring or care led by nursing or allied health professionals. It is also likely that demonstration of the impact of shared care in one cancer survivorship setting will lead to exploration and adoption of the model with other groups of cancer survivors.
Trial status
Currently 16 patients have been recruited.
Additional files
Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) 2013 checklist: recommended items to address in a clinical trial protocol and related documents. (DOC 120 kb)
Participant information sheet/consent form. (DOCX 55 kb)
Medicare consent form. (DOCX 33 kb)
Acknowledgements
Not applicable.
Funding
This trial is funded by the Victorian Cancer Agency in partnership with the Victorian Integrated Cancer Services through a Health Services Research Program grant. The funding body had no role in the design of the study or in the writing of the manuscript of this article, nor will it have any role in the collection, analysis and interpretation of data or in the writing of subsequent manuscripts.
Availability of data and materials
Not applicable.
Abbreviations
- CEA
Carcinoembryonic antigen
- CCM
Chronic Care Model
- CRC
Colorectal cancer
- CT
Computed tomography
- EORTC QLQ-C30
European Organisation for Research and Treatment of Cancer core questionnaire
- EOT
End of treatment
- IOM
Institute of Medicine
- PCP
Primary care physician
- QALY
Quality-adjusted life-year
- RCT
Randomised controlled trial
- SCORE
Shared care of Colorectal cancer survivors intervention
Authors’ contributions
MJ, PS, JE, EG, AM, RDAL, AH, DK and JPN conceived of and designed the study and acquired the funding. MJ, PR, AMM and LG developed the study protocol and procedures and obtained ethics approval. MJ, PR, AMM, NT, AB, IF, AH and RW are responsible for acquisition of data. AM and RDAL are responsible for the analysis and interpretation of data. MJ drafted the manuscript. All authors were involved in revising the manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to participate
Ethics approval was received 15 December 2016 from the Peter MacCallum Cancer Centre Human Research Ethics Committee (HREC/16/PMCC/89). Amendments to the study will be submitted to ethic committees and updated on the trial registry. Participants have provided or will provide written informed consent to participate in the trial.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Footnotes
Electronic supplementary material
The online version of this article (doi:10.1186/s13063-017-2245-4) contains supplementary material, which is available to authorized users.
Contributor Information
Michael Jefford, Phone: +61 3 8559 7902, Email: Michael.Jefford@petermac.org.
Jon Emery, Email: jon.emery@unimelb.edu.au.
Eva Grunfeld, Email: eva.grunfeld@utoronto.ca.
Andrew Martin, Email: andrew.martin@ctc.usyd.edu.au.
Paula Rodger, Email: paula.rodger@petermac.org.
Alexandra M. Murray, Email: alexandra.murray@petermac.org
Richard De Abreu Lourenco, Email: richard.deabreulourenco@chere.uts.edu.au.
Alexander Heriot, Email: alexander.heriot@petermac.org.
Jo Phipps-Nelson, Email: jo.phipps-nelson@petermac.org.
Lisa Guccione, Email: lisa.guccione@rmit.edu.au.
Dorothy King, Email: dorothy.king13@yahoo.com.
Karolina Lisy, Email: karolina.lisy@petermac.org.
Niall Tebbutt, Email: niall.tebbutt@onjcri.org.au.
Adele Burgess, Email: admin@heidelbergsurgical.com.au.
Ian Faragher, Email: ian.faragher@wh.org.au.
Rodney Woods, Email: rodney.woods@svhs.org.au.
Penelope Schofield, Email: pschofield@swin.edu.au.
References
- 1.Torre LA, et al. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65(2):87–108. doi: 10.3322/caac.21262. [DOI] [PubMed] [Google Scholar]
- 2.Miller KD, et al. Cancer treatment and survivorship statistics, 2016. CA Cancer J Clin. 2016;66(4):271–89. doi: 10.3322/caac.21349. [DOI] [PubMed] [Google Scholar]
- 3.Arndt V, et al. Quality of life in patients with colorectal cancer 1 year after diagnosis compared with the general population: a population-based study. J Clin Oncol. 2004;22(23):4829–36. doi: 10.1200/JCO.2004.02.018. [DOI] [PubMed] [Google Scholar]
- 4.Baker F, et al. Adult cancer survivors: how are they faring? Cancer. 2005;104(11 Suppl):2565–76. doi: 10.1002/cncr.21488. [DOI] [PubMed] [Google Scholar]
- 5.Kopp I, Bauhofer A, Koller M. Understanding quality of life in patients with colorectal cancer: comparison of data from a randomised controlled trial, a population based cohort study and the norm reference population. Inflamm Res. 2004;53(Suppl 2):S130–5. doi: 10.1007/s00011-004-0361-6. [DOI] [PubMed] [Google Scholar]
- 6.Pettersson G, et al. Symptom prevalence, frequency, severity, and distress during chemotherapy for patients with colorectal cancer. Support Care Cancer. 2014;22(5):1171–9. doi: 10.1007/s00520-013-2069-z. [DOI] [PubMed] [Google Scholar]
- 7.Phipps E, et al. Quality of life and symptom attribution in long-term colon cancer survivors. J Eval Clin Pract. 2008;14(2):254–8. doi: 10.1111/j.1365-2753.2007.00842.x. [DOI] [PubMed] [Google Scholar]
- 8.Schag CA, et al. Quality of life in adult survivors of lung, colon and prostate cancer. Qual Life Res. 1994;3(2):127–41. doi: 10.1007/BF00435256. [DOI] [PubMed] [Google Scholar]
- 9.Caravati-Jouvenceaux A, et al. Health-related quality of life among long-term survivors of colorectal cancer: a population-based study. Oncologist. 2011;16(11):1626–36. doi: 10.1634/theoncologist.2011-0036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Denlinger CS, Barsevick AM. The challenges of colorectal cancer survivorship. J Natl Compr Canc Netw. 2009;7(8):883–93. doi: 10.6004/jnccn.2009.0058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Di Fabio F, et al. Long-term outcome after colorectal cancer resection: patients’ self-reported quality of life, sexual dysfunction and surgeons’ awareness of patients’ needs. Tumori. 2008;94(1):30–5. doi: 10.1177/030089160809400107. [DOI] [PubMed] [Google Scholar]
- 12.Downing A, et al. Health-related quality of life after colorectal cancer in England: a patient-reported outcomes study of individuals 12 to 36 months after diagnosis. J Clin Oncol. 2015;33(6):616–24. doi: 10.1200/JCO.2014.56.6539. [DOI] [PubMed] [Google Scholar]
- 13.Emmertsen KJ, Laurberg S, Rectal Cancer Function Study Group Impact of bowel dysfunction on quality of life after sphincter-preserving resection for rectal cancer. Br J Surg. 2013;100(10):1377–87. doi: 10.1002/bjs.9223. [DOI] [PubMed] [Google Scholar]
- 14.Jansen L, et al. Quality of life among long-term (≥5 years) colorectal cancer survivors – systematic review. Eur J Cancer. 2010;46(16):2879–88. doi: 10.1016/j.ejca.2010.06.010. [DOI] [PubMed] [Google Scholar]
- 15.Nikoletti S, et al. Bowel problems, self-care practices, and information needs of colorectal cancer survivors at 6 to 24 months after sphincter-saving surgery. Cancer Nurs. 2008;31(5):389–98. doi: 10.1097/01.NCC.0000305759.04357.1b. [DOI] [PubMed] [Google Scholar]
- 16.Ramsey SD, et al. Quality of life in long term survivors of colorectal cancer. Am J Gastroenterol. 2002;97(5):1228–34. doi: 10.1111/j.1572-0241.2002.05694.x. [DOI] [PubMed] [Google Scholar]
- 17.Schover LR, et al. Sexual dysfunction and infertility as late effects of cancer treatment. EJC Suppl. 2014;12(1):41–53. doi: 10.1016/j.ejcsup.2014.03.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Trentham-Dietz A, et al. Health-related quality of life in female long-term colorectal cancer survivors. Oncologist. 2003;8(4):342–9. doi: 10.1634/theoncologist.8-4-342. [DOI] [PubMed] [Google Scholar]
- 19.Gamelin E, et al. Clinical aspects and molecular basis of oxaliplatin neurotoxicity: current management and development of preventive measures. Semin Oncol. 2002;29(5 Suppl 15):21–33. doi: 10.1053/sonc.2002.35525. [DOI] [PubMed] [Google Scholar]
- 20.Chambers SK, et al. A five-year prospective study of quality of life after colorectal cancer. Qual Life Res. 2012;21(9):1551–64. doi: 10.1007/s11136-011-0067-5. [DOI] [PubMed] [Google Scholar]
- 21.Graca Pereira M, Figueiredo AP, Fincham FD. Anxiety, depression, traumatic stress and quality of life in colorectal cancer after different treatments: a study with Portuguese patients and their partners. Eur J Oncol Nurs. 2012;16(3):227–32. doi: 10.1016/j.ejon.2011.06.006. [DOI] [PubMed] [Google Scholar]
- 22.Krouse RS, et al. Health-related quality of life among long-term rectal cancer survivors with an ostomy: manifestations by sex. J Clin Oncol. 2009;27(28):4664–70. doi: 10.1200/JCO.2008.20.9502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Lynch BM, et al. Describing and predicting psychological distress after colorectal cancer. Cancer. 2008;112(6):1363–70. doi: 10.1002/cncr.23300. [DOI] [PubMed] [Google Scholar]
- 24.Deimling GT, et al. Cancer-related health worries and psychological distress among older adult, long-term cancer survivors. Psychooncology. 2006;15(4):306–20. doi: 10.1002/pon.955. [DOI] [PubMed] [Google Scholar]
- 25.Simard S, et al. Fear of cancer recurrence in adult cancer survivors: a systematic review of quantitative studies. J Cancer Surviv. 2013;7(3):300–22. doi: 10.1007/s11764-013-0272-z. [DOI] [PubMed] [Google Scholar]
- 26.Ramsey SD, et al. Quality of life in survivors of colorectal carcinoma. Cancer. 2000;88(6):1294–303. doi: 10.1002/(SICI)1097-0142(20000315)88:6<1294::AID-CNCR4>3.0.CO;2-M. [DOI] [PubMed] [Google Scholar]
- 27.Jefford M, et al. Evaluating a nurse-led survivorship care package (SurvivorCare) for bowel cancer survivors: study protocol for a randomized controlled trial. Trials. 2013;14:260. doi: 10.1186/1745-6215-14-260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Russell L, et al. Psychological distress, quality of life, symptoms and unmet needs of colorectal cancer survivors near the end of treatment. J Cancer Surviv. 2015;9(3):462–70. doi: 10.1007/s11764-014-0422-y. [DOI] [PubMed] [Google Scholar]
- 29.Armes J, et al. Patients’ supportive care needs beyond the end of cancer treatment: a prospective, longitudinal survey. J Clin Oncol. 2009;27(36):6172–9. doi: 10.1200/JCO.2009.22.5151. [DOI] [PubMed] [Google Scholar]
- 30.Harrison SE, et al. Primary health and supportive care needs of long-term cancer survivors: a questionnaire survey. J Clin Oncol. 2011;29(15):2091–8. doi: 10.1200/JCO.2010.32.5167. [DOI] [PubMed] [Google Scholar]
- 31.Salz T, et al. Colorectal cancer survivors’ needs and preferences for survivorship information. J Oncol Pract. 2014;10(4):e277–82. doi: 10.1200/JOP.2013.001312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Stovall E, Greenfield S, Hewitt M, editors. From cancer patient to cancer survivor: lost in transition. Washington, DC: National Academies Press; 2006;1–128.
- 33.Weaver KE, et al. Follow-up care experiences and perceived quality of care among long-term survivors of breast, prostate, colorectal, and gynecologic cancers. J Oncol Pract. 2014;10(4):e231–9. doi: 10.1200/JOP.2013.001175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Jorgensen ML, Young JM, Solomon MJ. Optimal delivery of colorectal cancer follow-up care: improving patient outcomes. Patient Relat Outcome Meas. 2015;6:127–38. doi: 10.2147/PROM.S49589. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Steele SR, et al. Practice guideline for the surveillance of patients after curative treatment of colon and rectal cancer. Dis Colon Rectum. 2015;58(8):713–25. doi: 10.1097/DCR.0000000000000410. [DOI] [PubMed] [Google Scholar]
- 36.Earle CC, Neville BA. Under use of necessary care among cancer survivors. Cancer. 2004;101(8):1712–9. doi: 10.1002/cncr.20560. [DOI] [PubMed] [Google Scholar]
- 37.Yang W, et al. Projected supply of and demand for oncologists and radiation oncologists through 2025: an aging, better-insured population will result in shortage. J Oncol Pract. 2014;10(1):39–45. doi: 10.1200/JOP.2013.001319. [DOI] [PubMed] [Google Scholar]
- 38.Aziz NM, Rowland JH. Cancer survivorship research among ethnic minority and medically underserved groups. Oncol Nurs Forum. 2002;29(5):789–801. doi: 10.1188/02.ONF.789-801. [DOI] [PubMed] [Google Scholar]
- 39.Grunfeld E, et al. Comparison of breast cancer patient satisfaction with follow-up in primary care versus specialist care: results from a randomized controlled trial. Br J Gen Pract. 1999;49(446):705–10. [PMC free article] [PubMed] [Google Scholar]
- 40.Grunfeld E, et al. Follow-up of breast cancer in primary care vs specialist care: results of an economic evaluation. Br J Cancer. 1999;79(7-8):1227–33. doi: 10.1038/sj.bjc.6690197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Grunfeld E, et al. Randomized trial of long-term follow-up for early-stage breast cancer: a comparison of family physician versus specialist care. J Clin Oncol. 2006;24(6):848–55. doi: 10.1200/JCO.2005.03.2235. [DOI] [PubMed] [Google Scholar]
- 42.Grunfeld E, et al. Evaluating primary care follow-up of breast cancer: methods and preliminary results of three studies. Ann Oncol. 1995;6(Suppl 2):47–52. doi: 10.1093/annonc/6.suppl_2.S47. [DOI] [PubMed] [Google Scholar]
- 43.Grunfeld E, et al. Routine follow up of breast cancer in primary care: randomised trial. BMJ. 1996;313(7058):665–9. doi: 10.1136/bmj.313.7058.665. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Grunfeld E, et al. Follow up in breast cancer: quality of life unaffected by general practice follow up. BMJ. 1995;311(6996):54. doi: 10.1136/bmj.311.6996.54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Wattchow DA, et al. General practice vs surgical-based follow-up for patients with colon cancer: randomised controlled trial. Br J Cancer. 2006;94(8):1116–21. doi: 10.1038/sj.bjc.6603052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Baravelli C, et al. The views of bowel cancer survivors and health care professionals regarding survivorship care plans and post treatment follow up. J Cancer Surviv. 2009;3(2):99–108. doi: 10.1007/s11764-009-0086-1. [DOI] [PubMed] [Google Scholar]
- 47.Hewitt M, Rowland JH, Yancik R. Cancer survivors in the United States: age, health, and disability. J Gerontol A Biol Sci Med Sci. 2003;58(1):82–91. doi: 10.1093/gerona/58.1.M82. [DOI] [PubMed] [Google Scholar]
- 48.Yancik R, et al. Perspectives on comorbidity and cancer in older patients: approaches to expand the knowledge base. J Clin Oncol. 2001;19(4):1147–51. doi: 10.1200/JCO.2001.19.4.1147. [DOI] [PubMed] [Google Scholar]
- 49.Grunfeld E, Earle CC. The interface between primary and oncology specialty care: treatment through survivorship. J Natl Cancer Inst Monogr. 2010;2010(40):25–30. doi: 10.1093/jncimonographs/lgq002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Ngune I, et al. Predicting general practice attendance for follow-up cancer care. Am J Health Behav. 2015;39(2):167–74. doi: 10.5993/AJHB.39.2.2. [DOI] [PubMed] [Google Scholar]
- 51.Oeffinger KC, Argenbright KE, Levitt GA, McCabe MS, Anderson PR, Berry E, et al. Models of cancer survivorship health care: moving forward. Am Soc Clin Oncol Educ Book. 2014:205–13 [DOI] [PubMed]
- 52.Oeffinger KC, McCabe MS. Models for delivering survivorship care. J Clin Oncol. 2006;24(32):5117–24. doi: 10.1200/JCO.2006.07.0474. [DOI] [PubMed] [Google Scholar]
- 53.Rubin G, et al. The expanding role of primary care in cancer control. Lancet Oncol. 2015;16(12):1231–72. doi: 10.1016/S1470-2045(15)00205-3. [DOI] [PubMed] [Google Scholar]
- 54.Emery J, et al. Protocol for the ProCare Trial: a phase II randomised controlled trial of shared care for follow-up of men with prostate cancer. BMJ Open. 2014;4(3):e004972. doi: 10.1136/bmjopen-2014-004972. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Emery JD, Jefford M, King M, Hayne D, Martin A, Doorey J, et al. ProCare Trial: a phase II randomized controlled trial of shared care for follow-up of men with prostate cancer. BJU Int. 2017;119(3):381–9. doi: 10.1111/bju.13593. [DOI] [PubMed] [Google Scholar]
- 56.Wagner EH, Austin BT, Von Korff M. Organizing care for patients with chronic illness. Milbank Q. 1996;74(4):511–44. doi: 10.2307/3350391. [DOI] [PubMed] [Google Scholar]
- 57.Bodenheimer T, Wagner EH, Grumbach K. Improving primary care for patients with chronic illness: the chronic care model, part 2. JAMA. 2002;288(15):1909–14. doi: 10.1001/jama.288.15.1909. [DOI] [PubMed] [Google Scholar]
- 58.Coleman MP, et al. Cancer survival in Australia, Canada, Denmark, Norway, Sweden, and the UK, 1995–2007 (the International Cancer Benchmarking Partnership): an analysis of population-based cancer registry data. Lancet. 2011;377(9760):127–38. doi: 10.1016/S0140-6736(10)62231-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Ouwens M, et al. Integrated care programmes for chronically ill patients: a review of systematic reviews. Int J Qual Health Care. 2005;17(2):141–6. doi: 10.1093/intqhc/mzi016. [DOI] [PubMed] [Google Scholar]
- 60.Jiwa M, et al. Timely cancer diagnosis and management as a chronic condition: opportunities for primary care. Med J Aust. 2008;189(2):78–82. doi: 10.5694/j.1326-5377.2008.tb01921.x. [DOI] [PubMed] [Google Scholar]
- 61.Jefford M, et al. Tailored chemotherapy information faxed to general practitioners improves confidence in managing adverse effects and satisfaction with shared care: results from a randomized controlled trial. J Clin Oncol. 2008;26(14):2272–7. doi: 10.1200/JCO.2007.14.7710. [DOI] [PubMed] [Google Scholar]
- 62.Brown RF, et al. Education and role modelling for clinical decisions with female cancer patients. Health Expect. 2004;7(4):303–16. doi: 10.1111/j.1369-7625.2004.00294.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Barlow J, et al. Self-management approaches for people with chronic conditions: a review. Patient Educ Couns. 2002;48(2):177–87. doi: 10.1016/S0738-3991(02)00032-0. [DOI] [PubMed] [Google Scholar]
- 64.Deadman JM, et al. Taking responsibility for cancer treatment. Soc Sci Med. 2001;53(5):669–77. doi: 10.1016/S0277-9536(00)00369-5. [DOI] [PubMed] [Google Scholar]
- 65.Griffin SJ, et al. Effect on health-related outcomes of interventions to alter the interaction between patients and practitioners: a systematic review of trials. Ann Fam Med. 2004;2(6):595–608. doi: 10.1370/afm.142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Hodgkinson K, et al. The development and evaluation of a measure to assess cancer survivors’ unmet supportive care needs: the CaSUN (Cancer Survivors’ Unmet Needs measure) Psychooncology. 2007;16(9):796–804. doi: 10.1002/pon.1137. [DOI] [PubMed] [Google Scholar]
- 67.Ryan P, Lauver DR. The efficacy of tailored interventions. J Nurs Scholarsh. 2002;34(4):331–7. doi: 10.1111/j.1547-5069.2002.00331.x. [DOI] [PubMed] [Google Scholar]
- 68.Chan AW, et al. SPIRIT 2013 explanation and elaboration: guidance for protocols of clinical trials. BMJ. 2013;346:e7586. doi: 10.1136/bmj.e7586. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Moher D, Schulz KF, Altman D, CONSORT Group The CONSORT Statement: revised recommendations for improving the quality of reports of parallel-group randomized trials 2001. Explore (NY) 2005;1(1):40–5. doi: 10.1016/j.explore.2004.11.001. [DOI] [PubMed] [Google Scholar]
- 70.El-Shami K, et al. American Cancer Society colorectal cancer survivorship care guidelines. CA Cancer J Clin. 2015;65(6):428–55. doi: 10.3322/caac.21286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.".Cancer Council Australia. Publications. http://www.cancer.org.au/about-cancer/publications.html#jump_4. Accessed 2 Feb 2017.
- 72.Australian Cancer Survivorship Centre, Peter MacCallum Cancer Centre. I’m a survivor. https://www.petermac.org/services/support-services/australian-cancer-survivorship-centre/cancer-survivors. Accessed 17 Feb 2017.
- 73.Aaronson NK, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst. 1993;85(5):365–76. doi: 10.1093/jnci/85.5.365. [DOI] [PubMed] [Google Scholar]
- 74.Sprangers MA, te Velde A, Aaronson NK, European Organization for Research and Treatment of Cancer Study Group on Quality of Life The construction and testing of the EORTC colorectal cancer-specific quality of life questionnaire module (QLQ-CR38) Eur J Cancer. 1999;35(2):238–47. doi: 10.1016/S0959-8049(98)00357-8. [DOI] [PubMed] [Google Scholar]
- 75.Campbell HS, et al. Development and validation of the Short-Form Survivor Unmet Needs Survey (SF-SUNS) Support Care Cancer. 2014;22(4):1071–9. doi: 10.1007/s00520-013-2061-7. [DOI] [PubMed] [Google Scholar]
- 76.National Research Corporation . Development and validation of the Picker Ambulatory Oncology Survey Instrument in Canada: final report. Markham, ON, Canada: National Research Corporation; 2003. [Google Scholar]
- 77.Marshall GN, Hays RD. The Patient Satisfaction Questionnaire short-form (PSQ-18) Santa Monica, CA: RAND Corporation; 1994. [Google Scholar]
- 78.Norman GR, Sloan JA, Wyrwich KW. Interpretation of changes in health-related quality of life: the remarkable universality of half a standard deviation. Med Care. 2003;41(5):582–92. doi: 10.1097/01.MLR.0000062554.74615.4C. [DOI] [PubMed] [Google Scholar]
- 79.King MT, et al. QLU-C10D: a health state classification system for a multi-attribute utility measure based on the EORTC QLQ-C30. Qual Life Res. 2016;25(3):625–36. doi: 10.1007/s11136-015-1217-y. [DOI] [PubMed] [Google Scholar]
- 80.Briggs AH, Claxton K, Sculpher MJ. Decision modelling for health economic evaluation. New York: Oxford University Press; 2006. [Google Scholar]
- 81.McCabe MS, et al. American Society of Clinical Oncology statement: achieving high-quality cancer survivorship care. J Clin Oncol. 2013;31(5):631–40. doi: 10.1200/JCO.2012.46.6854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Ouwens M, et al. Implementation of integrated care for patients with cancer: a systematic review of interventions and effects. Int J Qual Health Care. 2009;21(2):137–44. doi: 10.1093/intqhc/mzn061. [DOI] [PubMed] [Google Scholar]
- 83.Klinkhammer-Schalke M, et al. Direct Improvement of Quality of Life in Colorectal Cancer Patients Using a Tailored Pathway with Quality of Life Diagnosis and Therapy (DIQOL): study and protocol for a randomised controlled trial. Trials. 2015;16(1):460–71. doi: 10.1186/s13063-015-0972-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Klinkhammer-Schalke M, et al. Direct improvement of quality of life using a tailored quality of life diagnosis and therapy pathway: randomised trial in 200 women with breast cancer. Br J Cancer. 2012;106(5):826–38. doi: 10.1038/bjc.2012.4. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) 2013 checklist: recommended items to address in a clinical trial protocol and related documents. (DOC 120 kb)
Participant information sheet/consent form. (DOCX 55 kb)
Medicare consent form. (DOCX 33 kb)
Data Availability Statement
Not applicable.