

Waldenström macroglobulinemia (WM) is characterized by bone marrow (BM) infiltration of monoclonal Immunoglobulin M (IgM) secreting lymphoplasmacytic lymphoma (LPL), and typically presents with anemia. MYD88 and CXCR4 activating somatic mutations (CXCR4MUT) are common in WM, and found in 90–95% and 35–40% of WM patients, respectively.1–3 Activating mutations in MYD88 support tumor growth via nuclear factor kappa-light-chain enhancer-of-activated B-cells (NF-κB), which is triggered by Interleukin (IL)-1 receptor-associated kinases (IRAK4/IRAK1) and Bruton’s tyrosine kinase (BTK).4 A distinct transcriptome signature based on both MYD88 and CXCR4 mutation status has been observed.5
Ibrutinib is a BTK inhibitor that is approved for the treatment of WM. Ibrutinib is highly active in WM patients, and responses are impacted by both MYD88 and CXCR4 mutation status. Patients with MYD88WTlack major responses, while those with mutated MYD88 show decreased response rates, and delayed time to response if carrying a CXCR4 mutation.2,6 Importantly, rapid improvements in hemoglobin levels were observed even in patients with modest or no changes in BM tumor infiltration, suggesting a contributing mechanism in addition to tumor debulking.6 Anemia in some WM patients may be related to elevated hepcidin levels produced by LPL cells.7 However, the effect of ibrutinib on hepcidin remains unknown. Serum cytokines are important in WM biology and can be produced either by the malignant cells, the surrounding microenvironmental cells, as well as by cells of the immune system.8 The anti-tumor effect of ibrutinib may impact all of these compartments, including cytokines that may support growth and survival of tumor cells, and contribute to morbidity in WM, including anemia.9,10 As such, we aimed to characterize the serum cytokine profile in WM patients based on MYD88 and CXCR4 mutation status, and to characterize serum cytokine and hepcidin changes in response to ibrutinib therapy.
We first analyzed off-therapy samples of 86 WM patients, 52 previously untreated, and 34 previously treated patients, including three mutational subgroups: MYD88L265P/CXCR4WT (n=45), MYD88L265P/CXCR4MUT (n=32) and MYD88WT/CXCR4WT (n=9), including 12 patients with frameshift and 20 patients with nonsense CXCR4 mutations. Samples from 20 age- and sex-matched healthy donors (HD) were used for comparison. We then analyzed serial samples of 29 relapsed and/or refractory patients who received ibrutinib therapy on a prospective clinical trial, and for whom baseline and post-treatment serum samples taken one year after initiation of therapy were available.6 These included three mutational subgroups: MYD88L265P/CXCR4WT (n=19), MYD88L265P/CXCR4MUT (n=9) and MYD88WT/CXCR4WT (n=1). All consecutive patients participating in this trial at the DFCI were included, apart from ten patients who were missing samples, and four patients who went off trial within the first year (see Online Supplementary Material). A total of 24 cytokines were analyzed, including soluble CD27 as a known biomarker in WM (details in Online Supplementary Material). Hepcidin was measured as previously described.11 Iron-related parameters (iron, ferritin, transferrin) were tested at the St. Antonius Hospital, using the cobas 6000 analyzer. Statistical analysis was performed with R software (R Core Team (2015) R: A language and environment for statistical computing). As previously described, allele-specific polymerase chain reaction (PCR) was used to detect MYD88L265P and CXCR4 mutations.6 Additional Sanger sequencing was performed for CXCR4. Clinical response to ibrutinib at one year was determined using consensus-based response criteria, wherein major response includes complete, very good partial or partial responses, and non-major response includes minor response, stable disease or progressive disease.12 Clinical parameters and cytokine levels were analyzed following log2 transformation. Correlation was tested using Spearman’s rho, and when appropriate the Holm-Bonferroni multiple-hypothesis correction procedure was applied. Adjusted P-values <0.05 were deemed significant. The Dana-Farber/Harvard Cancer Center (DF/HCC) Institutional Review Board approved the study.
For all 86 WM patients, the median age was 63 (range: 31–94 years); median BM infiltration was 58% (range: 3–95%); serum IgM level was 3,632 (range: 134–7,400 mg/dL); and 64/86 (74%) patients were male. The median age of the HD was 57 (38–80 years), and 15/20 (75%) were male. Compared to HD, CXCL10 (+1.7-fold; P=0.004), IL10 (+13.9; P<0.001), IL2RA (+4.3-fold; P<0.001), CXCL13 (+33.8-fold; P<0.001) and sCD27 (+174.1-fold; P<0.001) were significantly higher in WM patients, regardless of prior therapy status (Table 1; Figure 1A). In WM patients, serum levels of CXCL13, IL2RA and sCD27 strongly correlated with hemoglobin levels with correlation coefficients of −0.55, −0.55, and −0.47, respectively (P<0.001 for all comparisons; Figure 1B). Serum CXCL13 (rho=0.56; P<0.001) and sCD27 (rho=0.46; P<0.001) levels correlated with BM infiltration (Figure 1C), whereas no cytokine significantly correlated with serum IgM levels.
Table 1.
Summary of cytokine findings in WM patients (all, untreated and previously treated) versus healthy donors
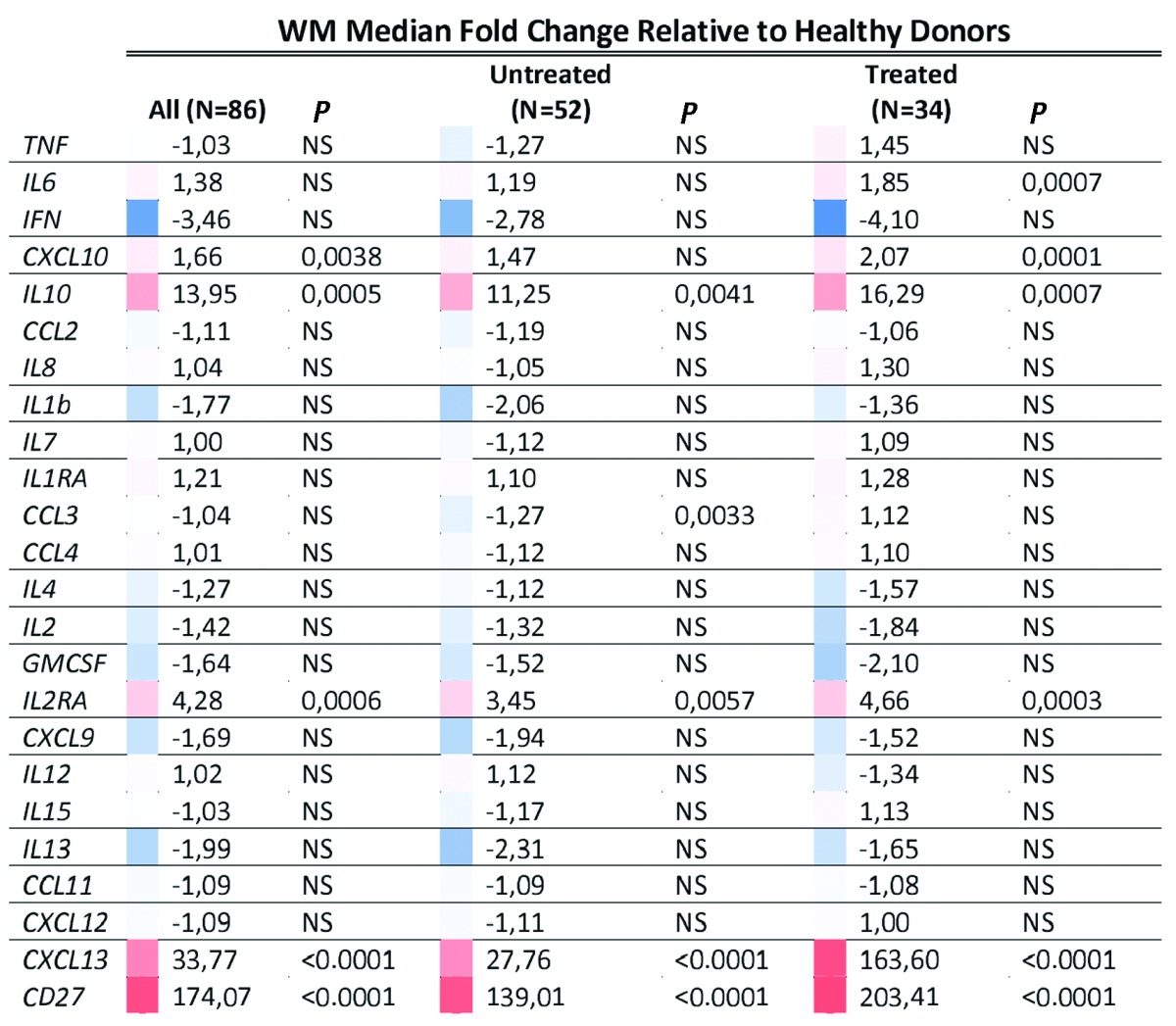
Figure 1.

Serum cytokine levels in WM patients and healthy donors. Serum levels for the five cytokines that were different between 86 (52 untreated and 34 previously treated) WM patients and 20 healthy donors. Data represents log2-transformed fold change values relative to the median of the healthy controls. All P-values were adjusted using Holm-Bonferroni correction for multiple hypothesis testing. A) All five cytokines were increased in WM patients with median levels of CD27 174.1-fold (P<0.001), IL2RA 4.3-fold (P<0.001), IL10 13.9-fold (P<0.001), CXCL13 33.8-fold (P<0.001) and CXCL10 1.7-fold (P=0.004) increased over median healthy donor concentrations. B) Log2-transformed CXCL13 levels positively correlated with percentage of WM bone marrow involvement (Spearman’s rho=0.562; P<0.001). C) Hemoglobin levels negatively correlated with CXCL13 levels (Spearman’s rho=0.567; P<0.001). WM: Waldenström macroglobulinemia.
We subsequently looked at cytokine differences between mutational subgroups in the WM patients. Although IL6 levels were not significantly different between all WM patients and HD, significantly higher IL6 levels were observed among MYD88L265PCXCR4WT patients compared to HD (+1.8-fold; P=0.001). Moreover, among MYD88L265P mutated patients, IL2RA (+2.2-fold; P=0.025), IL1RA (+1.5-fold; P=0.003), CXCL10 (+1.5-fold; P=0.026) and sCD27 (+1.7-fold; P=0.016) were higher in CXCR4WT versus CXCR4MUT patients. IL1RA (P=0.011) and CXCL13 (P=0.016) were also lower among CXCR4 frameshift but not CXCR4 nonsense mutated patients versus those who were CXCR4WT. We found no differences in cytokines between those patients with symptomatic (n=28) and asymptomatic (n=24) disease in the previously untreated group. All previously treated patients had symptomatic disease.
We next analyzed the samples of 29 previously treated, symptomatic WM patients who participated in a prospective clinical trial with single agent ibrutinib.6 Twelve of 24 cytokines showed a significant change following one year on ibrutinib (Figure 2A). Among these cytokines, TNF-α (−1.6-fold), IL2RA (−2.2-fold) and CXCL13 (−38.2-fold) showed the most significant decrease (P<0.001 for all). Of the cytokines evaluated, only baseline CXCL13 was associated with attainment of a major response after one year on ibrutinib: at baseline, CXCL13 was 451.6-fold higher in patients who achieved major responses versus those without a major response (P=0.049; Figure 2B). Following treatment at one year, a significantly greater decrease in CXCL13 levels was observed in patients who attained a major response (−306.9-fold) versus those who did not (−2.3-fold) (P=0.019; Figure 2C). These findings were also true using logistic regression to account for age, sex, MYD88 and CXCR4 mutational status (including the distinction between CXCR4 frameshift and nonsense mutations), and baseline BM involvement (P=0.035 for baseline CXCL13, P=0.005 for change in CXCL13). CXCL13 levels did not differ based on CXCR4 mutational status (P=0.199). Changes in CXCL13 correlated with changes in hemoglobin (rho=−0.64; P=0.005; Figure 2D) and serum IgM levels (rho=0.68; P=0.002; Figure 2E).
Figure 2.

CXCL13 response to ibrutinib therapy. Serum cytokine levels were assessed for 29 WM patient samples prior to the start of ibrutinib therapy and again after one year of therapy with ibrutinib. A) A row scaled heat map sorted by clinical response to ibrutinib at one year and statistical significance of the cytokine change demonstrating decreasing CXCL13 and increasing CCL11 levels following therapy. B) Baseline levels of CXCL13 were higher in patients who ultimately achieved a major response following one year of ibrutinib therapy (P=0.049). C) Changes in CXCL13 levels at one year were also greater in those patients obtaining a major response versus patients who did not achieve a major response (P=0.019). D) Changes in CXLC13 levels correlated with hemoglobin levels (Spearman’s rho=−0.64; P=0.005). E) Changes in CXCL13 levels also correlated with serum IgM response to ibrutinib (rho=0.68; P=0.002). IgM: Immunoglobulin M; HGB: Hemoglobin; SD: stable disease; MR: minor response; PR: partial response; VGPR: very good PR.
We also studied changes in hepcidin levels to clarify whether improvements in anemia following ibrutinib were related to this protein. At baseline, hepcidin levels correlated with hemoglobin levels (rho −0.39, P=0.02), but not with serum IgM, BM infiltration, or other cytokines evaluated. After one year of ibrutinib, median hepcidin levels decreased from 67 (range: 17.5–527.2 ng/ml) to 49 (range: 8.9–225 ng/ml; P=0.013); however there were no significant differences in decrease between patients with or without a major response, nor did they correlate with changes in hemoglobin, serum IgM or BM tumor involvement (data not shown).
The differences in cytokine levels that we observed between HD and WM patients were generally consistent with previous findings in WM,8 although these studies did not account for MYD88 and CXCR4 mutation status. Several cytokines were found to be lower in MYD88L265PCXCR4MUT versus MYD88L265PCXCR4WTpatients, which may relate to the suppression of MYD88L265P induced inflammatory pathways in patients with MYD88L265PCXCR4MUT status, as found in a recent transcriptome study.5
This is the first report on inflammatory cytokine changes following ibrutinib therapy in WM, and our findings parallel changes observed in CLL patients on ibrutinib therapy for CXCL13, IL8, CXCL10, CCL4, CCL11, IL1RA, and TNF-α.9 These changes may be related to on-target tumor effects leading to decreased cytokine production by LPL cells and/or the impact of ibrutinib on microenvironmental cells such as T cells and macrophages. Although hepcidin levels showed a modest decrease, changes in hepcidin or BM infiltration did not account for the robust improvements in hemoglobin levels observed in ibrutinib-treated WM patients.
An important finding was the behavior of CXCL13 as a robust predictive marker of major response to ibrutinib in WM. A high CXCL13 at baseline was a strong predictor of achieving a partial response (PR) or better after one year, and major responses were associated with a deep suppression of CXCL13 levels. To our knowledge there are no published data on the qualities of CXCL13 as a predictive marker of response to ibrutinib in CLL or other B-cell malignancies. CXCL13 is a chemokine that is expressed in lymphoid organs by follicular dendritic cells and macrophages, and is produced by LPL cells.5 CXCL13 attracts mast cells to the microenvironment in angioimmunoblastic T-cell lymphoma.13 Excessive BM mast cells are a known disease characteristic of the WM BM niche, and may provide support for WM cell growth and survival through CD40L and sCD27-CD70 interaction.14 In CLL, ibrutinib has been shown to strongly inhibit CXCL13 mediated adhesion of CLL cells to the BM and lymph node microenvironment, including interaction with macrophages.9,15 Our data suggest a role for CXCL13 in WM tumor biology and sensitivity to ibrutinib therapy, and warrant further investigation as a biomarker for ibrutinib therapy as well as a potential therapeutic target.
Supplementary Material
Footnotes
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Treon SP, Xu L, Yang G, et al. MYD88 L265P Somatic Mutation in Waldenström’s Macroglobulinemia. N Engl J Med. 2012;367(9):826–833. [DOI] [PubMed] [Google Scholar]
- 2.Treon SP, Xu L, Hunter Z. MYD88 Mutations and Response to Ibrutinib in Waldenström’s Macroglobulinemia. N Engl J Med. 2015;373(6):584–586. [DOI] [PubMed] [Google Scholar]
- 3.Xu L, Hunter ZR, Tsakmaklis N, et al. Clonal architecture of CXCR4 WHIM-like mutations in Waldenström Macroglobulinaemia. Br J Haematol. 2016;172(5):735–744. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Yang G, Zhou Y, Liu X, et al. A mutation in MYD88 (L265P) supports the survival of lymphoplasmacytic cells by activation of Bruton tyrosine kinase in Waldenstrom macroglobulinemia. Blood. 2013;122(7):1222–1232. [DOI] [PubMed] [Google Scholar]
- 5.Hunter ZR, Xu L, Yang G, et al. Transcriptome sequencing reveals a profile that corresponds to genomic variants in Waldenstrom macroglobulinemia. Blood. 2016;128(6):827–838. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Treon SP, Tripsas CK, Meid K, et al. Ibrutinib in previously treated Waldenström’s macroglobulinemia. N Engl J Med. 2015;372(15):1430–1440. [DOI] [PubMed] [Google Scholar]
- 7.Ciccarelli BT, Patterson CJ, Hunter ZR, et al. Hepcidin is produced by lymphoplasmacytic cells and is associated with anemia in Waldenström’s macroglobulinemia. Clin Lymphoma Myeloma Leuk. 2011;11(1):160–163. [DOI] [PubMed] [Google Scholar]
- 8.Elsawa SF, Novak AJ, Ziesmer SC, et al. Comprehensive analysis of tumor microenvironment cytokines in Waldenstrom macroglobulinemia identifies CCL5 as a novel modulator of IL-6 activity. Blood. 2011;118(20):5540–5549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Niemann CU, Herman SEM, Maric I, et al. Disruption of in vivo Chronic Lymphocytic Leukemia tumor-microenvironment interactions by ibrutinib - findings from an investigator-initiated phase II study. Clin Cancer Res. 2016;22(7):1572–1582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.de Rooij MFM, Kuil A, Kraan W, et al. Ibrutinib and idelalisib target B cell receptor- but not CXCL12/CXCR4-controlled integrin-mediated adhesion in Waldenstrom macroglobulinemia. Haematologica. 2016;101(3) e111–e115 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ganz T, Olbina G, Girelli D, Nemeth E, Westerman M. Immunoassay for human serum hepcidin. Blood. 2008;112(10): 4292–4297. [DOI] [PubMed] [Google Scholar]
- 12.Owen RG, Kyle RA, Stone MJ, et al. Response assessment in Waldenström macroglobulinaemia: update from the VIth International Workshop. Br J Haematol. 2013;160(2):171–176. [DOI] [PubMed] [Google Scholar]
- 13.Tripodo C, Gri G, Piccaluga PP, et al. Mast cells and Th17 cells contribute to the lymphoma-associated pro-inflammatory microenvironment of angioimmunoblastic T-cell lymphoma. Am J Pathol. 2010;177(2):792–802. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ho AW, Hatjiharissi E, Ciccarelli BT, et al. CD27-CD70 interactions in the pathogenesis of Waldenstrom macroglobulinemia. Blood. 2008;112(12):4683–4690. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.de Rooij MFM, Kuil A, Geest CR, et al. The clinically active BTK inhibitor PCI-32765 targets B-cell receptor- and chemokine-controlled adhesion and migration in chronic lymphocytic leukemia. Blood. 2012;119(11):2590–2594. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.