

Abstract
Background
Accumulating evidence from medical workforce research indicates that poor work/life balance and increased work/home conflict induce psychological distress. In this study we aim to examine the existence of a priority gap between ideal and real lives, and its association with psychological burnout among academic professionals.
Methods
This cross-sectional survey, conducted in 2014, included faculty members (228 men, 102 women) at a single medical university in Tokyo, Japan. The outcome of interest was psychological burnout, measured with a validated inventory. Discordance between ideal- and real-life priorities, based on participants’ responses (work, family, individual life, combinations thereof), was defined as a priority gap.
Results
The majority (64%) of participants chose “work” as the greatest priority in real life, but only 28% chose “work” as the greatest priority in their conception of an ideal life. Priority gaps were identified in 59.5% of respondents. A stepwise multivariable general linear model demonstrated that burnout scores were associated positively with respondents’ current position (P < 0.0018) and the presence of a priority gap (P < 0.0001), and negatively with the presence of social support (P < 0.0001). Among participants reporting priority gaps, burnout scores were significantly lower in those with children than in those with no children (P interaction = 0.011); no such trend was observed in participants with no priority gap.
Conclusions
A gap in priorities between an ideal and real life was associated with an increased risk of burnout, and the presence of children, which is a type of “family” social support, had a mitigating effect on burnout among those reporting priority gaps.
Keywords: Academic professions, Children Psychological burnout, Priority gap between ideal and real lives, Social support
Background
Burnout is a disastrous condition characterized by physical, emotional, and mental exhaustion that can be caused by emotional damage [1]. Accumulating evidence from medical workforce research indicates that poor work/life balance and increased work/home conflict induce psychological distress, characterized by anxiety, stress, broken relationships, depression, and/or burnout [2–4]. Burnout syndrome can affect individuals in a variety of professions that require intense interaction with other people, such as police officers, social workers, and nurses. Its consequences may be particularly important in the medical field; it has been associated with an increased risk of medical errors [5], suboptimal patient care [6], and reduced patient satisfaction. Burnout can also affect medical professionals’ personal lives, including relationships and activities outside the professional domain, often propelling them to consider early retirement [7]. Although associated factors and methods of resolving burnout have been discussed for a long time, no clear conclusion has been reached.
In this study, we focused on academic faculty members at a single medical university in Tokyo, Japan. As noted recently in Nature, young researchers are often excluded from Japanese universities and the number of young faculty members at these institutions is declining [8]. In addition, the number of publications originating from Japanese universities, companies, and organizations decreased by 4.3% between 2006 and 2010, whereas the numbers of such publications originating from the UK and Germany increased by 12.7 and 15%, respectively, during the same time period [9]. In Japan, obtaining academic employment related to medicine is known to be highly competitive, and the work required to retain such a position is known to be demanding. Thus, we hypothesized that the priority gap between conceptions of an ideal life and real life would create psychological distress in this population. Although few studies have examined this issue, one survey of psychiatrists working at medical schools throughout Japan demonstrated that difficulty with work/life balance and less work-environment satisfaction were associated significantly with greater emotional exhaustion [8]. Hence, the purpose of this study was to investigate the effect of an ideal-/real-life priority gap on burnout among academic faculty members at one medical university.
Methods
Participants
This cross-sectional survey was conducted at one university and one affiliated hospital from January to March 2014. We consecutively recruited 1189 faculty members, 1235 medical staff members, and 266 clerks. Of those who returned questionnaires, we excluded hospital workers (i.e., nurses, pharmacists, technicians, and clerks). Thus, the final sample consisted of 330 academic faculty members (228 men, 102 [31%] women), 54% of whom were aged 50–65 years (response rate, 27.8%). The participants worked in the following departments: Medicine (n = 94 [28.5%]), Medical Technology (n = 67 [20.3%]), Science and Engineering (n = 36 [10.9%]), Pharmacology (n = 28 [8.5%]), Economics (n = 26 [7.9%]), Literature (n = 22 [6.7%]), Education (n = 17 [5.2%]), Law (n = 9 [2.7%]), other (n = 17 [5.2%]), and not specified (n = 14 [4.1%]. The institutional review board of Teikyo University School of Medicine approved this study (no. 13–1310).
Measures
Outcome
The outcome of interest was burnout, measured by a 17-item inventory, developed originally for the assessment of workplace burnout by Maslach and Jackson [10] and translated into Japanese by Tao and Kubo [11]. Item responses are structured by a five-point Likert scale. Total scores range from 17 to 85, with higher scores indicating a greater risk of burnout.
Burnout was defined as a syndrome characterized by lack of interest in/enthusiasm for work (emotional exhaustion), a tendency to treat people as if they were impersonal objects (depersonalization), and a sense that one’s work is not meaningful or important (low sense of personal accomplishment).
Exposure
Priorities in a conception of ideal life and in real life were measured by asking participants, “What do you want to prioritize in your life?” and, “What do you prioritize in real life?,” respectively. Response choices included work, family, individual life, and combinations thereof. We also asked participants, “What do you want your partner to prioritize in your ideal life?” and, “What does your partner prioritize in your real life?” Differences in responses about ideal and real lives were used to define priority gaps.
Covariates
Covariates used in this study were gender, age, marital status, presence/absence of children, partner’s occupation (employed/homemaker or unemployed), current position (professor/associate professor/lecturer/assistant professor/instructor), and household income (upper/upper middle/middle/lower middle/lower). Household was measured by asking “Suppose if annual individual income is classified into five ranks, which categories do you think your income falls in?” We also asked about the average number of hours per day spent working at the workplace and in the household, and about social support. Social support scores were calculated using the 15-item Social Support Questionnaire originally developed by Sarason [12]. Questionnaire scores range from 15 to 75, with higher scores indicating more support.
Statistical analyses
Baseline characteristics and working conditions of men and women were compared using the t-test for continuous variables and the chi-squared test for categorical variables. We estimated regression coefficients and standard errors of each variable associated with the total burnout score using univariate and multivariate general linear models. Stepwise model selection was performed using the SAS glmselect procedure, and the final model was determined using Akaike’s information criterion. Selection was performed in three steps: the initial model included all explanatory variables, the second model included selected variables from the first model and all potential interaction terms between these variables (forced inclusion), and the final model included selected variables and interaction terms without forced inclusion. All analyses were performed using SAS software (version 9.3; SAS Institute Inc., Cary, NC, USA), with a two-tailed significance level of P < 0.05.
Results
Table 1 shows participants’ baseline characteristics and working conditions according to gender. Women were more likely than men to be single (P = 0.008), to have employed spouses (P < 0.001), to report personal and partner priority gaps (P = 0.002 and P < 0.001, respectively), and to work longer at the workplace and at home (P = 0.001). Women were also less likely to have children (P = 0.002) and to hold positions higher than lecturer (P < 0.001).
Table 1.
Baseline characteristics and working conditions according to gender
| Total (%) n = 328 | Women (%) n = 102 | Men (%) n = 228 | P-value | |
|---|---|---|---|---|
| Marital status | 0.008 | |||
| Married | 262 (79) | 72 (71) | 190 (83) | |
| Single (Including Divoced or Widowed) | 68 (21) | 30 (29) | 38 (17) | |
| Presence of children | 0.002 | |||
| No | 118 (36) | 49 (48) | 69 (30) | |
| Yes | 211 (64) | 53 (52) | 158 (70) | |
| Age group | 0.077 | |||
| 20s or 30s | 66 (20) | 27 (27) | 39 (17) | |
| 40s | 84 (26) | 28 (27) | 56 (25) | |
| 50s or more | 179 (54) | 47 (46) | 132 (58) | |
| Spouse’s employment | <0.001 | |||
| Employed | 164 (63) | 69 (96) | 95 (50) | |
| Unemployed | 98 (37) | 3 (4.2) | 95 (50) | |
| Current position | <0.001 | |||
| Lecturer or upper | 252 (76) | 65(64) | 187 (82) | |
| Assistant or lower | 78 (24) | 37 (36) | 41 (18) | |
| Household income | 0.350 | |||
| Upper | 168 (51) | 46 (46) | 122 (53) | |
| Middle | 119 (36) | 42 (42) | 77 (34) | |
| Lower | 41 (13) | 12 (12) | 29 (13) | |
| Gap of priority between ideal and real lives | 0.007 | |||
| No | 133 (41) | 29 (28) | 104 (46) | |
| Yes | 195 (59) | 73 (72) | 122 (54) | |
| Gap of priority in a partner between ideal and real lives | <0.001 | |||
| No | 125 (47) | 21 (29) | 104 (54) | |
| Yes | 140 (53) | 52 (71) | 88 (46) | |
| Work hours (means ± SD) | 0.021 | |||
| 9.7 ± 2.1 | 9.3 ± 1.8 | 9.8 ± 2.2 | ||
| Hours of house chores (means ± SD) | 0.001 | |||
| 11.3 ± 2.3 | 11.9 ± 2.0 | 11.1 ± 2.3 | ||
| Social support (means ± SD) | 0.180 | |||
| 54.2 ± 12.8 | 55.6 ± 12.9 | 53.5 ± 12.8 |
Any categories which does not become 100% has missing values
Household income was grouped into three categories (i.e., “upper/upper middle”, “middle”, “lower middle/lower”
Table 2 shows data on discordance between ideal- and real-life priorities. Responses from 195/328 (59.5%) participants revealed priority gaps. Significantly more participants (n = 209 [64.0%]) chose “work” as the greatest priority in real life compared to the situation in an ideal life (28.0%). This result was not changed by the exclusion of “do not know” responses from the analyses.
Table 2.
Contingency table of priority in between real and ideal life
| Priority in real life | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| work | family | individual | work & family | work & individual | family & individual | three of work, family, and individual | do not know | total | ||
| Priority in ideal life | work | 58 (27.8) | 0 | 0 | 0 | 1 (7.7) | 0 | 0 | 0 | 59 |
| family | 9 (4.3) | 1 (12.5) | 0 | 2 (2.6) | 0 | 0 | 0 | 0 | 12 | |
| individual | 1 (0.5) | 0 | 0 | 0 | 2 (15.4) | 0 | 0 | 0 | 3 | |
| work & family | 77 (36.8) | 7 (87.5) | 0 | 55 (70.5) | 0 | 0 | 0 | 2 (33.3) | 141 | |
| work & individual | 11 (5.3) | 0 | 1 (100) | 2 (2.6) | 5 (38.5) | 0 | 0 | 0 | 19 | |
| family & individual | 5 (2.4) | 0 | 0 | 0 | 1 (7.7) | 0 | 0 | 1 (16.7) | 7 | |
| three of work, family, and individual | 44 (21.1) | 0 | 0 | 19 (24.4) | 4 (30.8) | 1 (100) | 12 (100) | 1 (16.7) | 81 | |
| do not know | 4 (1.9) | 0 | 0 | 0 | 0 | 0 | 0 | 2 (33.3) | 6 | |
| total | 209 | 8 | 1 | 78 | 13 | 1 | 12 | 6 | 328 | |
Table 3 shows the results of the univariate general linear model for burnout. Significant variables in this model were gender (P = 0.036), marital status (P = 0.001), presence of children (P < 0.001), age group (P = 0.003), current position (P < 0.001), household income (P < 0.001), personal and partner priority gaps (P < 0.001 and P = 0.022, respectively), and workplace/household working hours (P = 0.004).
Table 3.
General linear models of an effect of covariates on burnout, both univariate and multivariate models
| Univariate | Multivariate (Stepwise model) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Model 1 n = 302、R2 = 0.23 | Model 2 n = 301、R2 = 0.25 | ||||||||
| Point estimate | SE | P-value | Point estimate | SE | P-value | Point estimate | SE | P-value | |
| Sex | 0.033 | ||||||||
| Women | 2.8 | 1.3 | |||||||
| Men | - | - | |||||||
| Marital status | 0.002 | ||||||||
| Married | 4.5 | 1.5 | |||||||
| Single (including Divoced or Widowed) | - | - | |||||||
| Presence of children | <0.001 | 0.005 | 0.960 | ||||||
| No | 4.9 | 1.2 | 3.4 | 1.2 | 0.1 | 1.8 | |||
| Yes | - | - | - | - | |||||
| Age group | 0.005 | ||||||||
| 20s or 30s | 4.1 | 1.6 | |||||||
| 40s | 3.9 | 1.4 | |||||||
| 50s or more | - | - | |||||||
| Spouse’s employment | 0.380 | ||||||||
| Unemployed | 1.1 | 1.3 | |||||||
| Employed | - | - | |||||||
| Current position | <0.001 | 0.014 | 0.002 | ||||||
| Assistant or lower | 5.9 | 1.4 | 4.5 | 1.4 | 4.3 | 1.4 | |||
| Lecturer | - | - | - | - | |||||
| Household income | |||||||||
| Lower | 8.7 | 1.9 | <0.001 | ||||||
| Middle | 2.2 | 1.3 | |||||||
| Upper | - | - | |||||||
| Gap of priority between ideal and real lives | <0.001 | <0.001 | <0.001 | ||||||
| Yes | 7.0 | 1.2 | 6.2 | 1.1 | 10 | 1.9 | |||
| No | - | - | - | - | - | - | |||
| Gap of priority in a partner between ideal and real lives | 0.022 | ||||||||
| Yes | 2.8 | 1.2 | |||||||
| No | - | - | |||||||
| Work hours | 0.300 | ||||||||
| More than 8 h | 2.0 | 1.9 | |||||||
| Less than 8 h | |||||||||
| Hours of house chores (means ± SD) | - | - | 0.003 | ||||||
| More than 8 h | 4.2 | 1.4 | |||||||
| Less than 8 h | - | - | |||||||
| Social Support | −0.28 | 0.045 | <0.001 | −0.22 | 0.043 | <0.001 | −0.21 | 0.043 | <0.001 |
| Statistical interaction | |||||||||
| Presence of children × Presence of WLB gap | −5.9 | 2.3 | 0.011 | ||||||
In the multivariate analysis, including all explanatory variables (model 1), the presence of children, current position, and priority gap were significant. In model 2, constructed by forced inclusion of these variables and all potential interactions between them, the priority gap, presence of children, current position, and interaction between the priority gap and presence of children were significant. In the final model, which included these variables and interaction terms and was analyzed by stepwise selection without forced inclusion, the same variables were significant in both model 1 and model 2. Burnout scores were ten times higher among respondents reporting priority gaps than among those reporting no gap (P < 0.001; Table 3).
Among participants reporting priority gaps, burnout scores were significantly lower in those with children than in those with no children (β = −5.9, P interaction = 0.011). Burnout scores were similar among those reporting no priority gap, with and without children (β = −0.096, P = 0.96). (Fig. 1).
Fig. 1.
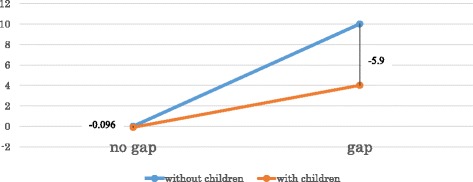
An effect of WLB gap on burnout (with or without children)
Discussion
Approximately 60% of participants in this study reported discordance between ideal- and real-life priorities. Burnout scores were associated positively with current position and this priority gap, and negatively with the presence of social support. Among participants of both genders reporting priority gaps, the presence of children had a mitigating effect on the burnout score.
In general, the presence of children is thought to be a cause of work/home conflict, which can provoke burnout [13]. Previous researchers [14] have found that perceived social support can affect individuals’ emotional well-being, in agreement with our results. The perceived social support factors of “family” and “friends” have consistently shown the strongest associations with symptomatology, such as depressed psychological state, in college students (n = 549) and psychiatric outpatients (n = 156) [15]. Umene et al. [8] demonstrated that social support had a mitigating effect on burnout, which was associated significantly with poor work/life balance and the number of nights worked per month. Our finding that the presence of children mitigated psychological burnout suggests that emotional support from children is a type of “family” social support, which appears to have a good influence on the mental health of faculty researchers, helping to alleviate work-related psychological stress.
Previously, we demonstrated that early pregnancy age among female doctors was associated with less likelihood of attaining a board specialty or DMSc [16], suggesting that those whose careers are not yet established should use caution when deciding whether to have a child at an earlier age. The gender division of labor is embedded strongly in the mindset of Japanese culture, and finding a balance between career development and child rearing is very difficult, especially for women [17]. In addition, this study found that higher position like “professor” is negatively associated with burnout. Because we confirmed that women were less likely to be in higher position, female faculties and especially those who had children are thought to be vulnerable to burnout. In this regard, having a child can be a double-edged sword; it negatively affects young female health professionals, who are required to study and rear children at the same time [16], but it may positively affect workers with perceived priority gaps.
Psychological burnout is a known risk factor for quitting one’s job or choosing early retirement, especially among women. Solutions for psychologically vulnerable workers that have been presented in the literature include mentorship and coaching, recently considered to be among the most powerful tools to help keep female health professionals working [13]. In addition, although very few studies have investigated the usefulness of “work/life balance interventions”, Fortney et al. [18] reported that a self-efficacy intervention involving training in mindfulness practice positively affected job satisfaction, quality of life, and compassion in the context of work; alleviated burnout and stress; and amplified resilience and empathy.
Due to the gender division of labor, the acquisition rate of child-care leave differs dramatically between men and women (1.7 and 86%, respectively) [19]. Johhanson et al. [20] pointed out the importance of preparation classes for reassurance and the acquisition of child-raising skills for fathers, and argued that policy makers and health-care providers should offer this kind of support, as it benefits not only men but also their children and partners, and ultimately helps to encourage egalitarian practices at home and work. Even in Sweden, one of the most advanced countries in the world in terms of welfare, fathers’ participation in child rearing remains a concern. Despite the inherent difficulties, policy makers in Japan should make further efforts, using multidirectional approaches to support female and male workers’ ability to continue work and develop careers.
This study has several limitations. First, it involved a small sample of participants from a single private medical university. Our participants were likely to have heavy workloads, which is often the case in the highly competitive work environment of academic medicine in Japan. Compared with respondents in a survey conducted by the Japanese Cabinet Office using the same items as in this study [21], more of our participants chose “work” (49% vs. 64%) and fewer chose “family” (19% vs. 2.5%) as the greatest real-life priority. Hence, our results require careful interpretation.
Second, our analyses examined only overall burnout scores. Many studies of burnout have involved the analysis of associations of individual burnout factors (emotional exhaustion, depersonalization, and low personal accomplishment) with covariates. We conducted such analyses, but they yielded no remarkable finding beyond the results of overall analyses. In addition, because such detailed analysis makes interpretation of the results complicated and difficult, we presented data only on overall burnout scores. Third, our result might have been different according to types of medical profession like medical doctors, nurses, or other health professions. This speculation however, could not be verified due to insufficient numbers of the responses.
Conclusion
We found that burnout scores were higher among participants reporting ideal-/real-life priority gaps than among those with no gap, in analyses adjusted for covariates. In addition, the presence of children had a mitigating effect on burnout. Child rearing is time consuming, especially when the child is small, but the presence of children later in life may mitigate psychological stress among parents in the workforce. The results of this study imply that the presence of children plays an important role in alleviating psychological stress not only among female but also among male faculty members.
Acknowledgements
We thank the faculty members in Teikyo University for participating in this research.
Funding
Kyoko Nomura has received research grants from the Ministry of Education, Science, Sports and Culture, Grant in Scientific Research (B), Number 16H05262 and Grant in Scientific Research (C), Number 25460814.
Availability of data and materials
The datasets generated and/or analysed during the current study are not publicly available due to including the privacy of participants but are available from the corresponding author on reasonable request.
Authors’ contributions
YC: contributed to the study design, developed database, statistical analysis and drafted manuscript; KN: contributed to the study conceptualization, design, developed database, statistical analysis, edited manuscript and had primary responsibility for the final content of the manuscript; HS, KT, MT and YS: contributed to the study conceptualization, design, and developed database; ST: provided constructive feedback on each draft of the manuscript; AM, HH, HO and DS: contributed to drafting the manuscript and the bibliography. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable
Ethics approval and consent to participate
This study was approved by the ethics committee of Teikyo University School of Medicine, Tokyo, Japan (TU-COI 14–109).
References
- 1.Maslach C, Jackson S, Leiter M. Maslach Burnout Inventory Manual (3rd ed). California: Consulting Psychologists Press; 1996. p. 191–218.
- 2.Nitzsche A, Driller E, Kowalski C, Ansmann L, Pfaff H. The conflict between work and private life and its relationship with burnout - results of a physician survey in breast cancer centers in North Rhine-Westphalia. Gesundheitswesen. 2013. doi:10.1055/s-0033-1337996. [DOI] [PubMed]
- 3.Shanafelt TD, Boone S, Tan L, Dyrbye LN, Sotile W, Satele D, West CP, Sloan J, Oreskovich MR. Burnout and satisfaction with work-life balance among US physicians relative to the general US population. Arch Intern Med. 2012;172:1377–85. doi: 10.1001/archinternmed.2012.3199. [DOI] [PubMed] [Google Scholar]
- 4.Cossman JS, Street D. Mississippi burnout part II: satisfaction, autonomy and work/family balance. J Miss State Med Assoc. 2009;50:338–45. [PubMed] [Google Scholar]
- 5.West CP, Huschka MM, Novotny PJ, Sloan JA, Kolars JC, Habermann TM, Shanafelt TD. Association of perceived medical errors with resident distress and empathy: a prospective longitudinal study. JAMA. 2006;296:1071–8. doi: 10.1001/jama.296.9.1071. [DOI] [PubMed] [Google Scholar]
- 6.Lu DW, Dresden S, McCloskey C, Branzetti J, Gisondi MA. Impact of Burnout on Self-Reported Patient Care Among Emergency Physicians. West J Emerg Med. 2015. doi:10.5811/westjem.2015.9.27945. [DOI] [PMC free article] [PubMed]
- 7.Rabatin J, Williams E, Baier Manwell L, Schwartz MD, Brown RL, Linzer M. Predictors and Outcomes of Burnout in Primary Care Physicians. J Prim Care Community Health. 2015. doi:10.1177/2150131915607799. [DOI] [PMC free article] [PubMed]
- 8.Fuyuno I. Numbers of young scientists declining in Japan -Government policies are hampering the country’s next generation of research leaders, advisory body says. 2012. http://www.nature.com/news/numbers-of-young-scientists-declining-in-japan-1.10254. Accessed 27 Sept 2016.
- 9.Umene-Nakano W, Kato TA, Kikuchi S, Tateno M, Fujisawa D, Hoshuyama T, Nakamura J. Nationwide survey of work environment, work-life balance and burnout among psychiatrists in Japan. PLoS ONE. 2013. doi:10.1371/journal.pone.0055189. [DOI] [PMC free article] [PubMed]
- 10.Maslach C, Leiter MP, Schaufeli WB. The Oxford handbook of organizational well-being. Oxford: Oxford University Press; 2009. Measuring Burnout; pp. 86–108. [Google Scholar]
- 11.Kubo M. The factorial and construct validity of the Japanese Burnout Scale among service workers. Shinrigaku Kenkyu. 2014;85:364–72. doi: 10.4992/jjpsy.85.13214. [DOI] [PubMed] [Google Scholar]
- 12.Sarason, IG, Levine HM, Basham, RB, Sarason BR. Social Support QUESTIONNAIRE. 1983. http://wikieducator.org/images/1/14/Sarason-83-SSQ1.pdf. Accessed 11 Oct 2016.
- 13.Petek D, Gajsek T, Petek Ster M. Work-family balance by women GP specialist trainees in Slovenia: a qualitative study. BMC Med Educ. 2016;16:31. doi: 10.1186/s12909-016-0551-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sarason IG, Sarason BR. Concomitants of social support: attitudes, personality characteristics, and life experiences. J Pers. 1982;50:331–44. doi: 10.1111/j.1467-6494.1982.tb00754.x. [DOI] [PubMed] [Google Scholar]
- 15.Clara IP, Cox BJ, Enns MW, Murray LT, Torgrudc LJ. Confirmatory factor analysis of the multidimensional scale of perceived social support in clinically distressed and student samples. J Pers Assess. 2003;81:265–70. doi: 10.1207/S15327752JPA8103_09. [DOI] [PubMed] [Google Scholar]
- 16.Chatani Y, Nomura K, Ishiguro A, Jagsi R. Factors Associated With Attainment of Specialty Board Qualifications and Doctor of Medical Science Degrees Among Japanese Female Doctors. Acad Med. 2016. doi:10.1097/ACM.0000000000001260. [DOI] [PubMed]
- 17.Nomura K, Yamazaki Y, Gruppen LD, Horie S, Takeuchi M, Illing J. The difficulty of professional continuation among female doctors in Japan: a qualitative study of alumnae of 13 medical schools in Japan. BMJ Open. 2015. doi:10.1136/bmjopen-2014-005845. [DOI] [PMC free article] [PubMed]
- 18.Fortney L, Luchterhand C, Zakletskaia L, Zgierska A, Rakel D. Abbreviated mindfulness intervention for job satisfaction, quality of life, and compassion in primary care clinicians: a pilot study. Ann Fam Med. 2013;11:412–20. doi: 10.1370/afm.1511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Equal Employment and Child Welfare, Annual Health, Labour, and Welfare Report p.179. Ministry of,Health, Labor and Welfare. 2015. http://www.mhlw.go.jp/english/wp/wp-hw9/dl/07e.pdf. Accessed 25 Mar 2017.
- 20.Johansson M, Thomas J, Hildingsson I, Haines H. Swedish fathers contemplate the difficulties they face in parenthood. Sex Reprod Healthc. 2016;8:55–62. doi: 10.1016/j.srhc.2016.02.005. [DOI] [PubMed] [Google Scholar]
- 21.Awareness survey about balancing work and life “Shigoto to Seikatsu no Chowa ni Kansuru Ishikichosa”. Cabinet Office of Japanese Garvernment. 2012. http://wwwa.cao.go.jp/wlb/research/pdf/wlb-net-svy.pdf. Accessed 27 Sept 2016.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets generated and/or analysed during the current study are not publicly available due to including the privacy of participants but are available from the corresponding author on reasonable request.