

Abstract
Purpose
To determine whether knee extensor power asymmetry limits functional mobility of older adults who possess muscle weakness.
Methods
Knee extensor power was measured in 36 older men and women (76.0 ± 7.6 yr), for each leg, on an isokinetic dynamometer at 60, 180, and 300 deg s−1 and power asymmetry was calculated as the percent difference in power between strong and weak legs, at each isokinetic velocity. 400-m walk, stair ascent, and five-repetition chair rise tests were performed to assess functional mobility. Pearson correlations were used to examine the relationship between weak leg power, strong leg power, power asymmetry, and 400-m walk time, stair ascent time, and chair rise time. Participants were then stratified into Low Power-High Asymmetry (LP-HA), Low Power-Low Asymmetry (LP-LA), High Power-High Asymmetry (HP-HA), and High Power-Low Asymmetry (HP-LA) groups who were compared for functional mobility.
Results
Knee extensor power asymmetry was unrelated to 400-m walk time (r = 0.16, p = 0.180), stair ascent time (r = 0.22, p = 0.094), or chair rise time (r = 0.03, p = 0.437), whereas weak and strong leg powers were equally associated with 400-m time (r = −0.62, p < 0.001; r = −0.62, p < 0.001), stair ascent time (r = −0.55, p < 0.001; r = −0.57, p < 0.001), and chair rise time (r = −0.28, p = 0.048; r = −0.31, p = 0.032), respectively. Power asymmetry was lowest at 60 deg s−1 (12%), and increased with contraction velocity (p = 0.001) to 15% at 180 deg s−1 and to 20% at 300 deg s−1. LP-HA exhibited 26% slower 400-walk time than HP-LA (p = 0.015) and 19% slower than HP-HA (p = 0.037). LP-HA had 31% slower stair ascent time than HP-LA (p = 0.033). There were no differences in chair rise performance between groups.
Conclusions
Knee extensor power asymmetry was unrelated to 400-m walk, stair ascent, and chair rise performance in older adults. Weak and strong limb powers were equally related to these functional measures, but a leftward shift of the power-mobility curve exists for the weak leg that may hinder clinical assessment if strength or power is measured on a single limb and symmetry is assumed. The greatest degree of knee extensor power asymmetry occurred at the fastest isokinetic velocity, which suggests high-speed muscle contractions may better differentiate laterality of function in older individuals.
Keywords: Lower-extremity function, strength, imbalance, symmetry, aging, laterality of function
1. Introduction
In older adults, low leg strength and power are important risk factors for falls, mobility limitations and disabilities, loss of independence, and hospital admissions (Wolfson, Judge et al. 1995, Skelton, Kennedy et al. 2002, Bean, Leveille et al. 2003, Manini, Visser et al. 2007, Cawthon, Fox et al. 2009). In both research and clinical settings, lower-extremity strength and power are sometimes measured bilaterally (i.e. both legs at the same time), or unilaterally on a single limb, with the assumption that limbs have equivalent function. However, differences in strength and power exist between limbs as a result of limb dominance, previous injury, disease, disuse, or occupation, which may hinder clinical interpretation of strength and power scores if symmetry is assumed (Manini, Visser et al. 2007, Suetta, Aagaard et al. 2007, Lanshammar and Ribom 2011, Alcock, O’Brien et al. 2014). The asymmetry of strength and power are approximately 10% for healthy, young adults, but increase to 15% in older adults, and 20% or more in older fallers, yet it is unclear how asymmetry impacts functional mobility in older adults (Skelton, Kennedy et al. 2002, Perry, Carville et al. 2007).
Recent work in our laboratory identified that older individuals with 20% or greater isometric knee extensor strength asymmetry had a more asymmetrical and variable gait pattern, and walked 19% slower than their more symmetrical peers (LaRoche, Cook et al. 2012). This study led to the hypothesis that strength asymmetry may be associated with physical dysfunction in older adults and that the weaker limb may limit walking performance. Using a pneumatic resistance knee extension, Carabello and colleagues demonstrated that older, mobility-limited participants had greater power asymmetry (≈20%) than healthy, older adults (≈12%), but did not observe any correlation between the degree of asymmetry and physical function (Carabello, Reid et al. 2010). Using the Nottingham power rig, Portegijs et al. showed in older women that maximal walking velocity was slowest in those that demonstrated poor leg extensor power and high asymmetry and that each variable was an independent predictor of walking velocity (Portegijs, Sipila et al. 2005). When leg press strength was assessed using pneumatic resistance, Ward and colleagues showed that despite their older adult sample possessing 20% strength asymmetry, a larger magnitude of asymmetry was not a predictor of decline in self-reported lower-extremity function, whereas weaker leg strength was (Ward, Beauchamp et al. 2016).
Despite the greater degree of power asymmetry in older adults, there has been only limited investigation of its relationship to functional performance in this at-risk population. It is currently undetermined whether strength and power asymmetry affect functional mobility in older adults, or if the independent powers of the strong or weak limbs are more associated with function. While greater strength and power asymmetry have been previously linked to slower walking velocity, less is known about the relation of asymmetry to other functional movements like chair rise and stair ascent. It is well-known that lower-extremity isokinetic power changes across muscle contraction velocities (Lanza, Towse et al. 2003), yet it is unknown how velocity affects muscle power asymmetry. Clarifying the connection between strong and weak leg powers, power asymmetry and functional mobility is important for understanding factors that limit movement in older adults and for valid assessment of their lower-extremity capacity.
The first purpose of this study was to determine if isokinetic knee extensor power asymmetry, obtained from a range of muscle contraction velocities, was related to 400-m walk, stair ascent, and chair rise performance in older adults at risk of mobility limitations due to low strength. It was hypothesized that there would be a linear relationship between the magnitude of knee extensor power asymmetry and 400-m walk, stair ascent, and chair rise times, that is, older adults with greater asymmetry would perform these activities more slowly. The second purpose was to determine if either strong or weak leg power was more closely associated with functional mobility; particularly to explore the hypothesis that weak limb power is the major limiter of performance in older adults. The third purpose was to explore the combined effects of power and asymmetry on physical function. It was hypothesized that when older adults were separated into Low Power-High Asymmetry (LP-HA), Low Power-Low Asymmetry (LP-LA), High Power-High Asymmetry (HP-HA), and High Power-Low Asymmetry (HP-LA) groups, that LP-HA would exhibit the lowest level of functional mobility and HP-LA the highest.
2. Methods
2.1 Participants
Thirty-six, community dwelling older men and women were recruited to the study via targeted mailings. To be included participants had to have a BMI < 30 kg m−2, have knee extensor muscle weakness placing them at risk of mobility limitation (as described below), and not have major cardiovascular, orthopedic, neuromuscular, or other health conditions that would affect their safe participation in the study. The study was approved by the University of New Hampshire Institutional Review Board for the use of human subjects and all participants gave their written, informed consent.
2.1 Visit 1 – Strength Screening
Upon arrival to the laboratory, participants’ height and mass were recorded and they were positioned on an isokinetic dynamometer (HUMAC NORM, CSMI, Stoughton, MA, USA) with a trunk angle of 100 deg and initial knee angle of 90 deg. They then performed three maximal, voluntary knee extensions, through a 90-deg range of motion, at an angular velocity of 60 deg s−1 using the right leg according to the protocol of Manini et al. (2007). Women were identified as having muscle weakness if the average of the three strength scores was less than 1.34 Nm kg−1 and men were identified as having muscle weakness if the average score was less than 1.71 Nm kg−1 using established criteria (Manini, Visser et al. 2007). Those who qualified for the study returned for a second visit to complete the 400-m long-distance corridor walk, chair rise, and stair ascent tests, and a knee extensor power familiarization session.
2.2 Visit 2 – Functional Mobility Assessment
At visit 2, participants performed a timed five-repetition chair rise test, with arms folded across the chest, that required them to stand up and sit down from a chair with a seat pan height of 0.44 m as fast as possible. They completed a timed stair ascent test that required them to climb a flight of 13 stairs with a tread height of 0.19 m as fast as possible using the hand rail only if needed. Chair rise and stair ascent times were recorded to the nearest tenth of a second. Participants performed the 400-m walk around two cones placed 20 m apart in accordance with established long-distance corridor walk methodology (Simonsick, Montgomery et al. 2001, Rolland, Cesari et al. 2004). Participants were instructed to “walk 10 laps, as quickly as possible, at a pace you can maintain” and the time to complete the walk was recorded to the nearest second. After participants had completely recovered from the 400-m walk, they were familiarized to knee extensor power testing on the same dynamometer used to screen for low strength. Three, maximal isokinetic knee extensions were performed at 60, 180, and 300 deg s−1 angular velocities for each leg.
2.3 Visit 3 – Power Measurement
At a third visit, 3–7 days later, participants completed knee extension power testing in the same manner as they did during the familiarization session at the three isokinetic velocities. Prior to measuring power, the dynamometer’s torque and position sensors were calibrated. To calculate knee extension power, the dynamometer’s torque and angular velocity analog outputs were sampled by a data acquisition system (MP150, BIOPAC Inc, Goleta, CA, USA) at a rate of 1 kHz and data were smoothed using a 100-sample sliding window. Knee extensor power (Watts) was calculated by the data acquisition software (AcqKnowledge, BIOPAC Inc, Goleta, CA, USA), in real time, as the product of the torque (Nm) and angular velocity (rad s−1) channels. The first of the three contractions refamiliarized the participants to the task, and the second two power scores were normalized to body mass and averaged for analysis. The weak leg was identified as the one that had the lowest average power and the strong leg the highest average power. Asymmetry of muscle power was determined as the percent difference between strong and weak legs as done previously (Carabello, Reid et al. 2010, LaRoche, Cook et al. 2012). It should be noted that due to the constant velocity of isokinetic contractions, that the asymmetries derived from peak torque (strength) and peak power are identical.
2.4 Statistical Analysis
Participant characteristics were compared between groups using one-way analysis of variance or chi square (χ2) tests as appropriate. To evaluate the consistency of power from trial-to-trial, and the consistency and direction (i.e. right vs. left) of power asymmetry across isokinetic contraction velocities, intraclass correlation coefficients were determined using Chronbach’s alpha. Then the standard error of the measurements (SEM) were calculated at each velocity. To test the first hypothesis of the study, Pearson correlations were used to relate the degree of power asymmetry at 60 deg s−1, 180 deg s−1, and 300 deg s−1 to 400-m walk, stair ascent, and chair rise times. To test the second hypothesis, knee extensor powers of strong and weak limbs were each associated with mobility tests in separate correlations to identify whether strong or weak leg power was more closely associated with lower-extremity function. Multiple regression was not used for these associations due to the high degree of dependency among predictor variables.
To test the third hypothesis, a 2 × 2 (power group × asymmetry group) multivariate analysis of variance (MANOVA) was used to compare 400-m walk time, stair ascent time, and chair rise time between LP-HA (n=9), LP-LA (n=9), HP-HA (n=9), and HP-LA (n=9) subgroupings. The groups were established by dichotomizing participants using the median power (1.81 W kg−1) as the threshold for low and high power group membership and the median power asymmetry (15.05 %) as the threshold for low and high asymmetry group membership. The medians were obtained from participants’ average power and average asymmetry calculated across the three isokinetic test velocities. The authors recognize that the sample size is marginal for this analysis and using the median to dichotomize participants may reduce effect sizes and statistical power, and increase the risk for Type II error (Cohen 1983, Iacobucci, Posavac et al. 2015), hence we consider this analysis exploratory. Because groups differed by gender and mass these variables were then tested as covariates. Further, repeated measures analysis of variance was used to determine if weak leg power, strong leg power, and power asymmetry varied across isokinetic test velocities and whether this differed between low and high asymmetry groups. Post hoc dependent and independent T-tests were used as appropriate to test for contraction velocity and group differences when main effects or interactions existed. Statistical significance was set at p < 0.05 for all tests. All analyses were conducted using a statistical program (IBM SPSS Statistics, v. 23, Chicago, IL).
3. Results
3.1 Participant Characteristics
Participant descriptive characteristics are reported in Table 1 for the overall sample, and when the same participants were dichotomized into low and high power, and, low and high asymmetry groupings. Age and BMI were similar within asymmetry and power groupings. Gender was unevenly distributed among low power and high power groups (χ2 = 13.8, p < 0.001) but was more evenly distributed among low asymmetry and high asymmetry groups (χ2 = 1.0, p = 0.310). Height and mass were greater in the high power than low power group (p < 0.05), but did not differ between low and high asymmetry groups. Table 2. provides participant characteristics for the LP-HA, LP-LA, HP-HA, and HP-LA subgroups that resulted from the 2 × 2 MANOVA. Gender was unequally distributed among the groups (χ2 = 15.0, p = 0.002) and mass was lower in LP-LA than HP-LA (p = 0.039).
Table 1.
Participant descriptive characteristics for the overall sample, and when the same participants were dichotomized into Low and High Power, and, Low and High Asymmetry groupings.
| Overall | Low Power | High Power | Low Asymmetry | High Asymmetry | |
|---|---|---|---|---|---|
| Age (yr) | 76.0 ± 7.6 | 77.7 ± 7.1 | 74.3 ± 7.9 | 75.1 ± 6.9 | 76.9 ± 8.3 |
| Males/Females (n) | 15/21 | 2/16a | 13/5 | 6/12 | 9/9 |
| Mass (kg) | 74.3 ± 13.2 | 68.0 ± 11.0b | 80.6 ± 12.4 | 73.3 ± 15.1 | 75.3 ± 11.3 |
| Height (m) | 1.67 ± 0.09 | 1.63 ± 0.06b | 1.71 ± 0.10 | 1.66 ± 0.10 | 1.67 ± 0.09 |
| Body Mass Index (kg m−2) | 26.6 ± 3.3 | 25.7 ± 4.0 | 27.6 ± 2.3 | 26.3 ± 4.0 | 26.9 ± 2.7 |
Values are mean ± SD
unequal distribution (X2) between Low and High Power groups, p < 0.05
difference between Low and High Power groups, p < 0.05
Table 2.
Participant descriptive characteristics for subgroups of the 2 × 2 (power group × asymmetry group) Multivariate Analysis of Variance.
| LP-HA | LP-LA | HP-HA | HP-LA | |
|---|---|---|---|---|
| Age (yr) | 77.9 ± 8.2 | 77.4 ± 6.3 | 75.9 ± 8.8 | 72.7 ± 7.0 |
| Males/Females (n)a | 2/7 | 0/9 | 7/2 | 6/3 |
| Mass (kg) | 70.6 ± 8.9 | 65.4 ± 12.6b | 79.9 ± 11.9 | 81.2 ± 13.6 |
| Height (m) | 1.64 ± 0.07 | 1.62 ± 0.05 | 1.70 ± 0.10 | 1.71 ± 0.10 |
| Body Mass Index (kg m−2) | 26.2 ± 2.8 | 25.2 ± 5.0 | 27.7 ± 2.4 | 27.5 ± 2.3 |
Values are mean ± SD
LP-HA = Low Power – High Asymmetry
LP-LA = Low Power – Low Asymmetry
HP-HA = High Power – High Asymmetry
HP-LA = High Power – Low Asymmetry
unequal distribution (X2) among groups, p < 0.05
difference between LP-LA and HP-LA groups, p < 0.05
3.2 Power Asymmetry and Contraction Velocity
The trial-to-trial (contraction 2 - contraction 3) intraclass correlation coefficient for knee extensor power was rxx = 0.99 (95% confidence interval 0.98 – 0.99) at each isokinetic velocity. The SEMs for power at 60 deg s−1, 180 deg s−1, and 300 deg s−1 were ±3.3 W, ±7.2 W, and ±8.3 W respectively, or 0.04 W kg−1, 0.10 W kg−1, and 0.11 W kg−1. The intraclass correlation coefficient for power asymmetry consistency across 60 deg s−1, 180 deg s−1, and 300 deg s−1, that considered both the laterality and magnitude of power asymmetry, was rxx = 0.81 (95% confidence interval 0.66 – 0.90). The SEMs for power asymmetry at 60 deg s−1, 180 deg s−1, and 300 deg s−1 were ±6.7%, ±10.2%, and ±12.4% respectively. Within individuals, strong and weak leg knee extensor powers were closely related to each other (r = 0.91, p < 0.001) despite the presence of a 16 ± 10 % average power asymmetry across all participants and contraction velocities (range of 3 – 35%).
For weak leg power, there was a significant effect of velocity (p < 0.001) because power increased from 60 deg s−1 by 62% at 180 deg s−1 and 75% at 300 deg s−1 (Figure 1A). An asymmetry group by velocity interaction (p = 0.003) indicates that weak leg power increased more in LA than it did in HA resulting in increasingly larger deficits in weak leg power for HA as contraction velocity increased. There was also a significant effect of velocity for strong leg power (p < 0.001) as power increased by 93% at 180 deg s−1 and 88% at 300 deg s−1 (Figure 1B), but no group effects or interactions existed. There was a significant effect of velocity (p = 0.001) on knee extensor power asymmetry as average asymmetry was lowest at 60 deg s−1 (12±8%), but increased linearly to 15±13% at 180 deg s−1 and to 20±15 % at 300 deg s−1 (Figure 1C). A significant asymmetry group by velocity interaction (p = 0.002) demonstrates that LA maintained a consistent level of power asymmetry across velocities whereas HA experienced a doubling of power asymmetry from 60 to 300 deg s−1.
Figure 1.
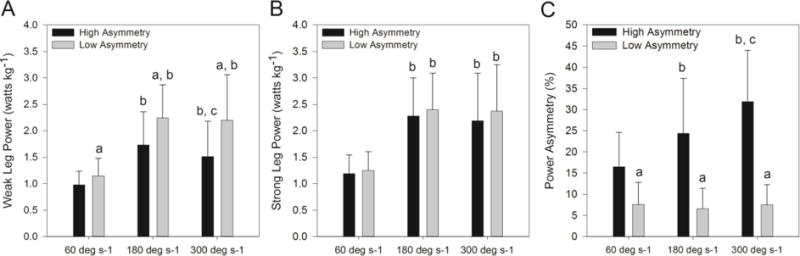
Comparison of weak leg knee extensor power (A), strong leg knee extensor power (B), and power asymmetry (C) between older adults with symmetrical (≤ 15%) and asymmetrical (> 15%) knee extensor power across a range of isokinetic contraction velocities.
a = different between asymmetrical and symmetrical groups, p < 0.05
b = different from 60 deg s−1 isokinetic test velocity, p < 0.05
c = different from 180 deg s−1 isokinetic test velocity, p < 0.05
3.3 Power, Asymmetry and Functional Mobility
Percent knee extensor power asymmetry was not associated with 400-m walk time, stair ascent time, or chair rise time for any isokinetic test velocity (Figure 2 A, B, C). Knee extensor powers of the strong and weak limbs, were both moderately related to 400-m walk time (Figure 2D) and stair ascent time (Figure 2E), but were only weakly related to chair rise time (Figure 2F). For simplicity, Figure 2 only displays data obtained at 180 deg s−1 as the relationships between strong and weak leg powers and functional mobility scores were similar at 60 deg s−1 (r = −0.36 to −0.54, p = 0.019 to p < 0.001) and 300 deg s−1 (r = −0.21 to −0.62, p = 0.117 to p < 0.001).
Figure 2.
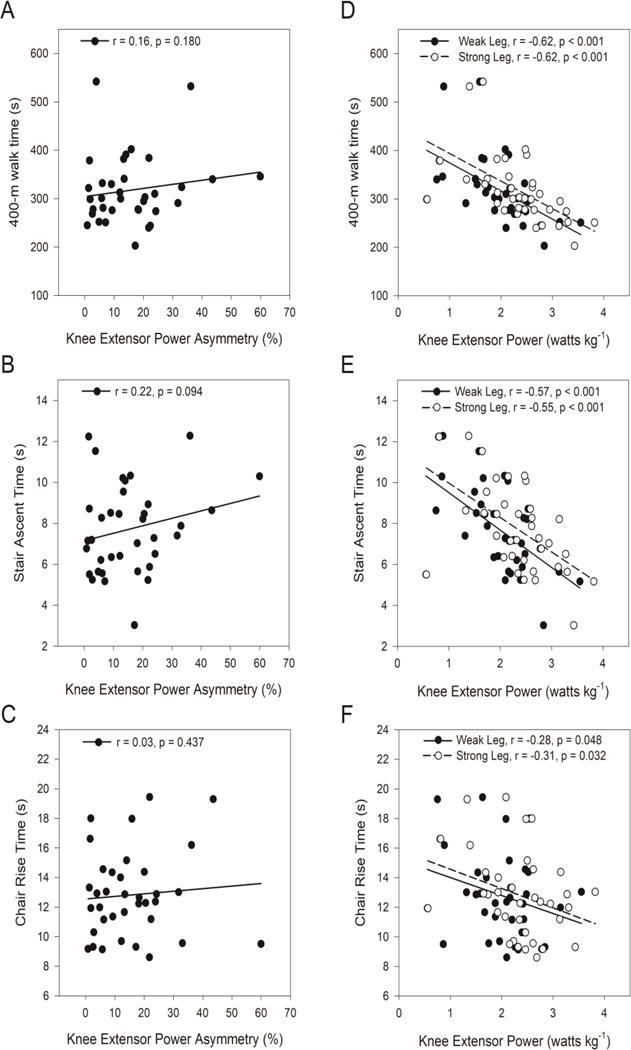
Associations between isokinetic knee extensor power asymmetry obtained at 180 deg s−1 and 400-m walk time (A), stair ascent time (B), and chair rise time (C), and, between isokinetic knee extensor power of strong and weak legs obtained at 180 deg s−1 and 400-m walk time (D), stair ascent time (E), and chair rise time (F).
When participants were separated into LP-HA, LP-LA, HP-HA, and HP-LA subgroups and compared for functional mobility performance, there was a significant main effect of power group for 400-m walk time (p = 0.014), yet no effect of asymmetry group (p = 0.32 – 0.47), nor power by asymmetry group interactions (p = 0.46 – 0.99) for any of the mobility measures (Figure 3). When gender was tested as a covariate it was not significant in the model (p = 0.92) and did not affect any main effects or interactions. Because mass was greater in the high-power group it was tested as a covariate. While it did not achieve statistical significance in the model (p = 0.073), its inclusion elicited a significant main effect of power group for stair ascent time (p = 0.013). Post hoc tests revealed that LP-HA’s 400-m walk time was 26% slower than HP-LA (p = 0.015) and 19% slower than HP-HA (p = 0.037) (Figure 3A). Similarly, LP-LA walked 21% slower than HP-LA (p = 0.044). LP-HA had 31% slower stair ascent time than HP-LA (p = 0.033) (Figure 3B). There were no group differences for chair rise time (Figure 3C).
Figure 3.
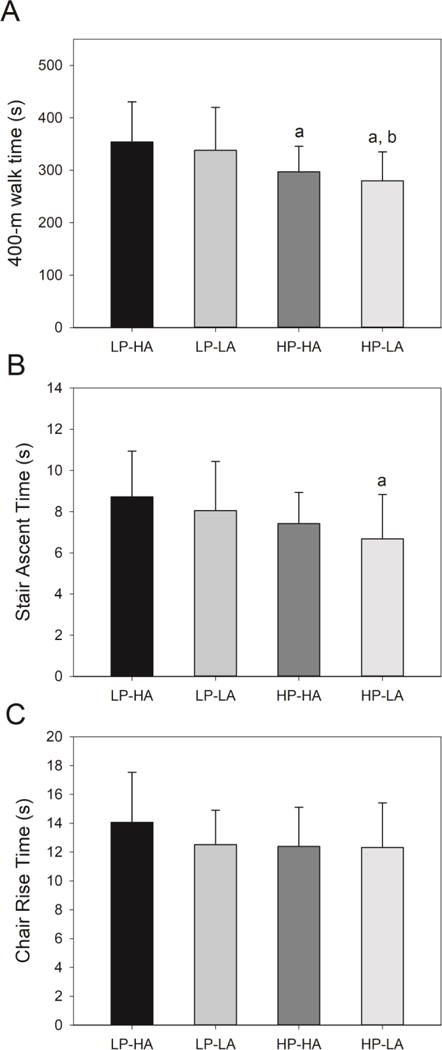
Comparison of 400-m walk time (A), stair ascent time (B), and chair rise time (C) between older adults who had low power and high asymmetry (LP-HA), low power and low asymmetry (LP-LA), high power and high asymmetry (HP-HA), and high power and low asymmetry (HP-LA). Low and high power groups were established using a 1.81 W kg−1 threshold and low and high asymmetry groups using a 15% threshold.
a = different from LP-HA, p < 0.05
b = different from LP-LA, p < 0.05
4. Discussion
This study tested the hypothesis that lower-extremity power asymmetry is related to functional mobility in older adults and the hypothesis that the weak limb is the major limiter of lower-extremity function in this group. Neither hypothesis was supported as knee extensor power asymmetry was unrelated to 400-m walk, stair ascent, or chair rise performance, and strong and weak limb powers were equally related to performance of these functional tasks.
These data indicate that the independent power of limbs is more closely related to function than the symmetry of power between limbs, which is in agreement with previous work by Carabello et al. (2010). The Boston RISE study found that while leg strength asymmetry was a significant predictor of self-reported lower-extremity function in older adults, it had the lowest association of the neuromuscular predictor variables, particularly in comparison to leg strength (Bean, Latham et al. 2013). Similarly, Straight and colleagues (2016) demonstrated that leg extension power asymmetry was weakly correlated to 6-minute walk, timed up-and-go, and 30-s chair stand tests and was an independent predictor of overall lower-extremity function only after controlling for total leg power, age, comorbidities, physical activity and adiposity. Longitudinal data from the Boston RISE study demonstrated that weaker leg strength was associated with a nearly two-fold likelihood of declining lower-extremity function, yet strength asymmetry was not (Ward, Beauchamp et al. 2016). Taken together, these results suggest that the asymmetry of strength and power is only marginally related to the functional mobility of older adults.
Asymmetries may develop because of unequal mechanical stimuli due to preferential use of one limb over another, disuse, injury or disease that affects one side of the body (e.g. arthritis, stroke, peripheral neuropathy) (Suetta, Aagaard et al. 2007, Lanshammar and Ribom 2011). For instance Alcock et al. (2014) demonstrated that older women who consistently used one limb to initiate stair ascent, more frequently stepped first with the weaker limb and used the stronger limb to transition from the ground to the second step, a movement that requires a greater vertical displacement. Despite an average 16% asymmetry in this sample, strong and weak leg powers were closely related to each other (r = 0.91), likely, because once initiated, many functional activities require the two limbs to work in unison. Thus, the mechanical loading and muscular forces experienced by an individual as a result of regular physical activity would be similar between limbs and neuromuscular adaptations that occur in response to these activities might be expected to be comparable. A physically active person may still have asymmetry, but have greater strength and power in both strong and weak limbs than a less active person. For instance, in this study HP-HA performed the 400-m walk faster than LP-HA despite a similar level of power asymmetry. The result is that the slope of the power and functional mobility performance curve is nearly identical for strong and weak limbs, yet there is a leftward shift of the curve when comparing the regression line of the weak limb to the strong limb in Figure 2 D, E, F. In one sense this finding is advantageous for the clinician or researcher that measures strength and power bilaterally, or on a single limb, because the capacity of each limb tracks similarly with functional mobility. In contrast, the leftward shift of the power-performance curve in the weak limb decreases the x and y-intercepts, which could hinder clinical interpretation when evaluating strength or power obtained from one limb to established criteria. For example, the data from Figure 2D show that the difference between 400-m walking speeds predicted from weak and strong limbs is approximately 0.1 m s−1, which has been determined to be a clinically meaningful difference (Perera, Mody et al. 2006).
To further investigate how knee extensor power and power asymmetry interact to affect functional mobility, participants were dichotomized into low and high power groupings and low and high asymmetry groupings in an exploratory analysis. We hypothesized that the lowest level of performance would be seen in LP-HA and highest in HP-LA, which was partially supported by the data. There was no effect of asymmetry group membership on 400-m walk, stair ascent, or chair rise times, nor differences in performance between LP-HA and LP-LA, nor between HP-HA and HP-LA. These findings suggest that power asymmetry has a limited effect on mobility at either low or high power and corroborates the correlations as only power group membership was significantly associated with 400-m walk and stair ascent times. Even though gender was an insignificant covariate, the unequal distribution between power groups cannot be ignored. This may be perceived as a limitation of performing this analysis on a small sample, or alternatively, as an accurate representation of the gender differences in lower-extremity function. Nevertheless, the largest differences in 400-m walk and stair ascent times were seen between LP-HA and HP-LA groups indicating that the best performers were both powerful and symmetrical, a result comparable to Portegijs et al. (2005).
For asymmetry to be detrimental to performance, it is probable that weak limb power must be below or near the minimum power necessary for a task. Samuel and colleagues have studied functional demand, or the percent of maximal strength or power required of a joint during functional activities, and have shown that older adults require 70–120% of maximal isometric knee extensor strength during walking, chair rise, stair ascent and descent (Samuel, Rowe et al. 2013). This demand may be overestimated in some instances (i.e. exceeding 100%) because the dynamic contractions that contribute to the knee extensor moment during ambulation were compared to isolated isometric strength measures. Regardless, if weak limb capacity is greater than required of the task, or if proximal or distal joints compensate for weakness, movement may be unimpeded and symmetrical, even in the presence of large strength and power asymmetries (Winter 1980). In this instance, symmetrical lower extremity forces may be generated by differential nervous activation, for example by increasing agonist activation of the weak limb or increasing antagonist activation of the strong limb (Õunpuu and Winter 1989, Bond, Cook et al. 2017). The ability to compensate for strength and power asymmetry may partially explain the lack of relation between measurements of asymmetry and functional mobility, but the extent to which this occurs in older adults is unknown. It is possible that older individuals have a reduced compensatory ability as a high-degree of strength asymmetry has been related to greater gait asymmetry in older walkers (LaRoche, Cook et al. 2012).
A novel finding of this study was that knee extensor power asymmetry increased with isokinetic contraction velocity. This effect was driven by an attenuated increase in weak leg power at 180 deg s−1, and a reduction in weak leg power at 300 deg s−1 in the HA group as strong leg powers increased proportionally and were comparable between LA and HA groups. Consequently, the greatest difference in power between these groups occurred in the weak leg at the fastest velocity, resulting in a doubling of power asymmetry from 60 deg s−1 to 300 deg s−1 in HA. This suggests that power asymmetry may be manifested most notably at fast contraction velocities, possibly due to the greater demand for motor unit activation, recruitment of type II muscle fibers, and limitations in nerve conduction velocity, excitation-contraction coupling, and contractile function (Komi, Linnamo et al. 2000, Babault, Pousson et al. 2002). These findings have important implications for fall risk as it has been demonstrated that step velocity and rate of weight transfer after perturbation are predictors of ability to recover from a fall (Thelen, Wojcik et al. 1997, Wojcik, Thelen et al. 1999). Skelton et al. (2002) showed that older fallers had 24% less leg extensor power in the weak limb and exhibited nearly three times the power asymmetry of nonfallers. It is interesting to contemplate that the rate of balance recovery might differ in those with high power asymmetry depending on which limb supports and which steps in response to a perturbation, but this remains to be investigated. Further, knee angular velocities in the 180 to 300 deg s−1 range are close to those observed during chair rise and walking, and power obtained at these speeds may have greater external validity (Jevsevar, Riley et al. 1993). Thus, it is our recommendation that strength and power testing of older adults include high-velocity assessments and exercise interventions incorporate high-velocity exercise training that has been shown to confer functional benefits to both healthy and diseased older adults (Ni, Signorile et al. 2016, Sayers, Gibson et al. 2016).
In population-based studies and screening programs strength and power are often measured on a single limb (e.g. dominant or right limb), or using bilateral exercises like the leg press, in order to minimize assessment time. While convenient, this streamlined method is insensitive to differences in strength and power that occur between legs, and may miss significant, unilateral, lower-extremity weakness. The problem is complicated by the fact that the dominant limb is not always the stronger limb and asymmetry of strength and power may be joint and task-specific. (Vagenas and Hoshizaki 1991, Sadeghi, Allard et al. 2000). If symmetry is assumed in older adults, failure to account for the side-to-side differences in strength and power may lead to the misclassification of risk for mobility limitations, falls, and other adverse health events. The difference in peak knee extensor torque between strong and weak limbs at 60 deg s−1 in this study was 0.15 Nm kg−1, which introduces an approximate 10% error when comparing these scores to knee extensor strength cutpoints developed to identify risk of mobility limitations (1.34 Nm kg−1 for women, 1.71 Nm kg−1 for men) (Manini, Visser et al. 2007). Further, identification of strong and weak limbs may allow practitioners to counsel patients regarding optimal strategies for transfers, initiating gait, stair ascent and descent to reduce the risk of falls. It is therefore important that future investigations relating strength and power to the health and mobility of older adults measure the performance of each limb independently to more carefully characterize the relationship between lower-extremity capacity and function.
When testing older adults for lower extremity strength, power, and asymmetry, it should be considered that strong to weak leg differences may be task-specific and vary across load and contraction velocity. Power asymmetry demonstrated good consistency across contraction velocities (rxx = 0.81), but consistency was lower than that of power measurement (rxx = 0.99) partially because error is compounded when two legs that each have their own power variability are used in the calculation of asymmetry. The SEMs from this study suggest that ≥10% power asymmetry may be detectable using isokinetic dynamometry, but asymmetry <10% may not be differentiated from the inherent variability of asymmetry measurement. It’s also probable that power asymmetry may not be an intrinsic characteristic of muscles, but rather a complex phenomenon resulting from the interaction of anatomical and physiological differences between limbs, laterality of function of the central nervous system, and efficacy of compensatory strategies (Sadeghi, Allard et al. 2000).
It should be noted that previous investigations of strength and power asymmetry in older adults have used a range of testing modalities including pneumatic resistance, the Nottingham Power Rig, and isokinetic dynamometry, and, some studies measured knee extensor asymmetry whereas others measured whole-leg asymmetry (Skelton, Kennedy et al. 2002, Portegijs, Sipila et al. 2005, Perry, Carville et al. 2007, Carabello, Reid et al. 2010, LaRoche, Cook et al. 2012, Bean, Latham et al. 2013, Straight, Brady et al. 2016, Ward, Beauchamp et al. 2016). These studies are therefore not directly comparable because of the task-specificity of asymmetry and the use of compensatory mechanisms that may mask single-joint strength and power asymmetries during whole-leg exercises (Bond, Cook et al. 2017). Neither the current study, nor the previous research discussed herein, has been able to directly test whether the weak limb limits functional mobility of older adults. To address this question future investigations may consider using the functional demand model (Samuel, Rowe et al. 2013), or directly compare the preferential use of strong and weak limbs (Alcock, O’Brien et al. 2014) during fall recovery, transfer, and ambulatory activities. Further, these assessments should not just be performed during short duration bouts, but should be obtained during a potentially fatiguing mobility task, such as the 400-m walk, because strong and weak leg performance may decline at different rates. Additional limitations of the current study include inclusion of only participants with low strength, exclusion of obese individuals, measurement of power only in the knee extensors, and a small sample size for the asymmetry-power subgroup comparisons.
In summary, knee extensor power asymmetry was unrelated to 400-m walk, stair ascent, and chair rise performance measures in older men and women. Weak and strong limb powers were equally related to these functional measures, but a leftward shift of the power-mobility curve exists for the weak leg that may hinder clinical assessment if strength or power is measured on a single limb and symmetry is assumed. The greatest degree of knee extensor power asymmetry occurred at the fastest isokinetic contraction velocities, which suggests rapid movements may better differentiate laterality of function in older individuals. Since the capacity to perform high-velocity lower-extremity movements has been associated with faster gait speed and better self-reported function (Sayers, Guralnik et al. 2005, Bean, Latham et al. 2013), high-velocity exercise interventions in older adults might be used to explore whether restoration of power symmetry confers functional benefits (Earles, Judge et al. 2001, Sayers 2007). The physiological origins of strength and power asymmetry, asymmetry’s relation to mobility, gait, and fall risk, and the mechanisms by which individuals compensate for asymmetry are not well characterized and deserve further investigation.
Highlights.
Association between knee extensor power asymmetry and mobility was tested
Power asymmetry was unrelated to 400-m walk, stair ascent and chair rise times
Strong and weak leg powers were equally related to mobility measures
Older adults with low power and high asymmetry had the poorest mobility
Power asymmetry increased with isokinetic test velocity
Acknowledgments
This study was supported by the National Institute on Aging of the National Institutes of Health under award number R15 AG040700-01A1 to S.B. Cook. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
The authors would like to sincerely thank the undergraduate research assistants, and participants, for their contribution to the study.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Conflicts of Interest: The authors report no conflicts of interest.
References
- Alcock L, O’Brien TD, Vanicek N. Biomechanical demands differentiate transitioning vs. continuous stair ascent gait in older women. Clin Biomech (Bristol, Avon) 2014;29(1):111–118. doi: 10.1016/j.clinbiomech.2013.10.007. [DOI] [PubMed] [Google Scholar]
- Babault N, Pousson M, Michaut A, Ballay Y, Hoecke JV. EMG activity and voluntary activation during knee-extensor concentric torque generation. Eur J Appl Physiol. 2002;86(6):541–547. doi: 10.1007/s00421-002-0579-3. [DOI] [PubMed] [Google Scholar]
- Bean JF, Latham NK, Holt N, Kurlinksi L, Ni P, Leveille S, Percac-Lima S, Jette A. Which neuromuscular attributes are most associated with mobility among older primary care patients? Arch Phys Med Rehabil. 2013;94(12):2381–2388. doi: 10.1016/j.apmr.2013.07.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bean JF, Leveille SG, Kiely DK, Bandinelli S, Guralnik JM, Ferrucci L. A comparison of leg power and leg strength within the InCHIANTI study: which influences mobility more? J Gerontol A Biol Sci Med Sci. 2003;58(8):728–733. doi: 10.1093/gerona/58.8.m728. [DOI] [PubMed] [Google Scholar]
- Bond CW, Cook SB, Swartz EE, LaRoche DP. Asymmetry of lower extremity force and muscle activation during knee extension and functional tasks. Muscle Nerve. 2017;56:495–504. doi: 10.1002/mus.25506. [DOI] [PubMed] [Google Scholar]
- Carabello RJ, Reid KF, Clark DJ, Phillips EM, Fielding RA. Lower extremity strength and power asymmetry assessment in healthy and mobility-limited populations: reliability and association with physical functioning. Aging clinical and experimental research. 2010;22(4):324–329. doi: 10.3275/6676. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cawthon PM, Fox KM, Gandra SR, Delmonico MJ, Chiou CF, Anthony MS, Sewall A, Goodpaster B, Satterfield S, Cummings SR, Harris TB. Do muscle mass, muscle density, strength, and physical function similarly influence risk of hospitalization in older adults? J Am Geriatr Soc. 2009;57(8):1411–1419. doi: 10.1111/j.1532-5415.2009.02366.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohen J. The Cost of Dichotomization. Applied Psychological Measurement. 1983;7(3):249–253. [Google Scholar]
- Earles DR, Judge JO, Gunnarsson OT. Velocity training induces power-specific adaptations in highly functioning older adults. Arch Phys Med Rehabil. 2001;82(7):872–878. doi: 10.1053/apmr.2001.23838. [DOI] [PubMed] [Google Scholar]
- Iacobucci D, Posavac SS, Kardes FR, Schneider MJ, Popovich DL. Toward a more nuanced understanding of the statistical properties of a median split. Journal of Consumer Psychology. 2015;25(4):652–665. [Google Scholar]
- Jevsevar DS, Riley PO, Hodge WA, Krebs DE. Knee kinematics and kinetics during locomotor activities of daily living in subjects with knee arthroplasty and in healthy control subjects. Phys Ther. 1993;73(4):229–239. doi: 10.1093/ptj/73.4.229. discussion 240–222. [DOI] [PubMed] [Google Scholar]
- Komi PV, Linnamo V, Silventoinen P, Sillanpaa M. Force and EMG power spectrum during eccentric and concentric actions. Med Sci Sports Exerc. 2000;32(10):1757–1762. doi: 10.1097/00005768-200010000-00015. [DOI] [PubMed] [Google Scholar]
- Lanshammar K, Ribom EL. Differences in muscle strength in dominant and non-dominant leg in females aged 20–39 years–a population-based study. Physical therapy in sport: official journal of the Association of Chartered Physiotherapists in Sports Medicine. 2011;12(2):76–79. doi: 10.1016/j.ptsp.2010.10.004. [DOI] [PubMed] [Google Scholar]
- Lanza IR, Towse TF, Caldwell GE, Wigmore DM, Kent-Braun JA. Effects of age on human muscle torque, velocity, and power in two muscle groups. J Appl Physiol. 2003;95(6):2361–2369. doi: 10.1152/japplphysiol.00724.2002. [DOI] [PubMed] [Google Scholar]
- LaRoche DP, Cook SB, Mackala K. Strength asymmetry increases gait asymmetry and variability in older women. Medicine and science in sports and exercise. 2012;44:2172–2181. doi: 10.1249/MSS.0b013e31825e1d31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Manini TM, Visser M, Won-Park S, Patel KV, Strotmeyer ES, Chen H, Goodpaster B, De Rekeneire N, Newman AB, Simonsick EM, Kritchevsky SB, Ryder K, Schwartz AV, Harris TB. Knee extension strength cutpoints for maintaining mobility. J Am Geriatr Soc. 2007;55(3):451–457. doi: 10.1111/j.1532-5415.2007.01087.x. [DOI] [PubMed] [Google Scholar]
- Ni M, Signorile JF, Balachandran A, Potiaumpai M. Power training induced change in bradykinesia and muscle power in Parkinson’s disease. Parkinsonism Relat Disord. 2016;23:37–44. doi: 10.1016/j.parkreldis.2015.11.028. [DOI] [PubMed] [Google Scholar]
- Õunpuu S, Winter DA. Bilateral electromyographical analysis of the lower limbs during walking in normal adults. Electroencephalogr Clin Neurophysiol. 1989;72(5):429–438. doi: 10.1016/0013-4694(89)90048-5. [DOI] [PubMed] [Google Scholar]
- Perera S, Mody SH, Woodman RC, Studenski SA. Meaningful change and responsiveness in common physical performance measures in older adults. J Am Geriatr Soc. 2006;54(5):743–749. doi: 10.1111/j.1532-5415.2006.00701.x. [DOI] [PubMed] [Google Scholar]
- Perry MC, Carville SF, Smith IC, Rutherford OM, Newham DJ. Strength, power output and symmetry of leg muscles: effect of age and history of falling. Eur J Appl Physiol. 2007;100(5):553–561. doi: 10.1007/s00421-006-0247-0. [DOI] [PubMed] [Google Scholar]
- Portegijs E, Sipila S, Alen M, Kaprio J, Koskenvuo M, Tiainen K, Rantanen T. Leg extension power asymmetry and mobility limitation in healthy older women. Arch Phys Med Rehabil. 2005;86(9):1838–1842. doi: 10.1016/j.apmr.2005.03.012. [DOI] [PubMed] [Google Scholar]
- Rolland YM, Cesari M, Miller ME, Penninx BW, Atkinson HH, Pahor M. Reliability of the 400-m usual-pace walk test as an assessment of mobility limitation in older adults. J Am Geriatr Soc. 2004;52(6):972–976. doi: 10.1111/j.1532-5415.2004.52267.x. [DOI] [PubMed] [Google Scholar]
- Sadeghi H, Allard P, Prince F, Labelle H. Symmetry and limb dominance in able-bodied gait: a review. Gait & posture. 2000;12(1):34–45. doi: 10.1016/s0966-6362(00)00070-9. [DOI] [PubMed] [Google Scholar]
- Samuel D, Rowe P, Nicol A. The functional demand (FD) placed on the knee and hip of older adults during everyday activities. Arch Gerontol Geriatr. 2013;57(2):192–197. doi: 10.1016/j.archger.2013.03.003. [DOI] [PubMed] [Google Scholar]
- Sayers SP. High-speed power training: a novel approach to resistance training in older men and women. A brief review and pilot study. J Strength Cond Res. 2007;21(2):518–526. doi: 10.1519/R-20546.1. [DOI] [PubMed] [Google Scholar]
- Sayers SP, Gibson K, Bryan Mann J. Improvement in functional performance with high-speed power training in older adults is optimized in those with the highest training velocity. Eur J Appl Physiol. 2016;116(11–12):2327–2336. doi: 10.1007/s00421-016-3484-x. [DOI] [PubMed] [Google Scholar]
- Sayers SP, Guralnik JM, Thombs LA, Fielding RA. Effect of leg muscle contraction velocity on functional performance in older men and women. J Am Geriatr Soc. 2005;53(3):467–471. doi: 10.1111/j.1532-5415.2005.53166.x. [DOI] [PubMed] [Google Scholar]
- Simonsick EM, Montgomery PS, Newman AB, Bauer DC, Harris T. Measuring fitness in healthy older adults: the Health ABC Long Distance Corridor Walk. Journal of the American Geriatrics Society. 2001;49(11):1544–1548. doi: 10.1046/j.1532-5415.2001.4911247.x. [DOI] [PubMed] [Google Scholar]
- Skelton DA, Kennedy J, Rutherford OM. Explosive power and asymmetry in leg muscle function in frequent fallers and non-fallers aged over 65. Age Ageing. 2002;31(2):119–125. doi: 10.1093/ageing/31.2.119. [DOI] [PubMed] [Google Scholar]
- Straight CR, Brady AO, Evans EM. Asymmetry in leg extension power impacts physical function in community-dwelling older women. Menopause. 2016;23(4):410–416. doi: 10.1097/GME.0000000000000543. [DOI] [PubMed] [Google Scholar]
- Suetta C, Aagaard P, Magnusson SP, Andersen LL, Sipila S, Rosted A, Jakobsen AK, Duus B, Kjaer M. Muscle size, neuromuscular activation, and rapid force characteristics in elderly men and women: effects of unilateral long-term disuse due to hip-osteoarthritis. Journal of applied physiology. 2007;102(3):942–948. doi: 10.1152/japplphysiol.00067.2006. [DOI] [PubMed] [Google Scholar]
- Thelen DG, Wojcik LA, Schultz AB, Ashton-Miller JA, Alexander NB. Age differences in using a rapid step to regain balance during a forward fall. J Gerontol A Biol Sci Med Sci. 1997;52(1):M8–13. doi: 10.1093/gerona/52a.1.m8. [DOI] [PubMed] [Google Scholar]
- Vagenas G, Hoshizaki B. Functional Asymmetries and Lateral Dominance in the Lower Limbs of Distance Runners. Internationl journal of sport biomechanics. 1991;7:311–329. [Google Scholar]
- Ward RE, Beauchamp MK, Latham NK, Leveille SG, Percac-Lima S, Kurlinski L, Ni P, Goldstein R, Jette AM, Bean JF. Neuromuscular Impairments Contributing to Persistently Poor and Declining Lower-Extremity Mobility Among Older Adults: New Findings Informing Geriatric Rehabilitation. Arch Phys Med Rehabil. 2016;97(8):1316–1322. doi: 10.1016/j.apmr.2016.03.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Winter DA. Overall principle of lower limb support during stance phase of gait. J Biomech. 1980;13(11):923–927. doi: 10.1016/0021-9290(80)90162-1. [DOI] [PubMed] [Google Scholar]
- Wojcik LA, Thelen DG, Schultz AB, Ashton-Miller JA, Alexander NB. Age and gender differences in single-step recovery from a forward fall. J Gerontol A Biol Sci Med Sci. 1999;54(1):M44–50. doi: 10.1093/gerona/54.1.m44. [DOI] [PubMed] [Google Scholar]
- Wolfson L, Judge J, Whipple R, King M. Strength is a major factor in balance, gait, and the occurrence of falls. J Gerontol A Biol Sci Med Sci. 1995;50 doi: 10.1093/gerona/50a.special_issue.64. Spec No: 64–67. [DOI] [PubMed] [Google Scholar]