

Abstract
Vitamin D is a cofactor responsible for autoimmune disorders. There is no agreement in the studies investigating the association between vitamin D and fibromyalgia. This study aims to combine the conflicting results of the primary studies which compared these patients with control groups regarding the serum concentration of vitamin D. This meta-analysis has been designed based on PRISMA guidelines. Relevant keywords were searched in PubMed, Science direct, Scopus, Cochrane, and Google scholar and primary studies were selected. After screening the eligible studies according to inclusion/exclusion criteria, we investigated the risk of bias in the selected studies and also the heterogeneity between the primary results using Cochrane (Q) and I-squared (I2) indices. The primary results were combined using inverse variance method and Cohen statistics as well as a random effects model. Publication bias was assessed using Egger test. Sensitivity analysis was applied to investigate the influence of each primary study on the final result of the meta-analysis. Suspected factors in the heterogeneity were assessed using meta-regression models. We entered 12 eligible studies in the meta-analysis including 851 cases compared with 862 controls. The standardized mean difference of Vitamin D between the two groups was −0.56 (95% confidence interval: −1.05, −0.08). Our meta-analysis showed that vitamin D serum levels of patients with fibromyalgia was significantly lower than that of control group.
Keywords: Eligibility determination, Fibromyalgia, Meta-analysis, Myofascial pain syndrome, Pain, Statistics, Vitamin D
INTRODUCTION
Fibromyalgia (FM) is a chronic non-articular rheumatologic disorder specified with chronic systemic musculoskeletal pains with unknown etiology, morning stiffness, fatigue, sleep disorder, multiple tender points, low pain threshold [1,2], symptoms of depression and anxiety [3,4,5] and intestinal dysmotility [4,5,6].
FMS affects 4–5 percent of the 30–60-year-old population 85–95 percent of whom are female [1,3]. The prevalence of FM in women is nine folds higher than that in men [6].
The pathogenesis of FM is still unknown [5]. However, several studies reported the effects of abnormal levels of neurotransmitters and disorders of the endocrine system [6,7,8,9,10]. In other words, the interaction between neuroendocrine, metabolic, and immunologic factors in developing FM cannot be ignored. In addition, other factors such as genetics, serotonin, melatonin, substance P, endorphin and vitamin D have been reported to be responsible for the pathophysiology of the disease [3,5].
Vitamin D is an important regulator of the immune system which acts as an active cofactor in the incidence of autoimmune disorders such as multiple sclerosis, rheumatoid arteritis, insulin dependent diabetes mellitus and irritable bowel syndrome. Vitamin D deficiency is defined as the serum level of 25 hydroxy vitamin D being lower than 20 ng/ml (50 nmol/ml) [11,12,13,14]. It seems that more than one billion people suffer from vitamin D deficiency [3]. This problem can lead to proximal muscle weakness, skeletal mineralization insufficiency, risk of falling in the elderly, and widespread body pain [3].
There is no consensus regarding the association between vitamin D and FM. Several studies have mentioned the correlation between a low concentration of vitamin D and non-specific musculoskeletal pains [3,12,13], while, some other studies reported the probable association between vitamin D deficiency and clinical manifestations of FM [1,3,4,5,14]. However, other studies, did not find any significant association between FM and vitamin D [15,16].
According to the above-mentioned discrepancies between the results of primary studies, we aimed to compare the serum levels of vitamin D between patients with FM and control groups using meta-analysis.
MATERIALS AND METHODS
This study was designed according to the PRISMA guideline [17] as well as a pre-defined protocol, however, this protocol has not been registered.
1. Inclusion criteria
All case-control studies published up to 30 August 2016 in English, carried out among women with fibromyalgia as cases compared with control groups, were entered into the meta-analysis. These studies had to report the mean and standard deviation of blood vitamin D levels in both groups.
2. Search strategy and data banks
To find required primary studies, PubMed, Science direct, Scopus, Cochrane, Ovid and Google scholar were searched from 22 September 2016 to 7 October 2016 by two independent researchers. Any disagreements were settled by a third researcher. The search was conducted without any geographical restriction using the following keywords: Fibromyalgia, FM, Chronic pain syndrome, 25-hydroxyvitamin D, 25OHD, 25-OHD, Vitamin D. Case-control.
3. Study selection
Two experts independently reviewed the studies regarding the inclusion criteria. First, all titles were reviewed and duplicates were excluded. Then, abstracts and full texts were investigated and irrelevant papers were omitted.
Kappa agreement statistics were used during the full text investigation based on the guideline suggested by Landis and Koch [18]. These statistics were categorized into slight agreement (0–0.20), fair agreement (0.21–0.40), moderate agreement (0.41–0.60), substantial agreement (0.61–0.80) and perfect agreement (more than 0.80).
4. Quality assessment
The quality of the primary studies was assessed using the Cochrane risk of bias tool [19,20] by two independent researchers and an additional investigator in the case of any conflicts. The risk of bias for each study was evaluated according to selection bias, performance bias, detection bias, attrition bias, reporting bias, and other sources of bias (e.g. bias of study design, extreme baseline imbalance).
Each of these biases were classified as high risk (score 0), low risk (score 2) and unclear risk of bias (score 1). The total risk of bias was calculated by a summation of all categories.
5. Data extraction
Two researchers extracted the required information from the selected studies including first author's name, date of publication, study design, country of the study conduction, sample size in each group, rationale of the sample size estimation, sampling design, diagnostic criteria, mean (SD) age of the participants in each group, mean (SD) of vitamin D in each group and P value for the difference of vitamin D between cases and controls. Discrepancies were investigated by a third researcher and final decisions were made.
6. Data analysis
All analyses were performed using Stata version 14 package (StataCorp, College station, TX, USA) as well as Cochrane Collaboration Review Manager Software (RevMan Version 5.3). Combining the results of primary studies was conducted based on inverse variance and Cohen statistics. The heterogeneity between the results was assessed using Cochrane (Q) and I-square indices considering P < 0.1 as the significance level.
As suggested by Higgins and Thompson [21], I-squared results were categorized into low heterogeneity (less than 26%), moderate heterogeneity (25%–75%) and high heterogeneity (more than 75%). According to the degree of heterogeneity, fixed or random effects models were applied for meta-analysis.
Point and pooled standardized mean differences (95% confidence intervals) of vitamin D levels between cases and controls were illustrated by forest plots. Any presence of publication bias was assessed using the Egger test (P value < 0.1 as significance level).
To assess the effect of each primary study on the total mean difference, sensitivity analysis was conducted. In addition, suspected factors in heterogeneity were investigated using meta-regression models.
RESULTS
Primary search showed 1579 studies (1507 records were identified through database searching and 72 records were identified through non-electronic search of the references) 921 of which were duplicate evidence and were removed. Reviewing the titles and abstracts revealed 644 irrelevant papers. Investigating the full texts of the remaining articles [1,3,5,14,16,22,23,24,25,26,27,28,29], two irrelevant papers [22,27] were also excluded. Others were quality assessed and entered into the final meta-analysis (Fig. 1). The Kappa statistics agreement between the researchers for full texts evaluation based on the inclusion criteria was 0.88 indicating perfect agreement.
Fig. 1. Flowchart of study selection.

All selected studies were case controls carried out among women and published between 2009 and 2016. Of these, 10 studies reported the matching variables (Table 1). The FMS diagnostic criteria were based on the American College of Rheumatology criteria. Mean age of participants in both groups was similar in nine studies. In the other three studies cases were significantly older than the controls.
Table 1. Charactristics of Primary Studies Included to Meta-analysis.

NS: Non-significant.
Fig. 2 and 3 represented the risk of bias in the primary studies based on the Cochrane risk of bias tool. There was high risk of selection bias in two studies, unclear risk of performance bias in two other studies, unclear risk of attrition bias in 12 studies, unclear detection bias in one study and unclear reporting bias in one study. Other sources of bias (design and extreme baseline imbalance) were observed in two studies (one study was high risk and in one study the risk was unclear).
Fig. 2. Risk of bias summary: review authors' judgements about each risk of bias item for each included study. ‘+’ denotes low risk of bias, ‘−’ represents high risk of bias and “?” indicated unclear bias.
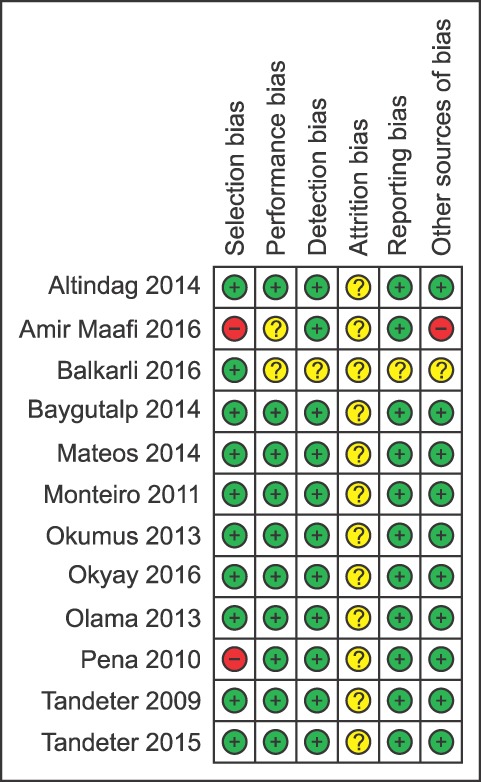
Fig. 3. Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.

All studies were carried out among 851 cases and 862 controls. In eight studies, the mean level of vitamin D was lower in cases than controls, six of which reported significant results. Of four studies reporting higher levels of vitamin D among cases, only one of the differences was statistically significant. Combining the results of these primary studies using a random effects model (Q = 244.9, P < 0.001; I-squared: 95.5%), the mean difference of vitamin D between patients and controls was estimated as −0.56 (95% confidence interval: −1.05, −0.08).
To assess the effect of the mean age of the participants as a factor for heterogeneity, meta-regression models showed non-significant results (β = 9.9, P = 0.10). We conducted a subgroup analysis based on the difference between the mean age of cases and controls and found different results between studies in which their case/control groups had the same age and those that did not (Fig. 4). In addition, another subgroup analysis was conducted based on the menopausal status of the participants which showed no difference in the pooled estimates between the premenopausal population and total population (Fig. 5).
Fig. 4. Point and pooled standardized mean difference of blood vitamin D level between subjects with and without fibromyalgia according to the age-matching of the cases/controls. In studies whose cases and controls had the same mean age, the pooled estimation of standardized mean difference of vitamin D differed between cases and controls, while in the studies which cases had different mean ages than controls, no considerable difference was observed between the vitamin D concentration of these two groups.

Fig. 5. Point and pooled standardized mean difference of blood levels of vitamin D between cases and controls based on menopausal status of cases/controls. There is no significant difference in the standardized mean difference of vitamin D between studies conducted among populations in premenopausal, postmenopausal and unknown menopausal status.

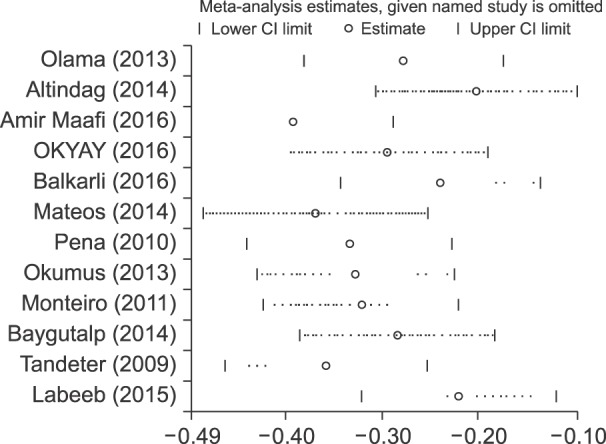
Sensitivity analysis indicated that exclusion of none of the primary studies influenced the pooled estimates (Fig. 6). Finally, the Egger test showed no evidence of publication bias (β = −17.3, P = 0.23).
Fig. 6. Sensitivity analysis of the effect of each primary study on the pooled results.
DISCUSSION
Review of the primary studies selected for meta-analysis showed that most of them found lower levels of vitamin D among FM patients than the control groups. But, four studies indicated that these patients had higher levels of vitamin D than healthy individuals. However, pooled estimates showed that FM patients in comparison with the control groups had, on average, 0.56 units lower concentration of vitamin D. Most of these studies compared age-matched cases/controls and half of these studies investigated only women in the premenopausal stage.
Vitamin D deficiency is common worldwide especially among children, women and the elderly population [3]. Half of the eight studies indicating lower concentrations of vitamin D among patients with FM had been carried out in Turkey. It seems that in such a country patients with FMS had low sunlight exposure due to their limited functional capacity.
Olama et al. [1] investigated the serum levels of vitamin D in the individuals with and without FM and found lower blood vitamin D levels in patients. They also showed that vitamin D level is correlated with pain (according to the VAS score), Beck Depression score, and lumbar bone mineral density.
Okyay et al. [3] showed severe vitamin D deficiency among patients with FMS, which was similar to our results as well as those reported by Olama et al. [1], but was in contrast to the results observed by Okumus et al. [16], which was conducted among premenopausal women.
Olama et al. [1], Okyay et al. [3], Labeeb et al. [4], Baygutalp et al. [5], Altindag et al. [14], and Okumus et al. [16] reported significant correlations between vitamin D blood level and pain intensity. In addition, significant impacts of vitamin D on the quality of life in patients with FM based on the FIQ (Fibromyalgia Impact Questionnaire) were observed by Okyay et al. [3], Labeeb et al. [4], and Altindag et al. [14], which was in contrast to the results of Baygutlap et al. [5].
The largest sample size (205 cases and controls) was used in the study conducted by Mateos et al. [25] while the Baygutalp study [5] with 19 cases/controls included the smallest sample size. Both of these studies reported lower blood vitamin D levels in FM patients than in controls.
One of the limitations of the current meta-analysis was the considerable heterogeneity between the results of the primary studies and we could not detect the source of this heterogeneity by meta-regression models. However, there were differences in the inclusion/exclusion criteria between the primary studies which might be responsible for a part of this heterogeneity. In addition, some of the studies had considered the season of the study conduction but most of them had not taken it into consideration. This might be another explanation for the observed heterogeneity.
In conclusion, our meta-analysis revealed credible evidence that vitamin D can be a determinant factor for fibromyalgia. It seems that the policymakers should consider vitamin D supplementation among women as a preventive strategy. Moreover, further studies are recommended to investigate the role of other factors such as season, obesity, menopausal status, history of hysterectomy, diabetes mellitus and other metabolic disorders, malignancy, pregnancy, sexual hormone levels, and history of OCP consumption in the heterogeneity of the primary studies.
References
- 1.Olama SM, Senna MK, Elarman MM, Elhawary G. Serum vitamin D level and bone mineral density in premenopausal Egyptian women with fibromyalgia. Rheumatol Int. 2013;33:185–192. doi: 10.1007/s00296-012-2361-0. [DOI] [PubMed] [Google Scholar]
- 2.Wolfe F, Smythe HA, Yunus MB, Bennett RM, Bombardier C, Goldenberg DL, et al. The American college of rheumatology 1990 criteria for the classification of fibromyalgia. Report of the multicenter criteria committee. Arthritis Rheum. 1990;33:160–172. doi: 10.1002/art.1780330203. [DOI] [PubMed] [Google Scholar]
- 3.Okyay R, Koçyigit B, Gürsoy S. Vitamin D levels in women with fibromyalgia and relationship between pain, tender point count and disease activity. Acta Med Mediterr. 2016;32:243–247. [Google Scholar]
- 4.Labeeb AA, Al-Sharaki DR. Detection of serum 25(OH)-vitamin D level in the serum of women with fibromyalgia syndrome and its relation to pain severity. Egypt Rheumatol Rehabil. 2015;42:196–200. [Google Scholar]
- 5.Baygutalp NK, Baygutalp F, Şeferoğlu B, Bakan E. The relation between serum vitamin D levels and clinical findings of fibromyalgia syndrome. Dicle Med J. 2014;41:446–450. [Google Scholar]
- 6.Abokrysha NT. Vitamin D deficiency in women with fibromyalgia in Saudi Arabia. Pain Med. 2012;13:452–458. doi: 10.1111/j.1526-4637.2011.01304.x. [DOI] [PubMed] [Google Scholar]
- 7.Abeles AM, Pillinger MH, Solitar BM, Abeles M. Narrative review: the pathophysiology of fibromyalgia. Ann Intern Med. 2007;146:726–734. doi: 10.7326/0003-4819-146-10-200705150-00006. [DOI] [PubMed] [Google Scholar]
- 8.Wood PB, Holman AJ, Jones KD. Novel pharmacotherapy for fibromyalgia. Expert Opin Investig Drugs. 2007;16:829–841. doi: 10.1517/13543784.16.6.829. [DOI] [PubMed] [Google Scholar]
- 9.Bergman S. Management of musculoskeletal pain. Best Pract Res Clin Rheumatol. 2007;21:153–166. doi: 10.1016/j.berh.2006.10.001. [DOI] [PubMed] [Google Scholar]
- 10.Arnold LM, Clauw DJ, Dunegan LJ, Turk DC FibroCollaborative. A framework for fibromyalgia management for primary care providers. Mayo Clin Proc. 2012;87:488–496. doi: 10.1016/j.mayocp.2012.02.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bhatty SA, Shaikh NA, Irfan M, Kashif SM, Vaswani AS, Sumbhai A, et al. Vitamin D deficiency in fibromyalgia. J Pak Med Assoc. 2010;60:949–951. [PubMed] [Google Scholar]
- 12.Atherton K, Berry DJ, Parsons T, Macfarlane GJ, Power C, Hyppönen E. Vitamin D and chronic widespread pain in a white middle-aged British population: evidence from a cross-sectional population survey. Ann Rheum Dis. 2009;68:817–822. doi: 10.1136/ard.2008.090456. [DOI] [PubMed] [Google Scholar]
- 13.Plotnikoff GA, Quigley JM. Prevalence of severe hypovitaminosis D in patients with persistent, nonspecific musculoskeletal pain. Mayo Clin Proc. 2003;78:1463–1470. doi: 10.4065/78.12.1463. [DOI] [PubMed] [Google Scholar]
- 14.Altindag O, Ögüt E, Gur A, Gursoy S, Gunay M. Serum vitamin D level and its relation with clinical parameters in fibromyalgia as a neuropathic pain. Orthop Muscular Syst. 2014;3:171. [Google Scholar]
- 15.Ulusoy H, Sarica N, Arslan S, Ozyurt H, Cetin I, Birgul Ozer E, et al. Serum vitamin D status and bone mineral density in fibromyalgia. Bratisl Lek Listy. 2010;111:604–609. [PubMed] [Google Scholar]
- 16.Okumus M, Koybası M, Tuncay F, Ceceli E, Ayhan F, Yorgancioglu R, et al. Fibromyalgia syndrome: is it related to vitamin D deficiency in premenopausal female patients? Pain Manag Nurs. 2013;14:e156–e163. doi: 10.1016/j.pmn.2011.09.006. [DOI] [PubMed] [Google Scholar]
- 17.Moher D, Liberati A, Tetzlaff J, Altman DG PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol. 2009;62:1006–1012. doi: 10.1016/j.jclinepi.2009.06.005. [DOI] [PubMed] [Google Scholar]
- 18.Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33:159–174. [PubMed] [Google Scholar]
- 19.Higgins JP, Green S. Cochrane handbook for systematic reviews of interventions version 5.1.0 [Internet] London: The Cochrane Collaboration; 2011. [cited 2011 March 3]. Available at http://handbook.cochrane.org. [Google Scholar]
- 20.Viswanathan M, Ansari MT, Berkman ND, Chang S, Hartling L, McPheeters M, et al. Assessing the risk of bias of individual studies in systematic reviews of health care interventions [Internet] Rockville (MD): Agency for Healthcare Research and Quality; 2012. [cited 2012 March 8]. Available at https://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0077771/ [PubMed] [Google Scholar]
- 21.Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21:1539–1558. doi: 10.1002/sim.1186. [DOI] [PubMed] [Google Scholar]
- 22.Al-Allaf AW, Mole PA, Paterson CR, Pullar T. Bone health in patients with fibromyalgia. Rheumatology (Oxford) 2003;42:1202–1206. doi: 10.1093/rheumatology/keg356. [DOI] [PubMed] [Google Scholar]
- 23.Maafi AA, Ghavidel-Parsa B, Haghdoost A, Aarabi Y, Hajiabbasi A, Shenavar Masooleh I, et al. Serum vitamin D status in Iranian fibromyalgia patients: according to the symptom severity and illness invalidation. Korean J Pain. 2016;29:172–178. doi: 10.3344/kjp.2016.29.3.172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Balkarli A, Balkarlı H, Temel S, Ozhan N, Ozkan U, Cobankara V. AB0656 Serum vitamin D and parathyroid hormone levels in premenopausal women with fibromyalgia syndrome. Ann Rheum Dis. 2013;72:A989 [Google Scholar]
- 25.Mateos F, Valero C, Olmos JM, Casanueva B, Castillo J, Martínez J, et al. Bone mass and vitamin D levels in women with a diagnosis of fibromyalgia. Osteoporos Int. 2014;25:525–533. doi: 10.1007/s00198-013-2434-2. [DOI] [PubMed] [Google Scholar]
- 26.Monteiro DM. Evaluation of vitamin D status in a population with fibromyalgia [master thesis] Coimbra: Univ. of Coimbra; 2011. [Google Scholar]
- 27.Özcan DS, Öken Ö, Aras M, Köseoğlu BF. Vitamin D levels in women with fibromyalgia and relationship between pain, depression, and sleep. Turk J Phys Med Rehabil. 2014;60:329–334. [Google Scholar]
- 28.de Rezende Pena C, Grillo LP, das Chagas Medeiros MM. Evaluation of 25-hydroxyvitamin D serum levels in patients with fibromyalgia. J Clin Rheumatol. 2010;16:365–369. doi: 10.1097/RHU.0b013e3181fe8a90. [DOI] [PubMed] [Google Scholar]
- 29.Tandeter H, Grynbaum M, Zuili I, Shany S, Shvartzman P. Serum 25-OH vitamin D levels in patients with fibromyalgia. Isr Med Assoc J. 2009;11:339–342. [PubMed] [Google Scholar]