

Abstract
Background
Health care services effort to provide alternative cardiac rehabilitation (CR) models to serve patients according to their preferences and needs. So, the present study aimed to assess and compare the effects of hospital-based and hybrid CR programs on chest pain intensity and discomfort in cardiac surgery patients.
Methods
In this prospective study, 110 cardiac surgery patients were invited to the CR department of a hospital in the western part of Iran between March and July 2016. Patients were divided into two groups: hospital-based and hybrid CR. The hospital-based program included 26 sessions, and the hybrid program included 10 training sessions and exercise. The Brief Pain Inventory and Pain Discomfort Scale were used as research instrument, and data were analyzed using the paired t-test and ANCOVA.
Results
The results indicated that both hospital-based and hybrid CR are effective in reducing the chest pain intensity and discomfort of cardiac surgery patients (P < 0.05). In addition, the comparison of scores before and after treatment using ANCOVA shows that no significant differences were observed between the two programs (P > 0.05).
Conclusions
Traditional hospital-based CR delivery is still the first choice for treatment in developing countries. However, hybrid CR is as effective as a hospital-based program in reducing pain components and it includes only 38% of the total cost in comparison to hospital-based delivery. So, we recommend using hybrid CR according with the recommendations of American Heart Association about using CR for the management of angina symptoms.
Keywords: Cardiovascular disease, Cost-benefit analysis, Home care services, Hospitals, Pain, Rehabilitation, Surgery
INTRODUCTION
Cardiac rehabilitation (CR) is a necessary effort in secondary prevention which helps patients' effective healing and in preserving their quality of life [1]. CR can be provided to patients in various formats, including multi-factorial call health services, internet-based presentations, call health services focused on exercise and recovery, home-based or hybrid CR, and specialized programs for departed and rural areas with different cultures and languages [2]. Despite this, in developing countries such as Iran, the traditional hospital-based delivery format is the first choice of treatment [3]. This delivery format is confronted with important challenges such as cost and access [3]. So, health care services have started making efforts to replace alternative CR policies in order to monopolize their services for patient's care, needs, and preferences [4].
Hybrid CR is one of the most cost-effective models which strongly influences the control of cardiac risk factors [4,5], improvement of exercise capacity, commitment to treatment, reducing complications and improving patient's quality of health [6,7]. Despite this, there are few studies that demonstrate its effect on reducing the risk of angina and other related psychological symptoms. Angina-associated chest pain is considered a significant cardiac risk factor which is associated with increased risk of cardiac mortality [8]. The results of a study showed that the exercise-based CR improved unstable angina [9]. Meanwhile, Piestrzeniewicz et al. [10] found that comprehensive hospital-based CR is significantly effective in reducing patient's chest pain after acute myocardial infarction treated with primary coronary intervention. In addition, the results of another report indicates that hospital-based CR has no effect on the frequency and the severity of angina [11]. Considering that other forms of CR have been less studied, the impact of alternative delivery formats on chest pain must be checked. Based on this consideration, the present study aims to investigate the effect of hybrid CR on patient's pain severity and discomfort by comparing this model and hospital-based CR.
MATERIALS AND METHODS
1. Study design and subjects
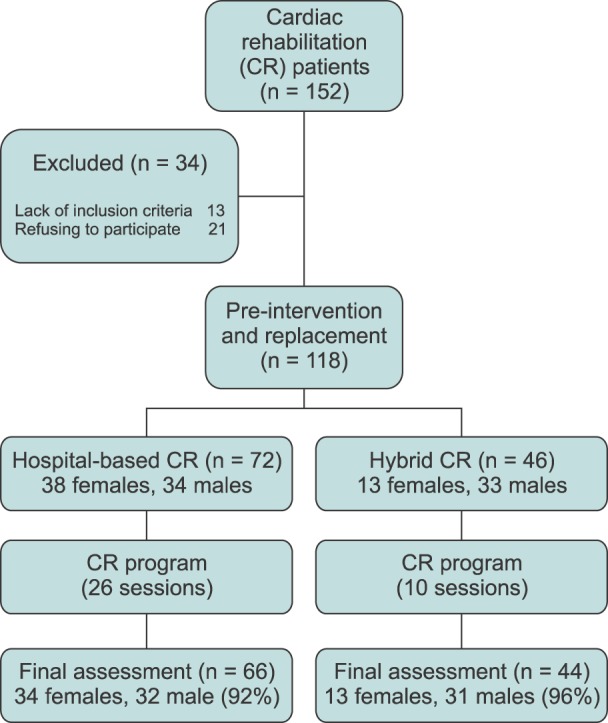
In this prospective study, cardiac surgery patients were invited to participate in a CR program after coronary artery bypass grafting (CABG) or valve replacement at Imam Ali hospital of Kermanshah city during March–July 2016. Initially, 152 persons were referred to the CR center. After applying our exclusion criteria, 42 were excluded as they were unwilling. Eventually, data for 110 people was analyzed (Fig. 1).
Fig. 1. Flow chart.
2. Inclusion criteria
Inclusion criteria included fluency in the Persian language, an age of between 30–75 years, lack of mobility or limited movement, and beginning participation in an exercise regimen according to the time planning of the outpatient CR team.
3. Exclusion criteria
Exclusion criteria were severe pain or stable dyspnea in the chest during aerobic exercise, serious health problems during exercise, and participation less than 90% of the CR sessions.
4. Interventions
1) Outpatient CR protocol
The CR program in Imam Ali hospital of Kermanshah is provided to patients in two formats: Hospital-based and hybrid CR programs. The baseline inclusion of patients was done in two phases. In the first phase, a cardiologist assessed the case's severity (low, medium, and high risk). The distance of patient's residence to the CR center was recorded in the second phase. So, the patients were divided into two groups: patients residing in Kermanshah city and those residing in neighboring cities. Then, based on the patients recorded information and level of cardiac risk. High-risk patients entered the hospital-based exercise program under the supervision of a treatment team blinded to their distance and situations. Patients with a low to medium level of risk who live in Kermanshah city were included in the hospital-based program. But those who had a low to medium level of risk, and live in neighboring cities, were included in the hybrid program, after completing a consent form.
In the hospital-based CR program, patients participated in a 1-hour exercise session (including a warm-up session for 10 min), dynamic exercise (45 min), and recovery (5 min), three times a week, totaling 26 sessions over 8 weeks. The dynamic exercise included strenuous movements and running on a treadmill. Otherwise, in the hybrid CR program, patients participated in a 2-hours training session and 1-hour exercise session (with 1 session a week for 10 weeks). The CR training sessions were focused on management of risk factors, healthy nutrition, weight control and stress management. One of the family members of illiterate patients was asked to participate in the training sessions. At the end of every session, hybrid CR patients were asked to do aerobic exercise, especially walking exercise, for five days of a week, as well as relaxation techniques. The results were recorded accordingly. The costs the CR program incurred was in accordance with the four health insurances acts in Iran, which include medical services, social security organization, the armed forces, and the Imdad Committee. They met 70% of the cost for 10 sessions, 70% of the total cost, 90% of 20 sessions, and 90% of the total cost, respectively, whereas additional costs, if any, were paid by the patients [3].
2) The exercise protocol
The American College of Sports Medicine (ACSM) guidelines (2005) were used as a basis for exercise prescription for patients in the current study. The Bruce protocol was used to calculate the intensity of exercise. Initially, the exercise intensity was calculated based on heart rate reserve obtained during the graded exercise test and the rating of perceived exertion. Then, target heart rate range (HRR), using the Karvonen formula, was used to prescribe exercise intensity. Graded aerobic training was mainly treadmill walking three times per week (and once for patients in the hybrid CR group), with an intensity of 40–70% of HRR, obtained in the exercise test, and a rating of perceived exertion of 11–14 for a duration of 20–45 min [12].
5. Methods of measurement
Initially, in accordance with the directions of the ethical committee of the Kermanshah University of Medical Sciences and the Helsinki Declaration, all patients gave their prior written consent to participate in this study. Then, the patients provided information regarding demographic data such as gender and marital status, along with clinical variables such as type of cardiac intervention and process, being overweight, smoking history, and histories of myocardial infarction (MI), hypertension, diabetes, and hyperlipidemia were recorded routinely by a cardiologist and clinical psychologist in the CR center 1 week before beginning the exercise program. The chief nurse recorded the presence of the patients in sessions as a daily note. The questionnaires of pain severity and discomfort were provided to patients 1 week before exercise and 1 week after CR. Educated people fulfilled out these questionnaires individually after receiving necessary explanations, but the psychologist read the items for illiterate patients and recorded their responses.
1) Brief Pain Inventory (BPI)
This scale grades the severity of pain on a 10-degree scale where zero indicates the absence of pain and ten indicates very severe pain. The reliability and validity of this scale were reported by Mirzamani et al. [13], and is acceptable in the population of Iran.
2) Pain Discomfort Scale
This scale provided by Jensen et al. in 1992 evaluates the emotional distress from pain. The items 1, 2, 3, 6, and 10 are scored directly while the items 4, 5, 7, 8, and 9 are scored indirectly. The items are scored in 0–4 degrees. The higher scores indicate more emotional distress and depression. Jensen et al. [14] reported its validity and reliability as acceptable. The retest reliability of this scale was reported as 0.76. In addition, its reliability related to the Beck Depression Inventory and Affective Pain scale from the McGill Pain Questionnaire are reported as 0.58 and 0.38 respectively [14].
6. Statistical analysis
The Chi-square test was used for nominal and classified variables (gender, marital status, type of cardiac intervention and process, being overweight, smoking history, and histories of MI, hypertension, diabetes, and hyperlipidemia) and the independent t-test was used for continuous variables (age, pain intensity, and pain discomfort) to compare the characteristics of patients in the hybrid and hospital-based CR groups.
The data are presented as percentages for non-continuous variables and as mean ± standard deviations for continuous variables. Finally, the paired t-test was used to assess the effect of each program on the severity and discomfort of pain. The scores before and after the two programs were compared by applying ANCOVA [15]. Before the analysis, the needed statistical presumptions for ANCOVA were assessed [15]. The baseline differences between the two groups for gender were adjusted, as these variables tend to confound pain intensity and discomfort.
All the differences were considered significant at 0.05 levels, and the data analysis was performed using SPSS (ver 20.0).
RESULTS
Baseline data regarding demographic variables, pain intensity and discomfort are presented in Table 1. Significant differences were observed between the two groups for gender (P < 0.05, Table 1).
Table 1. Baseline Demographics and Pain Discomfort and Intensity of Patients.

CABG: coronary artery bypass surgery, MI: myocardial infarction, CR: cardiac rehabilitation. *Data are presented as mean ± standard deviation. †Independent t test was used for the analyze. ‡Chi-square was used for the analyze.
Table 2 shows the effect of each CR in reducing pain severity and discomfort. According to the results, both programs independently are effective in reducing the severity and discomfort of pain (P < 0.05, Table 2). Finally, after controlling the effects of gender and pain severity and discomfort at baseline (pre-intervention), the results of ANCOVA shows that no significant differences were observed between the two programs (P > 0.05). So, the hybrid CR is as effective as a hospital-based program in reducing pain components (Table 2).
Table 2. Scores of Pre-post Intervention in Each Program.

Data are presented as mean ± standard deviation. *Statistical significance (P < 0.05) in pre- and post CR within each program.
DISCUSSION
In order to identify the cost-effective and appropriate program according to the needs of the patients, the present study was designed to assess and compare the impact of hospital-based and hybrid CR programs on chest pain intensity and discomfort. The present results show that no significant differences were observed between the two programs for lessening the pain intensity and discomfort in cardiac surgery patients. In other words, neither of the programs are superior to the other. Our findings are consistent with the results of previous studies on the effect of CR programs on pain components [9,10].
According to the obtained results, a question is posed: how do CR programs decrease the severity and discomfort of pain? It seems that a CR program, especially regular exercise, is a serious obstacle to the progression of coronary atherosclerosis among cardiac patients [16]. Regular follow up of a CR program by each patient increases the chest pain threshold. On the other hand, CR and exercise training can decrease arterial wall thickness in cardiovascular patients. Also, this situation actually alleviates chest pain in the patients [16]. Hence, patients report less pain at the end of the CR programs.
Despite the emphasis of the American Heart Association guidelines on comprehensive delivery of CR programs [17], it seems that these programs have not been implemented in accordance with the treatment of cardiovascular diseases and cardiac care [18]. However, it cannot be deduced whether these programs are effective for CR in cases of angina or not, as the published reports are not in agreement. One of these studies indicated that hospital-based CR had no effect on reducing the frequency and severity of angina [11]. On the other hand, the other studies found the same as the present study, indicating the effect of exercise-based CR program on reducing hypertension and chest pain among angina patients [9,19]. Angina is related to increased psychological morbidity and lower quality of life [20]. On the other hand, CR is accompanied by an increased quality of life through decreased psychological morbidity [21]. In addition, it seems that angina management programs which include cognitive-behavioral principles are imperative to positive outcomes [22].
Now, one of the serious problems of hospital-based CR is the lack of patients' tendency to participate in these programs, as it is evident that a lesser number of patients opted for hospital-based CR [23]. The traditional model of hospital-based CR is confronted with important challenges such as cost and access. So, nowadays, the cost effectiveness and better care by traditional CR methods have engrossed the attention of health care professionals [3]. Hybrid CR has been shown to be one of the most cost-efficient delivery formats, with only 38% of the total cost in comparison to the hospital-based delivery format [3]. Based on past reports [5,6,7], hybrid CR has a significant effect on reducing risk factors and increasing physical capacity and a return to work.
The results of the present study indicate the effect of this delivery format on reducing chest pain severity and discomfort in cardiac patients. In this hybrid CR, patients receive psychological training based on cognitive-behavioral principles in addition to regular exercise and nutritional management. So, this delivery format can correct the misconceptions about cardiac symptoms [22] and can help to reduce pain severity and discomfort in addition to the positive effect on patients' physical conditions [5,6,7].
In summation, traditional hospital-based CR delivery format is still the first choice of treatment in developing countries. However, hybrid CR is as effective as a hospital-based program in reducing pain components and it requires only 38% of the total cost in comparison to hospital-based delivery. So, we recommend using hybrid CR in accordance with the recommendations of the American Heart Association about using CR for the management of angina symptoms.
The lack of using a randomized replacement in the two delivery formats, hospital-based and hybrid CRs, and the lack of follow-up of treatment outcomes are limitations of the present study. In future studies, randomized replacement of patients can control the probable bias of the outcomes. Given that high-risk patients should be fully monitored by a health team, it is recommended that in future studies only low to medium risk patients should be replaced and compared in these two programs. The lack of control of the effect of medications was another limitation of this study. In addition, only CABG and valve replacement patients are included, and the results on other cardiac patients including MI and percutaneous coronary intervention will clear the overall picture.
References
- 1.Williams MA, Kaminsky LA. Healthy lifestyle medicine in the traditional healthcare environment-primary care and cardiac rehabilitation. Prog Cardiovasc Dis. 2017;59:448–454. doi: 10.1016/j.pcad.2017.01.008. [DOI] [PubMed] [Google Scholar]
- 2.Komasi S, Saeidi M, Ezzati P, Amirian J. How can we deliver outpatient cardiac rehabilitation services to all low-risk patients in Iran. Res Cardiovasc Med. 2017;6:e43585 [Google Scholar]
- 3.Komasi S, Saeidi M. Hybrid cardiac rehabilitation as an alternative to common hospital-based cardiac rehabilitation in Iran: an appropriate model for the Iranian health system limitations, culture, and patients. Res Cardiovasc Med. 2017;6:e39367 [Google Scholar]
- 4.Clark RA, Conway A, Poulsen V, Keech W, Tirimacco R, Tideman P. Alternative models of cardiac rehabilitation: a systematic review. Eur J Prev Cardiol. 2015;22:35–74. doi: 10.1177/2047487313501093. [DOI] [PubMed] [Google Scholar]
- 5.Korzeniowska-Kubacka I, Dobraszkiewicz-Wasilewska B, Bilińska M, Rydzewska E, Piotrowicz R. Two models of early cardiac rehabilitation in male patients after myocardial infarction with preserved left ventricular function: comparison of standard out-patient versus hybrid training programmes. Kardiol Pol. 2011;69:220–226. [PubMed] [Google Scholar]
- 6.Korzeniowska-Kubacka I, Bilińska M, Dobraszkiewicz-Wasilewska B, Piotrowicz R. Hybrid model of cardiac rehabilitation in men and women after myocardial infarction. Cardiol J. 2015;22:212–218. doi: 10.5603/CJ.a2015.0004. [DOI] [PubMed] [Google Scholar]
- 7.Najafi F, Nalini M. Hospital-based versus hybrid cardiac rehabilitation program in coronary bypass surgery patients in western Iran: effects on exercise capacity, risk factors, psychological factors, and quality of life. J Cardiopulm Rehabil Prev. 2015;35:29–36. doi: 10.1097/HCR.0000000000000087. [DOI] [PubMed] [Google Scholar]
- 8.Strand E, Pedersen ER, Svingen GF, Olsen T, Bjørndal B, Karlsson T, et al. Serum acylcarnitines and risk of cardiovascular death and acute myocardial infarction in patients with stable angina pectoris. J Am Heart Assoc. 2017;6:e003620. doi: 10.1161/JAHA.116.003620. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Babu AS, Noone MS, Narayanan SM, Franklin BA. Exercise based cardiac rehabilitation for unstable angina: a case report. Oman Med J. 2012;27:e034. doi: 10.5001/omj.2012.42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Piestrzeniewicz K, Navarro-Kuczborska N, Bolińska H, Jegier A, Maciejewski M. The impact of comprehensive cardiac rehabilitation in patients up to 55 years old after acute myocardial infarction treated with primary coronary intervention. Pol Arch Med Wewn. 2004;111:309–317. [PubMed] [Google Scholar]
- 11.Asbury EA, Webb CM, Probert H, Wright C, Barbir M, Fox K, et al. Cardiac rehabilitation to improve physical functioning in refractory angina: a pilot study. Cardiology. 2012;122:170–177. doi: 10.1159/000339224. [DOI] [PubMed] [Google Scholar]
- 12.American College of Sports Medicine. ACSM's guidelines for exercise testing and prescription. 7th ed. Philadelphia (PA): Lippincott Williams & Wilkins; 2006. [Google Scholar]
- 13.Mirzamani SM, Sadidi A, Salimi SH, Besharat MA. Validation of the Persian version of the brief pain inventory. Acta Med Iran. 2005;43:425–428. [Google Scholar]
- 14.Jensen MP, Karoly P, Harris P. Assessing the affective component of chronic pain: development of the pain discomfort scale. J Psychosom Res. 1991;35:149–154. doi: 10.1016/0022-3999(91)90069-z. [DOI] [PubMed] [Google Scholar]
- 15.Pallant J. SPSS survival manual: a step by step guide to data analysis using SPSS for windows (version 12) 2nd ed. Crows Nest: Allen & Unwin; 2005. pp. 142–152. [Google Scholar]
- 16.Nytrøen K, Gullestad L. Exercise after heart transplantation: an overview. World J Transplant. 2013;3:78–90. doi: 10.5500/wjt.v3.i4.78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Fletcher GF, Balady GJ, Amsterdam EA, Chaitman B, Eckel R, Fleg J, et al. Exercise standards for testing and training: a statement for healthcare professionals from the American Heart Association. Circulation. 2001;104:1694–1740. doi: 10.1161/hc3901.095960. [DOI] [PubMed] [Google Scholar]
- 18.Heydarpour B, Saeidi M, Ezzati P, Soroush A, Komasi S. Sociodemographic predictors in failure to complete outpatient cardiac rehabilitation. Ann Rehabil Med. 2015;39:863–871. doi: 10.5535/arm.2015.39.6.863. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Mazumdar S, Kumar A, Verma SK. Effect of cardiac rehabilitation on blood pressure in stable angina patients. J Exerc Sci Physiother. 2014;10:54–59. [Google Scholar]
- 20.Moore RK, Groves D, Bateson S, Barlow P, Hammond C, Leach AA, et al. Health related quality of life of patients with refractory angina before and one year after enrolment onto a refractory angina program. Eur J Pain. 2005;9:305–310. doi: 10.1016/j.ejpain.2004.07.013. [DOI] [PubMed] [Google Scholar]
- 21.Moore R, Groves D, Hammond C, Leach A, Chester MR. Temporary sympathectomy in the treatment of chronic refractory angina. J Pain Symptom Manage. 2005;30:183–191. doi: 10.1016/j.jpainsymman.2005.02.016. [DOI] [PubMed] [Google Scholar]
- 22.Furze G. Angina rehabilitation: exercise is not enough. Procedia Soc Behav Sci. 2010;5:1545–1549. [Google Scholar]
- 23.Moradi B, Maleki M, Esmaeilzadeh M, Abkenar HB. Physician-related factors affecting cardiac rehabilitation referral. J Tehran Heart Cent. 2011;6:187–192. [PMC free article] [PubMed] [Google Scholar]