

Abstract
Case
We report a case with concurrent ingestion of carbamazepine (CBZ) overdose and grapefruit juice. A 23‐year‐old man, with a history of epilepsy, was admitted to our emergency department 2 h after ingesting 10 g CBZ with 1 L grapefruit juice. On arrival, the patient's Glasgow Coma Scale score was 9 and he showed signs of restlessness. Grapefruit juice‐like gastric fluid, with tablet residue, was observed in his stomach after we inserted a gastric tube. Our initial test detected a blood CBZ level of 41.5 mg/L.
Outcome
We treated the patient with gastric lavage, activated charcoal, and charcoal hemoperfusion. His blood CBZ level began to decrease after gastrointestinal decontamination, and he was discharged without any sequelae on day 9.
Conclusion
Gastric lavage or aspiration may be considered in cases where drug residue is found in the stomach, especially if materials are involved that might exacerbate the drug's toxicity.
Keywords: Blood concentration, carbamazepine, gastrointestinal decontamination, grapefruit juice, overdose
Introduction
Carbamazepine (CBZ) is one of the most commonly prescribed anticonvulsant agents, and it is widely used to treat epilepsy, manic depression, schizophrenia, and trigeminal neuralgia throughout the world. Patients treated with CBZ are advised to avoid consuming grapefruit juice, as it is known to increase the blood concentration of CBZ.1 In the present report, we describe the successful treatment of a case with concurrent ingestion of CBZ overdose and grapefruit juice.
Case
A 23‐year‐old man was transported to our emergency department 2 h after having ingested 100 tablets of CBZ (100 mg/tablet) and having simultaneously drunk 1 L of 100% grapefruit juice. The patient's body weight was 60 kg, and he had a history of epilepsy, which was treated with CBZ (200 mg/day).
On arrival, the patient's Glasgow Coma Scale score was 9 (eye, 2; verbal, 2; motor, 5), and he showed signs of restlessness. A blood test revealed the patient's CBZ level was 41.5 mg/L (Fig. 1). His blood pressure was 117/82 mmHg, pulse rate was 113 b.p.m., respiratory rate was 20 breaths/min, and temperature was 35.7°C. On physical examination, auscultation revealed normal respiratory and heart sounds, although abdominal examination revealed hypoperistalsis. The patient showed no signs of seizures, had normal electrocardiogram results, and no other symptoms were detected in our systemic examination.
Figure 1.
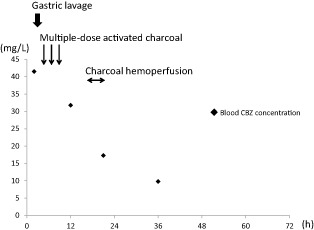
Clinical course and blood carbamazepine (CBZ) concentration over time in a 23‐year‐old man admitted to the emergency department 2 h after ingesting 10 g CBZ with 1 L grapefruit juice. Y axis: Blood carbamazepine concentration (mg/L). X axis: Time from ingestion (h) Gastric lavage was carried out immediately after the patient was admitted, and he was subsequently started on activated charcoal with sodium citrate (first dose, 50 g; 25 g per 2 h thereafter). Thirteen hours after admission, hemoperfusion was initiated for 4 h. ◆, Measured values for CBZ concentration.
After inserting a gastric tube, we observed approximately 600 mL grapefruit juice‐like gastric fluid with white tablet residue in the stomach; therefore, 6 L gastric lavage was carried out after tracheal intubation. Continuous infusion of propofol and mechanical ventilation were initiated, and 50 g activated charcoal with 50 g magnesium citrate was administered through the gastric tube. Thereafter, 25 g doses of activated charcoal with 25 g magnesium citrate were repeated every 2 h. After three doses, the patient was unable to defecate and developed metallic sounds in his abdomen; therefore, we discontinued the charcoal treatment. The metallic sounds subsided after the patient underwent an enema and defecated. However, 12 h after ingestion, his CBZ levels were still elevated (31.8 mg/L); therefore, 4 h of charcoal hemoperfusion (Medisorba; Asahi Kasei Medical Co, Tokyo, Japan) was carried out. The blood flow rate was 150 mL/min, and heparin anticoagulation was provided as a 1,000 U bolus infusion, followed by continuous infusion at 1,000 U/h. Following the hemoperfusion (21 h after ingestion), the patient's CBZ levels decreased to 17.3 mg/L; 36 h after ingestion his CBZ levels had further decreased to 9.8 mg/L. Thus, the propofol was discontinued, and after the patient regained consciousness, the tracheal tube was extubated. Oral treatment with CBZ (200 mg/day) was restarted on day 4. After a psychiatric consultation, the patient was discharged on day 9 without any sequelae.
Discussion
Although useful as an anticonvulsant agent, CBZ has been known to induce coma, seizures, respiratory depression, and arrhythmia when consumed in large quantities.2 In doses >50 mg/kg, CBZ ingestion is thought to cause fluctuation in mental status that is followed by coma, which requires intubation and ventilation within 12 h.2 Carbamazepine has also been reported to cause toxicity when its blood concentration is >20 mg/L,3 and blood concentrations >40 mg/L are associated with severe toxic symptoms.4 In the present case, the patient had ingested 10 g (167 mg/kg) CBZ and showed impaired consciousness during his admission. In addition, the patient's blood CBZ concentration reached 41.5 mg/L, with symptoms that were consistent with CBZ overdose.
Recently, it has been reported that gastric lavage should not be routinely carried out to manage cases of poisoning.5 In addition, gastric lavage has previously been indicated if a patient presents within 1 h of a massive CBZ overdose.3 However, CBZ also has an anticholinergic effect that causes diminished peristalsis, which can delay the processing of the ingested materials. In the present case, we observed that approximately 600 mL grapefruit juice‐like gastric fluid, with white tablet residue, was still present in the patient's stomach when we inserted the gastric tube (2 h after ingestion). Although there was no conclusive evidence that the gastric fluid and tablets were pure grapefruit juice and CBZ, respectively, the findings suggested that a large quantity of these materials was still present in the stomach.
Grapefruit juice has been reported to increase blood CBZ concentrations.1 The presumed mechanism for this effect is the inhibition of cytochrome P450 3A4 (CYP3A4) by furanocoumarins, which increases the bioavailability of CBZ.6 The combination of CBZ and grapefruit juice could result in an extended period of elevated blood CBZ concentration, highlighting the need to suppress any future increases in the CBZ concentration. Although the peak blood CBZ concentration typically appears 6–24 h after ingesting a normal therapeutic dose,3 a massive overdose may delay the peak concentration until more than 72 h after ingestion.7 In cases of CBZ overdose, blood CBZ concentrations have also been known to continue rising after the initial measurement.8 Although there was a concern that the extended increase in CBZ concentration was caused by grapefruit juice, the CBZ concentration had decreased by the second measurement (at 12 h, Fig. 1). Therefore, it appears that gastric lavage might suppress any delayed increase in CBZ concentration. In similar cases, gastric lavage or aspiration might be considered to avoid the massive increase in CBZ concentration, even if more than 1 h has passed since ingestion.
In addition to the gastric lavage, we provided multiple doses of activated charcoal, which has been used in cases of CBZ overdose to reduce the period of toxicity.2, 3, 9 In theory, the charcoal reducing the absorption from the intestine might be more important in cases with CYP3A4 inhibition than in cases without CYP3A4 inhibition. Hemoperfusion or hemodialysis have also been reported as effective in eliminating blood CBZ.10 Although the charcoal hemoperfusion was followed by discontinuation of the activated charcoal, the patient's CBZ concentration had already decreased to below 40 mg/L, indicating that the greatest risk of toxicity had passed. We believe that the hemoperfusion reduced the duration of the toxicity, although it is unclear whether the hemoperfusion was necessary for the patient's survival.
Conclusion
Gastric lavage or aspiration may be considered in cases where drug residue is found in the stomach even after 1 h following ingestion, especially if other materials are involved that might exacerbate the drug's toxicity.
Conflict of Interest
None.
References
- 1. Garg SK, Kumar N, Bhargava VK, Prabhakar SK. Effect of grapefruit juice on carbamazepine bioavailability in patients with epilepsy. Clin. Pharmacol. Ther. 1998; 64: 286–288. [DOI] [PubMed] [Google Scholar]
- 2. Soderstrom J, Murray L, Little M, Daly FF. Toxicology case of the month: Carbamazepine overdose. Emerg. Med. J. 2006; 23: 869–871. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Jones AL, Proudfoot AT. Features and management of poisoning with modern drugs used to treat epilepsy. QJM 1998; 91: 325–332. [DOI] [PubMed] [Google Scholar]
- 4. Hojer J, Malmlund HO, Berg A. Clinical features in 28 consecutive cases of laboratory confirmed massive poisoning with carbamazepine alone. J. Toxicol. Clin. Toxicol. 1993; 31: 449–458. [DOI] [PubMed] [Google Scholar]
- 5. Benson BE, Hoppu K, Troutman WG et al Position paper update: Gastric lavage for gastrointestinal decontamination. Clin. Toxicol. (Phila.) 2013; 51: 140–146. [DOI] [PubMed] [Google Scholar]
- 6. Fukuda K, Ohta T, Oshima Y, Ohashi N, Yoshikawa M, Yamazoe Y. Specific CYP3A4 inhibitors in grapefruit juice: Furocoumarin dimers as components of drug interaction. Pharmacogenetics 1997; 7: 391–396. [DOI] [PubMed] [Google Scholar]
- 7. de Zeeuw RA, Westenberg HG, van der Kleijn E, Gimbrère JS. An unusual case of carbamazepine poisoning with a near‐fatal relapse after two days. Clin. Toxicol. 1979; 14: 263–269. [DOI] [PubMed] [Google Scholar]
- 8. Patel VH, Schindlbeck MA, Bryant SM. Delayed elevation in carbamazepine concentrations after overdose: A retrospective poison center study. Am. J. Ther. 2013; 20: 602–606. [DOI] [PubMed] [Google Scholar]
- 9. Montoya‐Cabrera MA, Sauceda‐García JM, Escalante‐Galindo P, Flores‐Alvarez E, Ruiz‐Gómez A. Carbamazepine poisoning in adolescent suicide attempters. Effectiveness of multiple‐dose activated charcoal in enhancing carbamazepine elimination. Arch. Med. Res. 1996; 27: 485–489. [PubMed] [Google Scholar]
- 10. Tapolyai M, Campbell M, Dailey K, Udvari‐Nagy S. Hemodialysis is as effective as hemoperfusion for drug removal in carbamazepine poisoning. Nephron 2002; 90: 213–215. [DOI] [PubMed] [Google Scholar]