

Abstract
Case
A 69 year‐old female with history of schizophrenia was transported to our hospital by ambulance due to coma. On arrival, she was hypotensive and tachycardic with a Glasgow coma scale score of 3 and a rectal core temperature of 40°C. Heatstroke was strongly suspected as the cause of the coma and hypotension. Active external cooling with an electric fan and cooled IV fluid administration were started. Her electrocardiogram (EKG) showed ST elevation in V2‐6, II, III and aVF. Echocardiography revealed apical ballooning, which indicated Takotsubo cardiomyopathy. Coronary angiography indicated normal coronary arteries.
Outcome
After admission to the intensive care unit, her cardiovascular status gradually improved and she was transferred to the psychiatric ward on day 36.
Conclusion
Heatstroke and Takotsubo cardiomyopathy can share the same pathophysiology. Close evaluation of hemodynamic status and myocardial damage is critical for survival.
Keywords: Circulation, echocardiography, heatstroke, shock, Takotsubo cardiomyopathy
Introduction
Heatstroke is a life‐threatening condition caused by prolonged exposure to a high temperature environment or excessive physical activity. Core body temperature can be greater than 40°C, which can lead to multiorgan failure including hematologic, hepatic, renal and cardiovascular dysfunction. With delayed therapy, the mortality rate can be as high as 70%, especially among the elderly population. Early diagnosis and management with immediate cooling can reduce the mortality rate to 10%.1 The most common cause of death is multiple organ failure including refractory cardiovascular failure. The pathophysiology of cardiovascular dysfunction due to heatstroke includes hypovolemia and decreased peripheral vascular tonus.1 It is reported that heatstroke can also cause myocardial damage.2 Here, we report a case of heatstroke presented with ST‐elevation on electrocardiography (ECG), echocardiography and coronary angiography, revealing a rare complication of stress‐induced myocardial dysfunction, known as Takotsubo cardiomyopathy (TCM).
Case Report
A 69‐year‐old female with history of schizophrenia being treated with blonanserin and flunitrazepam, was found unconscious in the backyard of her house at noon one summer day. She was immediately transferred to our emergency department by ambulance. On admission, physical examination revealed a Glasgow Coma Scale score of 3, and heart rate of 162 beats/min. Her blood pressure was immeasurable and her rectal core temperature was as high as 40.6°C. Endotracheal intubation was immediately performed. To decrease body temperature, cooled IV fluids were administered, together with external cooling with a water spray and an electric fan.
Laboratory data showed elevated serum creatine kinase, creatine‐kinase‐MB, BUN, creatinine, and positive troponin‐T (Table 1). ECG found ST elevation in V2‐6, II, III, and aVF (Fig. 1A). Transthoracic echocardiography revealed severe systolic dysfunction with ballooning of distal and apical wall, which indicated possible TCM (Fig. 2A, B, and Supporting Information 1).
Table 1.
Clinical laboratory findings of the case
| Hematology | Biochemistory | ||
|---|---|---|---|
| WBC | 12,800/μL | CRP | 0.1 mg/dL |
| RBC | 449 × 104/μL | TP | 7.8 g/dL |
| Hb | 13.3 g/dL | Alb | 4.8 g/dL |
| Ht | 39.3% | AST | 91 IU/L |
| Plt | 25.4 × 104/μL | ALT | 24 IU/L |
| LDH | 402 IU/L | ||
| CPK | 883 IU/L | ||
| CPK‐MB | 34 IU/L | ||
| ALP | 391 IU/L | ||
| γGTP | 15 IU/L | ||
| BUN | 29 mg/dL | ||
| Cre | 2.12 mg/dL | ||
| T‐Bil | 0.9 mg/dL | ||
| Troponin‐T | Positive |
Alb, albmin; ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartatetransaminase; BUN, blood urea nitrogen; CPK, creatine phosphokinase; CPK‐MB, creatine phosphokinase myoglobin; Cre, Creatinine; CRP, c‐reactive protein; γGTP, γglutamyl transpeptidase; Hb, hemoglobin; Ht, hematocrit; LDH, lactate dehydrogenase; Plt, platelets; RBC, red blood cell; T‐Bil, total bilirubin; TP, total protein; WBC, white blood cell.
Figure 1.
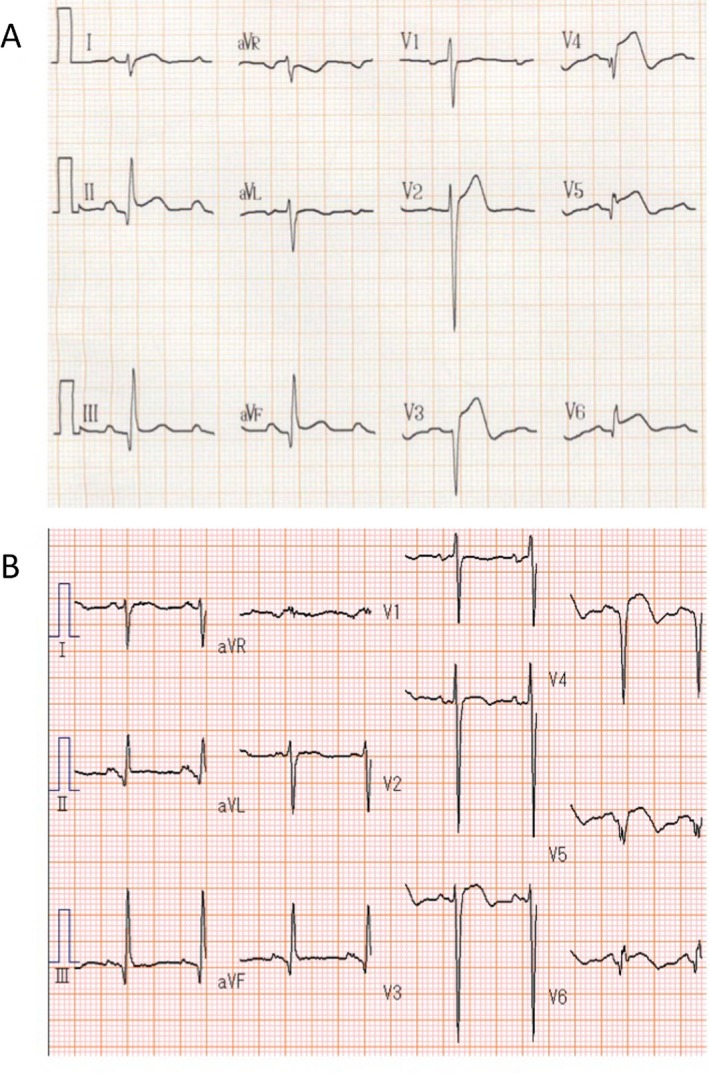
(A) The electrocardiogram recorded 3 h after arrival showed ST elevation in V2‐6, II, III and aVF. B) The electrocardiogram recorded on day 15 showed negative T wave in V2‐6.
Figure 2.
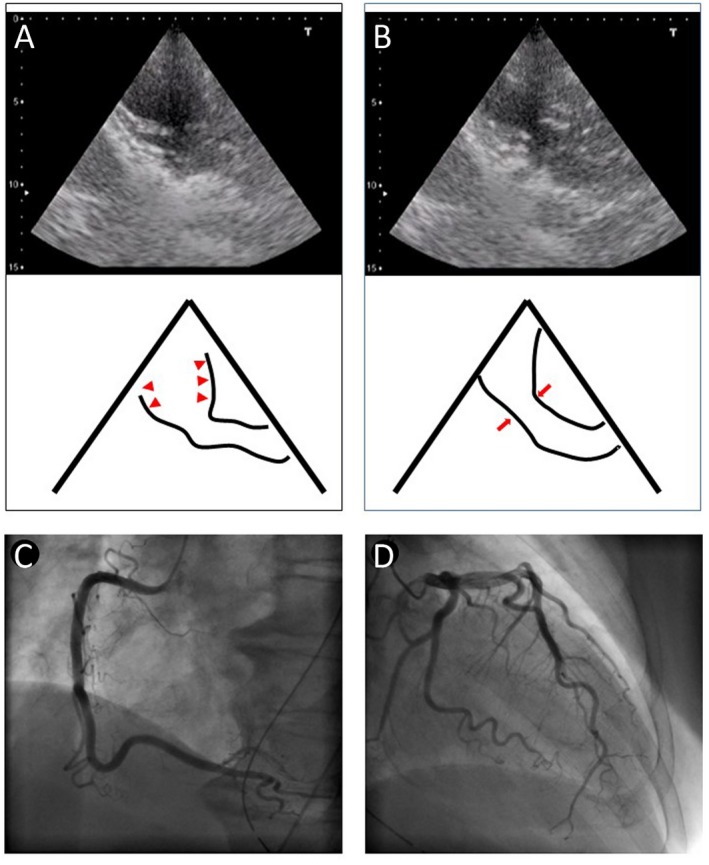
Echocardiography and angiography of the case. The echocardiogram on arrival displays (A) ventricular apical ballooning [arrowheads] with (B) basal hypercontraction [arrows]. Angiography revealed normal coronary arteries. (C) Right coronary angiography. (D) Left coronary angiography.
Despite fluid, vasoconstrictor, and inotrope administration, her cardiovascular status remained unstable. Due to her ECG findings of abnormal ST‐elevation and laboratory data, she underwent a cardiology consultation and subsequent coronary angiography to exclude the possibility of a complicating myocardial infarction. Angiography, however, indicated no coronary artery abnormalities (Fig. 2C, D) and the diagnosis of TCM complicating heatstroke was established.
After admission to the intensive care unit, her cardiovascular status gradually improved over a period of several hours. She was discharged from ICU and transferred to the psychiatric ward on day 36.
Discussion
This report presents a severe case of heatstroke complicated with TCM. Despite an extensive literature search, we could only find a single previous case report of heatstroke with TCM.3
Heatstroke‐associated myocardial damage has been well documented in the literature.1 Among various abnormal findings, ECG changes are common. Most of these involve sinus tachyarrhythmia, increased QT interval, or ST‐T changes.4 The frequency of ST‐T changes has been reported to be about 21.6%.4, 5, 6 Although the exact mechanism underlying ST‐T changes is unclear, it is reported to be associated with an increase in oxygen demand due to high core temperature, tachycardia, and high cardiac output.4 Elevated serum cardiac enzymes such as creatinine kinase (CK) or cardiac troponin 1 can also be found among severe heatstroke patients.7
Among reports of heatstroke associated myocardial damage, there is only one case report of heatstroke complicated with TCM, by Chen et al., involving a 39‐year‐old female.3 This patient with a rectal temperature of 43.1°C and ST elevation in V4 to 6 underwent coronary angiography, which indicated a normal coronary artery, while left ventriculography showed typical apical ballooning, which confirmed the diagnosis of TCM. Excessive release of catecholamine after emotional or physical stress has been focused on as the initial trigger for the abrupt development of TCM.8 Prolonged exposure to high ambient temperature resulting in an excessive high core temperature >40.5°C is a detrimental physical stress. An observational postmortem study of fatal heatstroke revealed elevated levels of plasma catecholamines,9 which strongly suggests that heatstroke and TCM share the same pathophysiology. As Chen et al. indicated, ST elevation in heatstroke victims may not necessarily be caused by atherosclerotic heart disease.3 However, since most heatstroke victims do not undergo coronary angiography, it is possible that some such victims complicated with TCM are not evaluated. Since fatal heatstroke can cause acute circulatory failure in its early stage, close monitoring of cardiac function is mandatory for survival outcome.
Although the present case was successfully managed by fluid administration, severe TCM cases sometimes require temporal intra‐aortic balloon pump usage to maintain internal blood pressure.8 Since TCM is a transient acute cardiomyopathy, nearly all patients survive if managed properly.8 However, the prognosis of heatstroke victims complicated with TCM is unclear. Our case and the previous report3 indicate that heatstroke patients with TCM can be managed as well as patients in whom TCM is induced by various other means.
Conclusion
This report indicates, along with the previous case report,3 that heatstroke and TCM can share the same pathophysiology of excessive catecholamine release and that TCM can be a possible cause of ST elevation. Since heatstroke can cause acute circulatory failure, close evaluation of hemodynamic status and myocardial damage is critical for survival.
Conflict of Interest
The authors have no conflicts of interests to disclose.
Supporting information
Supporting Information 1. Video of two‐dimensional echocardiography from the case.
References
- 1. Yeo TP. Heatstroke a comprehensive review. AACN Clin. Issues 2004; 15: 280–293. [DOI] [PubMed] [Google Scholar]
- 2. Zahger D, Moses A, Weiss AT. Evidence of prolonged myocardial dysfunction in heatstroke. Chest 1989; 95: 1089–1091. [DOI] [PubMed] [Google Scholar]
- 3. Chen W‐T, Lin C‐H, Hsieh M‐H et al Stress‐induced cardiomyopathy caused by heatstroke. Ann. Emerg. Med. 2012; 60: 63–66. [DOI] [PubMed] [Google Scholar]
- 4. Mimish L. Electrocardiographic findings in heatstroke and exhaustion: a study on Makkah pilgrims. J. Saudi Heart Assoc. 2012; 24: 35–39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Henderson A, Simon JW, Melia WM et al Heat illness. A report of 45 cases from Hong Kong. J. R. Army Med. Corps 1986; 132: 76–84. [DOI] [PubMed] [Google Scholar]
- 6. Akhtar MJ, Al‐Nozha M, Al‐Harthi S, Nouh MS. Electrocardiographic abnormalities in patients with heat illness. Chest 1993; 104: 411–414. [DOI] [PubMed] [Google Scholar]
- 7. Alzeer AH, El‐Hazmi MAF, Warsy AS. Serum enzymes in heatstroke: prognostic implication. Clin. Chem. 1997; 43: 1182–1187. [PubMed] [Google Scholar]
- 8. Pilgrim TM, Wyss TR. Takotsubo cardiomyopathy or transient left ventricular apical ballooning syndrome: a systematic review. Int. J. Cardiol. 2008; 124: 283–292. [DOI] [PubMed] [Google Scholar]
- 9. Yoshida C, Ishikawa T, Michiue T et al Postmortem biochemistry and immunohistochemistry of chromogranin a as a stress marker with special regard to fatal hypothermia and hyperthermia. Int. J. Legal Med. 2011; 125: 11–20. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supporting Information 1. Video of two‐dimensional echocardiography from the case.