

Abstract
Aim
Emergency department overcrowding is problematic. Some emergency departments have established a triage system to prevent overcrowding; however, effective management of a triage system requires knowledge of factors that influence emergency department attendance. Therefore, we investigated the effect of ambient temperature on emergency department attendance, as well as the types of patients that may have been affected.
Methods
Data on emergency department attendance at Shiga University of Medical Science Hospital (Otsu, Japan) were retrospectively collected from 1 April, 2007 to 31 March, 2010. Attendance was classified into eight categories based on a combination of symptoms (trauma or non‐trauma), transport (by ambulance or walk‐in), and severity (serious or non‐serious).
Results
A total of 7,755 patients (4,120 [53.1%] men and 3,635 [46.9%] women) attended the emergency department during the study period. Statistically significant seasonal differences were observed in emergency department attendance in walk‐in and non‐serious groups of both trauma and non‐trauma patients (P < 0.01), with the smallest differences occurring during winter. In a linear regression model, the mean ambient temperature had a positive correlation with emergency department attendance only in the walk‐in and non‐serious group of non‐trauma patients during the summer (y = 0.092 × [mean ambient temperature] − 0.565).
Conclusion
In the walk‐in and non‐serious group of non‐trauma patients, emergency department attendance significantly increased with the increase in mean ambient temperature during summer. In emergency department triage systems, it may be more effective to evaluate non‐trauma and walk‐in patients during summer, especially on hot days.
Keywords: Emergency department, non‐trauma, seasonal difference, temperature, walk‐in
Introduction
In many countries, the number of people attending the emergency department (ED) has been increasing.1, 2, 3 In Japan, approximately 4 million patients were transported to EDs by ambulance in 2000, and this number increased to nearly 5 million in 2010.4 Emergency department overcrowding causes a number of problems, including prolonged waiting times, increased patient suffering, unpleasant therapeutic environments, and, in some cases, can result in poor clinical outcomes.5 Solutions to alleviate ED overcrowding are complex, expensive, and currently being debated.6
The universal healthcare system in Japan is a free‐access system without gatekeepers that allows people to be examined and treated at the medical institutions of their choice at any time, regardless of their symptoms. Moreover, anyone can use an ambulance free of charge simply by making a call. Therefore, patients without a severe illness or injury are able to attend the ED whenever they want to see a doctor.
A triage system is vital for the effective management of the ED. A large number of patients attending an ED believe they have an emergency or urgent condition, but nearly half of them have non‐urgent conditions based on triage classifications.7 For efficient operation of the triage system, it is important to both determine what factors influence ED attendance and predict demand for ED services. Previous studies have focused on the effects of weather on human health, suggesting a relationship between the ambient temperature and mortality,8, 9, 10, 11, 12 myocardial infarction,13, 14 stroke,15, 16, 17 and trauma.18, 19 The effects of ambient temperature on ED attendance were also investigated, but the results were inconsistent.20, 21, 22
Therefore, we investigated the correlation between the ambient temperature and ED crowding, as well as which types of patients attending the ED were influenced by the ambient temperature.
Methods
Data on ED attendance at Shiga University of Medical Science Hospital (Otsu, Japan) were retrospectively collected from 1 April, 2007 to 31 March, 2010. The Shiga University of Medical Science Hospital ED receives surgical and psychiatric emergencies, as well as those in internal medicine involving patients aged 16 years or over (pediatricians consult with internal medicine patients younger than 16 years of age). The ED also provides 24‐h ambulance emergency services and out‐of‐hours services for walk‐ins, Monday to Friday from 5:00 pm to 8:30 am, as well as on weekends and holidays.
Data collection and processing
All patient data were obtained from records in our hospital. Emergency department attendance was classified into eight categories based on a combination of symptoms (trauma or non‐trauma), transport (by ambulance or walk‐in), and severity (serious or non‐serious).
For transport, patients who were transferred from another hospital or who happened to have been injured in our hospital were classified as “other visit type”. For severity, the patients who were admitted, who died, or who were transferred to another hospital were classified as serious cases. Patients who were discharged from the ED were classified as non‐serious cases. Only 35 patients attended the ED by “other visit type” during the study period; these patients were excluded from analysis because they were far fewer in number than patients who attended by ambulance or walk‐in.
Weather data
Our hospital is located in Shiga Prefecture, which is in central Japan. Most regions in the country have a temperate climate with four distinct seasons: spring (March–May), summer (June–August), autumn (September–November), and winter (December–February). Each of these seasons has distinct characteristics and was therefore examined separately.
The mean ambient temperatures for the period from 1 April, 2007 to 31 March, 2010 were obtained from the Japan Meteorological Agency, which reported observations made at the meteorological station nearest to the hospital.
Data exclusion
Temperature data from 21 January, 2010 to 28 January, 2010 were excluded because the device for collecting meteorological data was being upgraded and was therefore inoperable during this period.
Data analysis
The χ2‐test was used to compare proportions between the groups in seasonal distribution of ED attendance. Linear regression analysis was used to evaluate the associations between the mean ambient temperature and the daily ED attendance in each group. Regression coefficients and 95% confidence intervals were estimated for mean ambient temperature‐associated differences in daily ED attendance. Statistical analysis was carried out with IBM spss Statistics 20.0 for Windows (IBM Japan, Tokyo, Japan). All tests were two‐tailed, and P‐values < 0.05 were considered statistically significant.
Results
During the 1,088‐day study period, a total of 7,755 patients (4,120 [53%] men and 3,635 [47%] women) attended the ED. The mean ages (± standard deviation) for the men and women were 45.0 ± 23.7 years and 47.0 ± 23.8 years, respectively. The number of days, the mean ambient temperature, and the number of patients attending the ED are summarized in Table 1.
Table 1.
Number of days, mean ambient temperature, and number of patients attending the emergency department of Shiga University of Medical Science Hospital (Otsu, Japan) by season, 1 April, 2007 to 31 March, 2010
| All seasons | Spring | Summer | Autumn | Winter | |
|---|---|---|---|---|---|
| Number of days | 1,088 | 276 | 276 | 273 | 263 |
| Temperature (°C) | 15.4 ± 8.3 | 13.2 ± 4.8 | 25.1 ± 3.0 | 17.5 ± 5.6 | 5.4 ± 2.7 |
| Number of patients | 7,755 | 1,922 | 2,048 | 1,993 | 1,792 |
Temperature data are expressed as mean ± standard deviation. Autumn, September–November; Spring, March–May; Summer, June–August; Winter, December–February.
Number of patients attending the ED
Figure 1 shows the seasonal differences in the number of patients in each group that attended the ED. In the walk‐in and non‐serious groups of both trauma and non‐trauma patients, statistically significant seasonal differences were apparent in ED attendance (χ2 = 16.9, 17.6, Df = 3; P < 0.01). The smallest differences were seen during winter. No statistically significant seasonal differences were found in ED attendance for the walk‐in and serious groups (χ2 = 5.06, 1.31, Df = 3; P = 0.168, 0.726), for the ambulance and non‐serious groups (χ2 = 3.72, 5.49, Df = 3; P = 0.293, 0.139), or for the ambulance and serious groups (χ2 = 1.77, 3.99, Df = 3; P = 0.621, 0.263).
Figure 1.
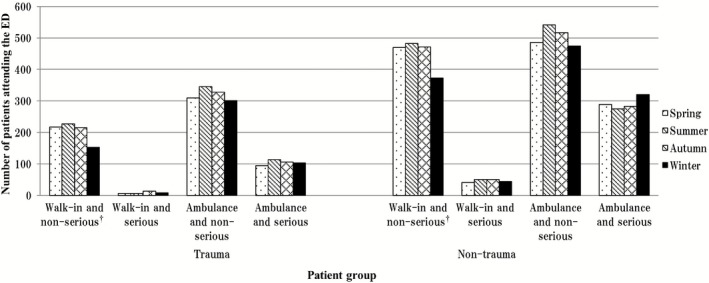
Seasonal differences in attendance at the emergency department (ED) of Shiga University of Medical Science Hospital (Otsu, Japan) from 1 April, 2007 to 31 March, 2010, according to patient group. †Statistically significant seasonal differences were observed in walk‐in and non‐serious groups of both trauma and non‐trauma patients (χ2 = 16.9, 17.6, Df = 3; P < 0.01).
Effect of mean ambient temperature
To study the effect of the mean ambient temperature in each group, the daily ED attendance was used as the dependent variable in the linear regression model. Table 2 shows the coefficients and the corresponding 95% confidence intervals of each group in every season. The mean ambient temperature had a significant positive correlation with the daily ED attendance only for the walk‐in and non‐serious group of non‐trauma patients during the summer (Table 2). The following formula was established:
Table 2.
Effects of mean ambient temperature on attendance of each patient group at the emergency department of Shiga University of Medical Science Hospital (Otsu, Japan) by season, 1 April, 2007 to 31 March, 2010
| Trauma patients | ||||||
|---|---|---|---|---|---|---|
| Group | Total number | Coefficient | 95% CI | P‐value | ||
| Spring | Walk‐in | Non‐serious | 217 | 0.010 | −0.013 to 0.032 | 0.393 |
| Serious | 6 | 0.001 | −0.003 to 0.004 | 0.675 | ||
| Ambulance | Non‐serious | 310 | 0.019 | −0.010 to 0.049 | 0.194 | |
| Serious | 95 | 0.000 | −0.140 to 0.014 | 0.980 | ||
| Summer | Walk‐in | Non‐serious | 227 | −0.003 | −0.045 to 0.038 | 0.883 |
| Serious | 6 | −0.005 | −0.011 to 0.001 | 0.095 | ||
| Ambulance | Non‐serious | 346 | 0.016 | −0.034 to 0.066 | 0.535 | |
| Serious | 114 | −0.006 | −0.031 to 0.020 | 0.664 | ||
| Autumn | Walk‐in | Non‐serious | 216 | −0.006 | −0.028 to 0.016 | 0.598 |
| Serious | 14 | −0.001 | −0.005 to 0.004 | 0.830 | ||
| Ambulance | Non‐serious | 328 | −0.017 | −0.042 to 0.008 | 0.180 | |
| Serious | 106 | −0.005 | −0.019 to 0.009 | 0.449 | ||
| Winter | Walk‐in | Non‐serious | 153 | −0.027 | −0.063 to 0.009 | 0.146 |
| Serious | 8 | 0.002 | −0.006 to 0.010 | 0.591 | ||
| Ambulance | Non‐serious | 301 | 0.006 | −0.047 to 0.059 | 0.826 | |
| Serious | 103 | 0.012 | −0.021 to 0.044 | 0.473 | ||
| Non‐trauma patients | ||||||
|---|---|---|---|---|---|---|
| Group | Total number | Coefficient | 95% CI | P‐value | ||
| Spring | Walk‐in | Non‐serious | 470 | 0.007 | −0.032 to 0.046 | 0.732 |
| Serious | 41 | −0.003 | −0.012 to 0.007 | 0.539 | ||
| Ambulance | Non‐serious | 486 | −0.004 | −0.039 to 0.030 | 0.800 | |
| Serious | 289 | −0.011 | −0.037 to 0.015 | 0.405 | ||
| Summer | Walk‐in | Non‐serious | 483 | 0.092 | 0.034 to 0.151 | 0.002* |
| Serious | 50 | 0.004 | −0.013 to 0.022 | 0.616 | ||
| Ambulance | Non‐serious | 542 | 0.030 | −0.024 to 0.084 | 0.270 | |
| Serious | 275 | 0.034 | −0.006 to 0.073 | 0.092 | ||
| Autumn | Walk‐in | Non‐serious | 472 | −0.027 | −0.059 to 0.005 | 0.096 |
| Serious | 50 | 0.009 | 0.000 to 0.018 | 0.058 | ||
| Ambulance | Non‐serious | 517 | 0.005 | −0.027 to 0.036 | 0.776 | |
| Serious | 283 | −0.019 | −0.043 to 0.004 | 0.108 | ||
| Winter | Walk‐in | Non‐serious | 373 | 0.023 | −0.039 to 0.085 | 0.470 |
| Serious | 44 | 0.013 | −0.007 to 0.032 | 0.195 | ||
| Ambulance | Non‐serious | 475 | −0.008 | −0.074 to 0.058 | 0.814 | |
| Serious | 320 | −0.031 | −0.084 to 0.021 | 0.243 | ||
The dependent variable was the daily number of patients attending the emergency department, and the independent variable was the mean ambient temperature. All P‐values were two‐sided. *P < 0.05 determined statistical significance. Autumn, September–November; Spring, March–May; Summer, June–August; Winter, December–February. CI, confidence interval.
Figure 2 shows the mean daily ED attendance for the walk‐in and non‐serious group of non‐trauma patients according to the mean ambient temperature in intervals of 3°C during summer.
Figure 2.
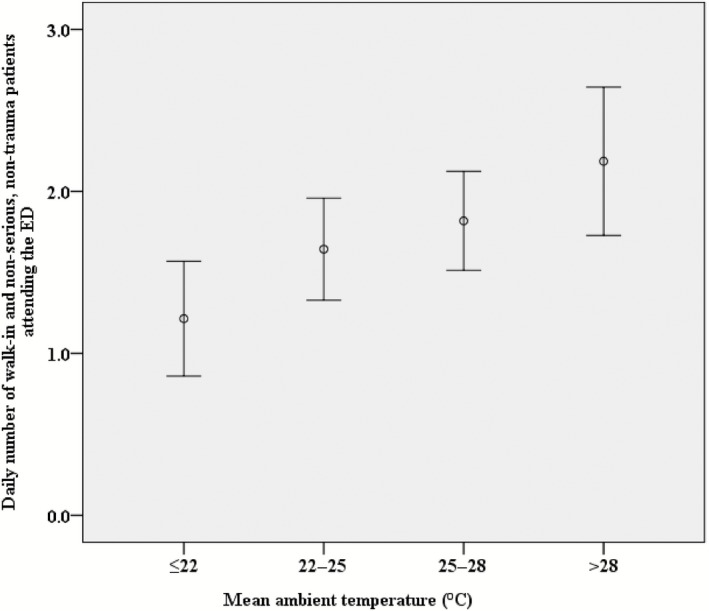
Daily number of walk‐in and non‐serious non‐trauma patients attending the emergency department (ED) of Shiga University of Medical Science Hospital (Otsu, Japan) from 1 April, 2007 to 31 March, 2010, according to daily mean ambient temperature during summer. The ranges of the mean ambient temperatures were ≤22°C, 22–25°C, 25–28°C, and >28°C, and the numbers of days at these temperatures during summer were 45, 84, 92, and 55 days, respectively. Bars represent 95% confidence intervals.
Exposure to higher ambient temperatures during summer increases the likelihood of heat‐related illnesses. In our study, the number of patients suffering from heat‐related illnesses in the walk‐in and non‐serious group of non‐trauma patients during summer was only 5 (1.0% [5/483]). To clarify whether heat‐related illnesses influenced ED attendance or not, we further analyzed the number of patients excluded from the patients suffering from heat‐related illnesses in the walk‐in and non‐serious group of non‐trauma patients during the summer. The resulting formula was:
This result suggested that heat‐related illnesses had no influence on ED attendance in the walk‐in and non‐serious group of non‐trauma patients during the summer.
No statistically significant correlations were observed in other groups or seasons (Table 2).
Discussion
Inappropriate use of ED services is a common problem in many countries, with prevalence varying from 20% to 40%.23, 24 Those inappropriately using the ED were reported to have better health, to be less likely to arrive by ambulance, and to be less often admitted to hospital from the ED than those appropriately using the ED.25
In our study, no seasonal differences were seen in the number of patients attending the ED in either the walk‐in and serious groups, the ambulance and non‐serious groups or the ambulance and serious groups, whereas the number of patients attending the ED in the walk‐in and non‐serious groups of both non‐trauma and trauma patients was the smallest during winter (Fig. 1). Daily physical activity was reported to increase with the maximal temperature up to 84°F (28.9°C) in Tennessee, USA, which has a temperate climate.26 Regarding trauma patients, low physical activity seemed to decrease the number of non‐serious patients during the winter. This may be one reason why ED attendance at our hospital by the walk‐in and non‐serious group of trauma patients was the lowest during winter. On the contrary, regarding non‐trauma patients, low physical activity was thought to be the reason why non‐serious patients were less likely to visit the hospital. This might explain the decrease in the number of walk‐ins and non‐serious, non‐trauma patients that attended the ED at our hospital during the winter. Regarding non‐trauma patients, we found that the mean ambient temperature had no correlation with ED attendance in either the walk‐in and serious group, the ambulance and non‐serious group, or the ambulance and serious group (Table 2). These results suggest that the mean ambient temperature had no correlation with disease prevalence in our hospital. However, the mean ambient temperature did have a positive correlation with the daily number of patients attending the ED in the walk‐in and non‐serious group of non‐trauma patients only during the summer (Fig. 2). Tai et al. found that, in Taiwan, which is located in a subtropical region, more patients with less severe illnesses or injuries attended the ED on warm days.20 Taken together, these findings suggest that walk‐in, non‐serious, non‐trauma patients might use the ED inappropriately.
Because of ED overcrowding, prioritizing patients based on acuity and risk has become increasingly important.27 Consequently, some EDs have established a triage system to assign relatively scarce resources to unlimited medical needs.28 Our study showed that ED attendance in the walk‐in and non‐serious group of non‐trauma patients increased with increases in the mean ambient temperature during summer. We suggest the following methods as effective ways of utilizing scarce human resources in the ED: adjusting the work schedules of medical staff; requesting support from staff in other departments (e.g., general internists suitable for consulting with internal medicine for walk‐in patients); expanding the waiting area for walk‐in patients and/or establishing a triage system to evaluate walk‐in and non‐trauma patients during the summer, especially on hot days. These methods will allow the staff in the ED to concentrate their attention on serious patients, and could result in good clinical outcomes. Further research in different geographic areas and hospitals is recommended as the characteristics of ED attendance vary between hospitals. Information specific to each hospital would be useful in planning the allocation of human resources and in reviewing work plans, thereby alleviating ED overcrowding.
Limitations
Our study had several limitations. First, we chose the mean ambient temperature as the tested weather variable. Other weather variables not included in this study, such as typhoons or the rainy season, might have confounded our results. Second, the daily numbers of patients in each group were small. In our study, the average daily number of patients in the walk‐in and non‐serious group of non‐trauma patients during the summer was 1.75. Furthermore, a 1°C change in the mean ambient temperature was associated with 0.092 additional patient visits. Thus, ED attendance in this group increased 5.3% with each 1°C increase in ambient temperature. To transcend this limitation, further research is recommended in our hospital during a longer period, or in another hospital where its daily number of patients attending the ED is much larger. Third, our ED did not accept all patients arriving by ambulance; during the study period, the number of refusals was 75 (6.0% [75/1255]) in spring, 98 (7.1% [98/1375] in summer, 72 (5.5% [72/1306]) in autumn, and 78 (6.1% [78/1277]) in winter. Finally, we did not classify patients by disease type because this study aimed to investigate the correlation between a weather factor and ED crowding.
Conclusions
We found that, among non‐trauma cases, ED attendance by walk‐in and non‐serious patients significantly increased with increases in the mean ambient temperature during the summer. In ED triage systems, it may be more effective to evaluate non‐trauma and walk‐in patients during the summer, especially on hot days. This may facilitate more effective distribution of scarce medical resources.
Conflict of Interest
None.
References
- 1. Tang N, Stein J, Hsia RY, Maselli JH, Gonzales R. Trends and characteristics of US emergency department visits, 1997–2007. JAMA 2010; 304: 664–670. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Santos‐Eggimann B. Increasing use of the emergency department in a Swiss hospital: Observational study based on measures of the severity of cases. BMJ 2002; 324: 1186–1187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. McCaig LF, Burt CW. National Hospital Ambulatory Medical Care Survey: 2002 emergency department summary. Adv. Data 2004; 18: 1–34. [PubMed] [Google Scholar]
- 4. Trends in the Number of Patients Transported by Ambulance. Fire and Disaster Management Agency of the Ministry of Internal Affairs and Communications of Japan, Tokyo: 2010. [cited 20 Feb 2014]. Available from: http://www.fdma.go.jp/html/hakusho/h23/h23/html/2‐2‐4‐1_1.html. (In Japanese.) [Google Scholar]
- 5. Derlet RW, Richards JR. Overcrowding in the nation's emergency departments: Complex causes and disturbing effects. Ann. Emerg. Med. 2000; 35: 63–68. [DOI] [PubMed] [Google Scholar]
- 6. Brillman J, Mathers‐Dunbar L, Graff L et al Management of observation units. American College of Emergency Physicians. Ann. Emerg. Med. 1995; 25: 823–830. [DOI] [PubMed] [Google Scholar]
- 7. Young GP, Wagner MB, Kellermann AL, Ellis J, Bouley D. Ambulatory visits to hospital emergency departments. Patterns and reasons for use. 24 Hours in the ED Study Group. JAMA 1996; 276: 460–465. [DOI] [PubMed] [Google Scholar]
- 8. Iñiguez C, Ballester F, Ferrandiz J et al Relation between temperature and mortality in thirteen Spanish cities. Int. J. Environ. Res. Public Health 2010; 7: 3196–3210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Kvaløy JT, Skogvoll E. Modelling seasonal and weather dependency of cardiac arrests using the covariate order method. Stat. Med. 2007; 26: 3315–3329. [DOI] [PubMed] [Google Scholar]
- 10. Analitis A, Katsouyanni K, Biggeri A et al Effects for cold weather on mortality: Results from 15 European cities within the PHEWE project. Am. J. Epidemiol. 2008; 168: 1397–1408. [DOI] [PubMed] [Google Scholar]
- 11. Ng CF, Ueda K, Takeuchi A et al Sociogeographic variation in the effects of heat and cold on daily mortality in Japan. J. Epidemiol. 2014; 24: 15–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Curriero FC, Heiner KS, Samet JM, Zeger SL, Strug L, Patz JA. Temperature and mortality in 11 cities of the Eastern United States. Am. J. Epidemiol. 2002; 155: 80–87. [DOI] [PubMed] [Google Scholar]
- 13. Hirasawa K, Shibata J, Yamamura K. Clinical and statistical evaluation of the occurrence of acute myocardial infarction in the cold inland area of Hokkaido. Jpn Circ. J. 1989; 53: 677–685. [DOI] [PubMed] [Google Scholar]
- 14. Bhaskaran K, Hajat S, Haines A, Herrett E, Wilkinson P, Smeeth L. Effects of ambient temperature on the incidence of myocardial infarction. Heart 2009; 95: 1760–1769. [DOI] [PubMed] [Google Scholar]
- 15. Low RB, Bielory L, Qureshi AI, Dunn V, Stuhlmiller DF, Dickey DA. The relation of stroke admissions to recent weather, airborne allergens, air pollution, seasons, upper respiratory infections, and asthma incidence, September 11, 2001, and day of the week. Stroke 2006; 37: 951–957. [DOI] [PubMed] [Google Scholar]
- 16. Chang CL, Shipley M, Marmot M, Poulter N. Lower ambient temperature was associated with an increased risk of hospitalization for stroke and acute myocardial infarction in young women. J. Clin. Epidemiol. 2004; 57: 749–757. [DOI] [PubMed] [Google Scholar]
- 17. Ohshige K, Hori Y, Tochikubo O, Sugiyama M. Influence of weather on emergency transport events coded as stroke: Population‐based study in Japan. Int. J. Biometeorol. 2006; 50: 305–311. [DOI] [PubMed] [Google Scholar]
- 18. Atherton WG, Harper WM, Abrams KR. A year's trauma admissions and the effect of the weather. Injury 2005; 36: 40–46. [DOI] [PubMed] [Google Scholar]
- 19. Parsons N, Odumenya M, Edwards A, Lecky F, Pattison G. Modelling the effects of the weather on admissions to UK trauma units: A cross‐sectional study. Emerg. Med. J. 2011; 28: 851–855. [DOI] [PubMed] [Google Scholar]
- 20. Tai CC, Lee CC, Shih CL, Chen SC. Effects of ambient temperature on volume, specialty composition and triage levels of emergency department visits. Emerg. Med. J. 2007; 24: 641–644. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Alessandrini E, Zauli Sajani S, Scotto F, Miglio R, Marchesi S, Lauriola P. Emergency ambulance dispatches and apparent temperature: A time series analysis in Emilia‐Romagna, Italy. Environ. Res. 2011; 111: 1192–1200. [DOI] [PubMed] [Google Scholar]
- 22. Diehl AK, Morris MD, Mannis SA. Use of calendar and weather data to predict walk‐in attendance. South. Med. J. 1981; 74: 709–712. [DOI] [PubMed] [Google Scholar]
- 23. Dale J, Green J, Reid F, Glucksman E. Primary care in the accident and emergency department: I. Prospective identification of patients. BMJ 1995; 311: 423–426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Carret ML, Fassa AC, Domingues MR. Inappropriate use of emergency services: A systematic review of prevalence and associated factors. Cad. Saude Publica 2009; 25: 7–28. [DOI] [PubMed] [Google Scholar]
- 25. Afilalo J, Marinovich A, Afilalo M et al Nonurgent emergency department patient characteristics and barriers to primary care. Acad. Emerg. Med. 2004; 11: 1302–1310. [DOI] [PubMed] [Google Scholar]
- 26. Wolff D, Fitzhugh EC. The relationships between weather‐related factors and daily outdoor physical activity counts on an urban greenway. Int. J. Environ. Res. Public Health 2011; 8: 579–589. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Bullard MJ, Unger B, Spence J, Grafstein E, the CTAS National Working Group . Revisions to the Canadian Emergency Department Triage and Acuity Scale (CTAS) adult guidelines. CJEM 2008; 10: 136–151. [DOI] [PubMed] [Google Scholar]
- 28. FitzGerald G, Jelinek GA, Scott D, Gerdtz MF. Emergency department triage revisited. Emerg. Med. J. 2010; 27: 86–92. [DOI] [PubMed] [Google Scholar]