

Abstract
Objective:
Saudi demographic composition has changed because of increased life expectancy and decreased fertility rates. Little data are available about health conditions among older adults in Saudi Arabia, who are expected to represent 20% of the population by 2050. The study aim was to assess the prevalence and risk factors for chronic conditions among older Saudi men.
Methods:
The sample pertained to 400 men (age ≥55 years) from Buraidah, Al-Qassim. Research assistants recruited participants in all the mosques from the randomly selected neighborhoods (16 of 95). They administered a structured questionnaire that assessed self-reported disease history (heart disease, hypertension, diabetes, asthma, gastric/peptic ulcer, and cancer), and medication use; participants’ height, weight, blood pressure, and random blood glucose (glucometer) were measured. Multinomial logistic regressions were employed to assess correlates of number of chronic diseases.
Results:
The mean and standard deviation for age and body mass index (BMI) were 63.0 ± 7.5 years and 28.9 ± 4.8 (kg/m2), respectively. 78% (77.8%) were overweight or obese, 35.0% were employed, 54.5% walked daily, 9.3% were current smokers, and 85.0% belonged to the middle class. The prevalence of hypertension, diabetes, heart disease, asthma, ulcer, and cancer were: 71.3% 27.3%, 16.4%, 9.7%, 8.9%, and 2.0%, respectively. Of the participants, 31.0% had one, 34.5% had two or more, and 34.5% did not have any chronic diseases. The likelihood of chronic diseases increased with increased age, higher BMI, and current smoking.
Conclusion:
The chronic disease prevalence among the Saudi elderly men is substantial.
Keywords: Chronic disease, elderly, Saudi Arabia
Introduction
Saudi Arabia has been experiencing a slow but steady change in its demography with a larger proportion of elderly people (i.e. 65+ years) in the distribution, thanks to a host of factors such as decreasing fertility and infant-mortality rates as well as the availability of free, modern healthcare for its citizens. Elderly people were only 3% of the Saudi population in 2010; in contrast, they will be nearly 20% by 2050.1
Saudi Arabia is a leading nation in the world with a high prevalence of chronic diseases and their associated risk factors.2 For example, one in four adult is either obese or diabetic.3 The population prevalence of hypertension is 25% and that of coronary heart disease is nearly 6%.4 Both physical activity level and consumption of fruits and vegetables in the population are very low and the proportion of smokers is substantial.5-7
It is expected that the prevalence of chronic diseases are even higher among the Saudi elderly people; but the available data for this group come from studies that sampled the adult population (i.e., 18+) and reported age-stratified disease outcomes.8-10 There are hardly any studies that have specifically targeted the elderly population. Without such studies, many issues important to older adults have been overlooked such as quality of life (i.e., physical functioning or mental health), common mental disorders (e.g., depression), and conditions specific to older age (e.g., memory loss).
To meet this knowledge gap, a survey was conducted in the Al-Qassim region among its elderly members with a comprehensive assessment of their chronic diseases, lifestyle, quality of life, depression, and memory loss. This report, first in a series, contained only the disease prevalence data and the correlates of these conditions.
Methods
Sample
This cross-sectional study was conducted in Buraidah, the largest city in the Al-Qassim region of Saudi Arabia, among 400 Saudi men. The inclusion criteria were: (1) Age at least 55 or older, (2) Saudi by citizenship, and (3) residents of Buraidah. The age inclusion for this study was reduced to 55 years to obtain an adequate sample with ease, since the percentage of elderly (≥65 years) in Saudi Arabia is relatively low (3.2%),
The research Ethics Committee in the College of Medicine at Sulaiman Al-Rajhi Colleges approved the study in 2015; the data were collected between December 2015 and February 2016.
Sample size
According to the Governmental Statistics, the total male population of Al-Qassim region of Saudi Arabia in 2016 was 501,831, of which 9.5% or approximately 50,000 were aged 55 years and older.11 Therefore, the minimum sample size for this study was 381 men (95% confidence and with a 5% margin of error), which was exceeded by enrolling 400 men.
Sampling strategy
A multi-stage semi-random sampling technique was used to obtain the sample. The detailed area map of Buraidah city was used to list the neighborhoods (total 96 neighborhoods) and 20 were selected randomly from it. All mosques in the selected neighborhoods were mapped and listed. The recruitment goal was three eligible persons per mosque. Therefore, 133 mosques were needed to obtain the adequate sample size. However, a 20% extra mosques were selected (total 160) to ensure that the study had the required sample.
Research assistants described the study objectives and procedures to the prayer attendee, and invited the eligible participant to join. Those who showed interest were given the informed consent form, which they read and signed to be enrolled into the study.
Assessment
The assessment took place in a quiet corner in the mosque after the prayer. Participants were interviewed with standardized questionnaires to obtain information on demography, lifestyle, quality of life, and chronic conditions. Participants were asked whether they have been told by their physician in the past that they had any of the following chronic conditions: Hypertension, diabetes, heart disease, asthma, peptic ulcer, or cancer; in addition, they were asked about the duration of the disease and medication use if they answered positively for any conditions. After the interview, they were assessed for physical measurement (i.e., height, weight, and blood pressure) and blood glucose as per standard protocols. Two blood pressure readings were taken with a digital sphygmomanometer and the lowest value was recorded. Random blood glucose was measured with a glucometer (Accu-Chek Active).12
Outcome
Heart disease, asthma, and peptic ulcer were entirely self-reported. Hypertension and diabetes status were determined with the use of both measurement and self-report data. Hypertension was defined as systolic blood pressure of ≥140 or diastolic ≥90 mm Hg or use of anti-hypertensive medication. Diabetes was defined as blood glucose ≥200 mg/dl or use of anti-diabetic medication. Number of chronic conditions was derived from the summation of conditions and was categorized as none, one, or two or more conditions.
Covariates
Body mass index (BMI) was calculated as kg/m2 and was divided into <25, 25-29.9, and ≥30. The other variables were age (<60, 60-69, ≥70), marital status (currently married vs. not), employment status (currently employed vs. not), daily walking (yes, no), eating at restaurants (mostly at home, both home, and restaurant), cigarette smoking (never, former, and current), and economic status (poor, lower middle class, upper middle class, and rich).
Analysis
Data analysis was carried out with SPSS (version 22); all tests were two sided with an alpha level of 0.05. Analysis began with the generation of descriptive statistics of variables. Mean and standard deviation for continuous and frequency for categorical variables were reported. The prevalence of individual disease (i.e., hypertension, diabetes, heart disease, asthma, peptic ulcer, and cancer) as well as the total number of diseases (none, one, two, or more) were reported. The distribution of total number of diseases across age and BMI categories were calculated and compared.
Multinomial logistic regression was employed to model the associations between risk factors and participants having either single disease or two or more diseases (reference category: participants with no disease). The model building began with unadjusted analyses; age, BMI, employment status, daily walk, eating habit, smoking status, and socioeconomic status were assessed as risk factors. For eating habit, only 6 participants responded to “mostly restaurant food” option; therefore, it was merged with “home and restaurant food” group. Similarly, socioeconomic status was made binary by collapsing “poor” with “lower middle class” and “rich” with “upper middle class.”
Afterward, these variables were included in the adjusted analyses. A backward elimination process was employed for the selection of the most parsimonious model. The odds ratio and the associated 95% confidence interval for each of the comparison categories of the included variables in the final model were estimated.
Results
The participants’ mean age was 63 years (standard deviation = 7.5 years) and mean BMI was 28.9 kg/m2 (standard deviation = 4.8). Most of them were overweight or obese (77.8%). Almost all of them (98.0%) were married and 35.0% were employed at the time of the interview. A large majority of them (76.5%) never smoked cigarettes and mostly ate home-cooked food (65.0%). A little over half of them (54.5%) reported walking daily as leisure-time activity. Most of them (85.0%) reported that they belonged to the middle class, and a minority categorized them as poor (8.8%) or rich (6.3%) (Table 1).
Table 1.
Demographic characteristics of a sample of older Saudi men in Al-Qassim Saudi Arabia (n=400)

71% (71.3%) had hypertension and 27.3% had diabetes; 16.4% percent had heart disease, 9.7% had asthma, 8.9% had peptic ulcer, and 2.0% had cancer (Figure 1). A total of 31.0% (n = 124) had one, 34.5% (n = 138) had two or more, and 34.5% (n = 138) did not have any chronic diseases (data not shown). The frequency of having multiple chronic conditions increased with age and BMI. For example, only 22.5% of those who were <60 years old had multiple conditions, the corresponding frequency for the 60-69 and ≥70 years age groups were 34.8% and 57.3%, respectively. Likewise, the frequency of multiple chronic conditions among the normal, overweight or obese participants was 22.5%, 37.9%, and 38.0%, respectively (Figure 2).
Figure 1.
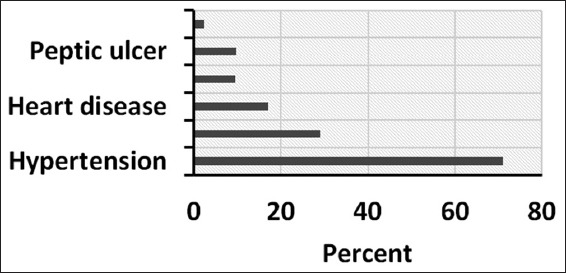
Prevalence of chronic conditions among older Saudi men (age ≥55 years) in Al-Qassim Saudi Arabia (n = 400)
Figure 2.
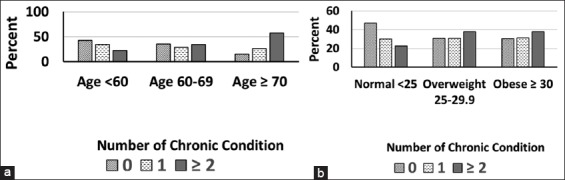
Univariate relationships between covariates and number of chronic conditions among older Saudi men (age ≥55 years) in Al-Qassim Saudi Arabia (n = 400): (a) Stratified by age and (b) stratified by body mass index categories
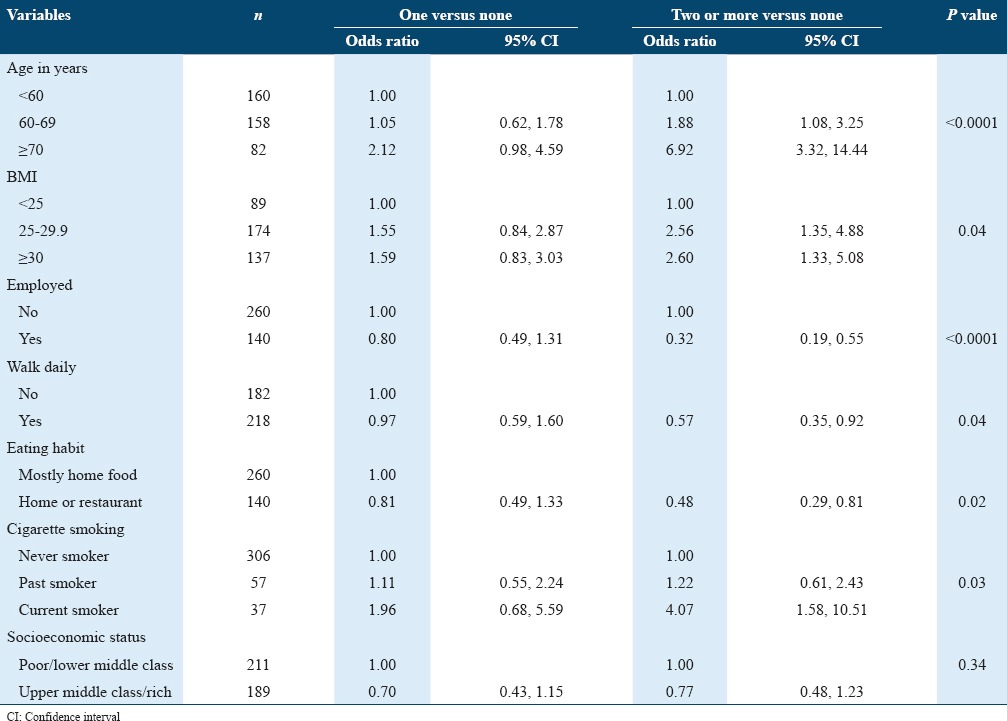
Unadjusted multinomial regression showed that an increased age, a higher BMI, and a smoking history (either current or past) were more likely to be associated with number of chronic conditions. On the other hand, being employed, having a daily walk, a mixed eating habit (i.e., both home and restaurant food), and a higher socioeconomic status were less likely to be associated with number of chronic conditions. All risk factors exhibited significant associations with the outcome except for socioeconomic status (Table 2).
Table 2.
Unadjusted multinomial logistic models of number of chronic conditions among older Saudi men (age ≥55 years) in Al-Qassim Saudi Arabia (n=400)
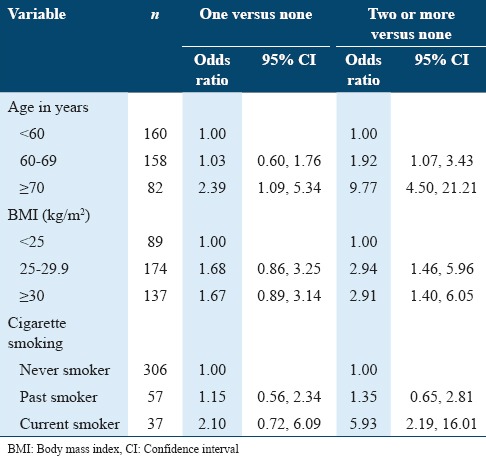
The backward selection method retained only three risk factors (i.e. age, BMI, and smoking habit) in the adjusted multinomial regression. Employment status, eating habit, and daily walking lost their significance in the adjusted models and thus were excluded by the selection method. The final adjusted models showed that the odds of having one chronic condition was similar for the 60-69 years and 2.39 times higher for the ≥70 years when compared against <60 years of age; and the odds of multiple conditions were 1.92 times higher for the 60-69 years age and 9.77 times higher for ≥70 years (reference group ≤60 years of age). The odds of having one chronic condition was 1.67 times higher (statistically not significant) for the obese compared to normal weight. The odds of having multiple conditions was 2.94 times higher for the overweight and 2.91 times higher for the obese (reference group = normal weight). The odds of having one chronic condition were 2.10 times higher and the odds of having multiple conditions were 5.93 times higher for the current smokers compared to the non-smokers (Table 3).
Table 3.
Adjusted multinomial logistic models of number of chronic conditions among older Saudi men (age ≥55 years) in Al-Qassim Saudi Arabia (n=400)
Discussion
This study showed that majority of the Saudi elderly men had at least one chronic disease. The number of chronic diseases increased across the increasing age and BMI categories. Cigarette smoking was significantly correlated with the number of chronic diseases, in addition to age and BMI. According to the Saudi Health Interview Survey (SHIS) – A national multistage survey of 10,375 individuals aged 15 years or older – the prevalence of hypertension and diabetes among those aged 65 or older were 65% and 50%, respectively.8-10 The hypertension prevalence of this study was comparable to that of SHIS (71.3% vs. 65%) but the diabetes prevalence was lower (27.3% vs. 50%). The reliance on random blood glucose only, as opposed to both fasting and random glucose, for the determination of diabetes in this study may explain the differences in prevalence.
The prevalence of heart diseases (16.4%) and asthma (9.7%) reported in this study were also comparable to those from other studies. The results from the Riyadh Cohort Study showed that the prevalence of coronary heart disease was 16% in 2011 among men aged over 60.13 Similarly, the SHISH 2013 data indicated the prevalence of asthma in men over the age of 55 to be around 7%.14 There was no available data on peptic ulcer prevalence in elderly men in Saudi Arabia. The prevalence found in this study (8.9%) closely matched the lifetime prevalence of peptic ulcer (10%) reported in the US study.15
Dietary intake showed that one-third of participants substituted their diet with restaurant/fast-food regularly. This finding is not directly comparable with the available data on diet because of the differences in the type of measurement. However, national data from Saudi Arabia suggested that sub-optimal nutritional intake is prevalent in all age groups and less than 6% of adults met the daily dietary recommendations.16 Physical inactivity in this study was indicated by a lack of daily walking and 45.5% of the participants met this definition; this estimate is similar to those found in Saudi males over the age of 60 (48%).6 The obesity prevalence of this study was lower than that reported in the SHIS (34.3% vs. 48%).10 The difference in obesity prevalence was likely due to the difference in age distribution (SHIS 55-64 vs. current study 55-82 years). The prevalence of current cigarette smoking, found in this study, was very similar to what has been reported in SHIS among men aged 55 years or older (9.3% vs. 9.8%).5
The risk factors for chronic conditions that were identified in the current study are similar to those reported in earlier studies. In this study, univariate associations suggested that diet, exercise, BMI, and smoking were related to chronic conditions. These lifestyle factors have been consistently reported in the literature as being associated with various chronic conditions.2,17-19 The finding that the number of chronic conditions significantly increased with age and BMI was supported in the literature. In a nationally-representative sample of older adults (65+) in the US, the prevalence of chronic conditions increased with age from 74% among those aged 65-69 years to 88% among those aged 85 years and older.20 Similarly, in the Third National Health and Nutrition Examination Survey (III), the prevalence of having two or more health conditions increased with weight status category across all racial and ethnic subgroups.21 The higher number of chronic conditions among current smokers, found in this study is plausible since smoking has been associated with an increased risk of all major chronic diseases including heart diseases, asthma, ulcers, and cancer.22
A few limitations of this study should be noted. Majority of the diseases (i.e., heart disease, asthma, peptic ulcer, and cancer) were self-reported. Moreover, layman terms (e.g., heart disease) were used instead of more specific terms (such as coronary heart disease) for a better understanding of the question by the participants. The prevalence data were based on a single (as opposed to multiple) time point assessment; therefore, some degree of measurement error is likely.
This study used an innovative sampling strategy to obtain its participants. The barriers for selection of a random sample were the absence of a population database and the prevailing social norms that discourage home visit by unknown people (in this case research assistants). Therefore, mosques were chosen for sampling since they were a suitable gathering place for all those who could be theoretically eligible in this study. Moreover, it is customary among the Saudi people to go to mosque for daily prayers, and the rate is very high among older adult males. It should be noted that we missed those who were ill at the time of study or who could not attend prayer because of their physical disability.
The future studies should note the limitations of this study and improve on the design and the measurement. For example, a more representative sample by inclusion of female and obtaining it from a wider geographical area of the country. Second, the use of a full spectrum of diagnostic tools for a given disease (e.g., fasting in addition to random blood glucose for diabetes) or a validated check-list for self-reported diseases (e.g., asthma checklist for the detection of asthma) will make the outcome more accurate.
Conclusion
The prevalence of chronic diseases among elderly Saudi men was substantial. The number of chronic conditions increased as age and BMI increased; and current smokers were more likely to have a higher number of conditions. Future studies on the elderly Saudi population should include objective assessments of all the diseases and should be conducted on a national level.
Funding
This study was funded by the research unit at SRC through its annual allocation for the promotion of student research.
References
- 1.Abusaaq H. Population Aging in Saudi Arabia. Saudi Arabian Monetary Agency; 2015. http://www.sama.gov.sa/en-US/EconomicResearch/WorkingPapers/population%20aging%20in%20saudi%20arabia.pdf .
- 2.Memish ZA, Jaber S, Mokdad AH, Al-Mazroa MA, Murray CJ, Al Rabeeah AA, et al. Burden of disease, injuries, and risk factors in the Kingdom of Saudi Arabia 1990-2010. Prev Chronic Dis. 2014;11:E169. doi: 10.5888/pcd11.140176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Alqurashi KA, Aljabri KS, Bokhari SA. Prevalence of diabetes mellitus in a Saudi community. Ann Saudi Med. 2011;31(1):19–23. doi: 10.4103/0256-4947.75773. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Al-Nozha MM, Abdullah M, Arafah MR, Khalil MZ, Khan NB, Al-Mazrou YY, et al. Hypertension in Saudi Arabia. Saudi Med J. 2007;28(1):77–84. [PubMed] [Google Scholar]
- 5.Moradi-Lakeh M, El-Bcheraoui C, Tuffaha M, Daoud F, Al-Saeedi M, Basulaiman M, et al. Tobacco consumption in the Kingdom of Saudi Arabia 2013: Findings from a national survey. BMC Public Health. 2015;15:611. doi: 10.1186/s12889-015-1902-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Al-Hazzaa HM. Prevalence of physical inactivity in Saudi Arabia: A brief review. East Mediterr Health J. 2004;10:663–70. [PubMed] [Google Scholar]
- 7.El-Bcheraoui C, Tuffaha M, Daoud F, Kravitz H, Al-Mazroa MA, Al Saeedi M, et al. On your mark, get set, go: Levels of physical activity in the Kingdom of Saudi Arabia 2013. J Phys Act Health. 2016;13:231–8. doi: 10.1123/jpah.2014-0601. [DOI] [PubMed] [Google Scholar]
- 8.El-Bcheraoui C, Memish ZA, Tuffaha M, Daoud F, Robinson M, Jaber S, et al. Hypertension and its associated risk factors in the Kingdom of Saudi Arabia 2013: A national survey. Int J Hypertens. 2014;2014:564679. doi: 10.1155/2014/564679. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.El-Bcheraoui C, Basulaiman M, Tuffaha M, Daoud F, Robinson M, Jaber S, et al. Status of the diabetes epidemic in the Kingdom of Saudi Arabia 2013. Int J Public Health. 2014;59:1011–21. doi: 10.1007/s00038-014-0612-4. [DOI] [PubMed] [Google Scholar]
- 10.Memish ZA, El-Bcheraoui C, Tuffaha M, Robinson M, Daoud F, Jaber S, et al. Obesity and associated factors--Kingdom of Saudi Arabia 2013. Prev Chronic Dis. 2014;11:E174. doi: 10.5888/pcd11.140236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.General Authority of Statistics. Saudi Arabia. [[Last accessed on 2016 Dec]]. Available from: http://www.stats.gov.sa/sites/default/files/en-demographic-research-2016_2.pdf .
- 12.Freckmann G, Baumstark A, Jendrike N, Zschornack E, Kocher S, Tshiananga J, et al. System accuracy evaluation of 27 blood glucose monitoring systems according to DIN EN ISO 15197. Diabetes Technol Ther. 2010;12(3):221–31. doi: 10.1089/dia.2009.0128. [DOI] [PubMed] [Google Scholar]
- 13.Al-Daghri NM, Al-Attas OS, Alokail MS, Alkharfy KM, Yousef M, Sabico SL, et al. Diabetes mellitus Type 2 and other chronic non-communicable diseases in the central region, Saudi Arabia (Riyadh cohort 2): A decade of an epidemic. BMC Med. 2011;9:76. doi: 10.1186/1741-7015-9-76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Moradi-Lakeh M, El-Bcheraoui C, Daoud F, Tuffaha M, Kravitz H, Al Saeedi M, et al. Prevalence of Asthma in Saudi adults: Findings from a national household survey 2013. BMC Pulm Med. 2015;15:77. doi: 10.1186/s12890-015-0080-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Sonnenberg A, Everhart JE. The prevalence of self-reported peptic ulcer in the United States. Am J Public Health. 1996;86:200–5. doi: 10.2105/ajph.86.2.200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Moradi-Lakeh M, El-Bcheraoui C, Afshin A, Daoud F, Al-Mazroa MA, Al-Saeedi M, et al. Diet in Saudi Arabia: Findings from a nationally representative survey. Public Health Nutr. 2017;20(6):1075–1081. doi: 10.1017/S1368980016003141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Field AE, Coakley EH, Must A, Spadano JL, Laird N, Dietz WH, et al. Impact of overweight on the risk of developing common chronic diseases during a 10-year period. Arch Intern Med. 2001;161:1581–6. doi: 10.1001/archinte.161.13.1581. [DOI] [PubMed] [Google Scholar]
- 18.Elaziz KM, Gabal MS, Aldafrawy OA, Seif HA, Allam MF. Prevalence of metabolic syndrome and cardiovascular risk factors among voluntary screened middle-aged and elderly Egyptians. J Public Health (Oxf) 2015;37:612–7. doi: 10.1093/pubmed/fdu097. [DOI] [PubMed] [Google Scholar]
- 19.Afshin A, Micha R, Khatibzadeh S, Fahimi S, Shi P, Powles J, et al. The impact of dietary habits and metabolic risk factors on cardiovascular and diabetes mortality in countries of the Middle East and North Africa in 2010: A comparative risk assessment analysis. BMJ Open. 2015;5:e006385. doi: 10.1136/bmjopen-2014-006385. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Wolff JL, Starfield B, Anderson G. Prevalence, expenditures, and complications of multiple chronic conditions in the elderly. Arch Intern Med. 2002;162:2269–76. doi: 10.1001/archinte.162.20.2269. [DOI] [PubMed] [Google Scholar]
- 21.Must A, Spadano J, Coakley EH, Field AE, Colditz G, Dietz WH. The disease burden associated with overweight and obesity. J Am Med Assoc. 1999;282:1523–9. doi: 10.1001/jama.282.16.1523. [DOI] [PubMed] [Google Scholar]
- 22.U.S. Department of Health and Human Services. The Health Consequences of Smoking: A Report of the Surgeon General. In U.S. Department of Health and Human Services Centers for Disease Control and Prevention National Center for Chronic Disease Prevention and Health Promotion. Office on Smoking and Health. 2004 [Google Scholar]