

Abstract
Objective:
The current study was intended to evaluate the knowledge and awareness toward Middle East respiratory syndrome coronavirus (MERS-CoV) of pilgrims from Saudi Arabia and from different Arabian countries.
Methods:
A prospective study was conducted among pilgrims from Saudi Arabia and those from other Arab nations. A total number of 2120 participants including 736 Saudi pilgrims (436 males and 300 females) and 1384 non-Saudi Arabian pilgrims (1384; 909 males and 475 females) were included in the study. The responses of the participants were descriptively analyzed. Pearson correlation coefficient was used to screen the possible correlations among different variables. The differences in the responses between the two groups were evaluated using Mann–Whitney analysis.
Results:
The responses of the Saudi pilgrims showed statistically significant results in comparison to non-Saudi pilgrims in answering all questions except those related to the presence of efficient vaccination or treatment and the source of information. It was clear that the Saudi pilgrims were more oriented about different aspects of MERS-CoV including the nature of the causative agent, the signs, the severity of the disease, the animals that can transmit the infection to humans, the risk groups, and when one need to be screened for infection. In both Saudi and non-Saudi pilgrims, the official websites of health organizations constitute the main source of their information.
Conclusion:
It was concluded that Saudi pilgrims possess good knowledge about the MERS-CoV although more orientation is still required.
Keywords: MERS-CoV, Coronavirus, Pilgrims, Saudi Arabia
Introduction
The Middle East respiratory syndrome coronavirus (MERS-CoV) continues to cause sporadic cases and nosocomial outbreaks.1 MERS-CoV was firstly detected in the Arabian Peninsula in 2012 and responsible for at least 1864 laboratory-confirmed cases with approximately 35% case fatality. Although the disease was detected in about 27 countries, >80% of cases were detected in Saudi Arabia.2 MERS-CoV is classified as lineage C of the genus Betacoronavirus.3 Insect-eating bats are currently the known potential reservoir host for MERS-CoV4,5 while dromedary camels are the known potential animal host.6,7 Consumption of raw camel products and direct contact with camels may constitute a possible role of disease transmission.8
MERS-CoV affects all ages. The clinical epidemiology of MERS-CoV cases showed similarity to the seasonal flu; however, severe cases have been reported in elderly individuals and immune compromised patients with underlying conditions.9 Health-care workers are among the risk groups2 and asymptomatic health-care workers spread illness among hospitalized patients.10
Annually, Saudi Arabia hosts at least three million Muslims from different nationalities at the same time in Mekkah during the pilgrimage season. Pilgrims also visit Medinah after finishing the pilgrimage rituals. Accordingly, there is a possibility of transmission of different diseases among pilgrims. Interestingly, no notification of laboratory-confirmed MERS-CoV cases during pilgrimage seasons was reported; however, several imported MERS-CoV cases were recorded among returning individuals who visited Mekkah and Medinah in different countries including the Netherlands, UK, Algeria, Tunisia, and Malaysia.11-13
Appropriate public health responses are dependent on high-quality knowledge and awareness about important aspects of the disease. Whenever facing an outbreak, there is always a need for health education programs to raise the public awareness with regular evaluation of the level of knowledge to fill gaps of deficient or lack of information. MERS-CoV is a good case in point that constituted a real panic to populations. Preparing population adequately for this threat involves action on many fronts, including enhancing the public awareness toward the basic knowledge about the disease that is one key pillar of an enhanced outbreak investigation, response, and control system. We argue that our thinking should converge on the public awareness and we should address the gaps of all disciplines of the disease. The initial public health response to the MERS-CoV have been poorly calibrated owing to early estimates of the case fatality rate.14 What was initially thought to be a potential threat and severe novel coronavirus turned out to be no more severe than an average respiratory infection.15,16 The current study aimed to evaluate the level of knowledge and awareness of the Saudi and non-Saudi-Arabian pilgrims regarding the MERS-CoV.
Methods
This study has reviewed and approved by the Taif University Ethics Committee. During the pilgrimage season 2016, a prospective study has conducted among pilgrims from Saudi Arabia and those from other Arab nations. The respondents’ knowledge regarding MERS-CoV and their understanding of the risk of MERS-CoV infection were descriptively analyzed. The questionnaire was distributed in Mina, Saudi Arabia. The sample size was calculated using RASOFT online freely available program (http://www.raosoft.com/samplesize.html) with 99% confidence level. A total number of 2120 participants including 736 Saudi and non-Saudi Arabian pilgrims (1384; 909 males and 475 females) were included in the study. Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS) v.16.0 (SPSS, Inc., Chicago, IL, USA). The numbers and the percentages of the different variables were estimated using descriptive analysis. Pearson correlation coefficient and chi-square test were used to evaluate variables and determine the possible correlations. The data from Saudi and non-Saudi were compared statistically analyzed using Mann-Whitney analysis.
Results
A total number of 2120 pilgrims were enrolled in the current study: 736 Saudi (436 males and 300 females) and 1384 non-Saudi Arabian pilgrims (909 males and 475 females). About 44% (333/736) of the Saudi and 43% (595/1384) of the non-Saudi pilgrims hold a high level of education; a bachelor degree or higher. The major source of information included the official websites of health organizations (39.54%, 49.49%) followed by the social media (25.95, 20.23) for Saudi and non-Saudi pilgrims, respectively, with no statistical significance detected between the Saudi and non-Saudi pilgrims (Table 1). Both groups of pilgrims (n: 2120) were first screened for the overall knowledge and awareness toward MERS-CoV. Results showed incorrect knowledge and awareness when asking the whole pilgrims about the following information: MERS-CoV appears in certain time in the year, MERS-CoV is a fatal disease to any person, the animal source of the disease, the probability of camel meat and milk to transmit the disease, whether people should be screened after coming in contact with laboratory-confirmed cases and the presence of available vaccine and antiviral for the MERS-CoV (Figure 1).
Table 1.
Demographic data and source of information for Saudi and non-Saudi Arabian pilgrims
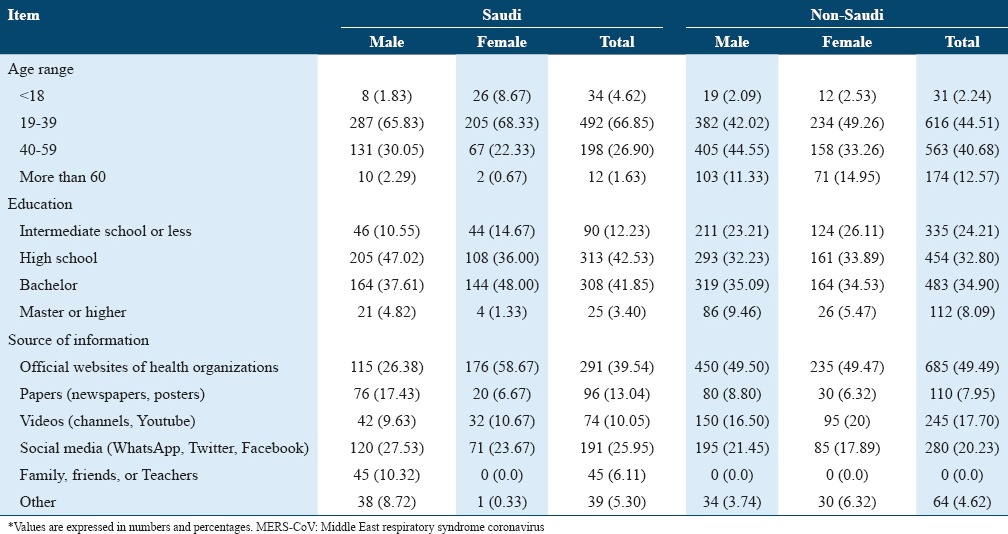
Figure 1.

The overall knowledge and awareness of all the pilgrims toward Middle East respiratory syndrome coronavirus (MERS-CoV). Q1 - What is the MERS-CoV, Q2 - MERS-CoV appears in certain time in the year, Q3 - MERS-CoV signs are similar to Flu, Q4 - MERS-CoV is a fatal disease to any person, Q5 - The following animals can transmit the MERS-CoV, Q6 - Camel milk and meat may transmit the MERS-CoV to humans, Q7 - People having chronic medical illnesses are considered high-risk group, Q8 - Being health-care workers make you more susceptible to get the disease, Q9 - If you come in contact to laboratory confirmed MERS-CoV infected person, you should be monitored for MERS-CoV, Q10 - Currently, there is an effective treatment for MERS-CoV, Q11 - Currently, there is a vaccine for MERS-CoV
On comparing the Saudi and non-Saudi Arab pilgrims, the level of knowledge was changed according to whether the tested participants were Saudi or not. The Saudi pilgrims showed significant differences in the level of knowledge than non-Saudi Arabian pilgrims in the following topics: The nature of MERS-CoV (79.35% vs. 61.78%, %, P = 0.042), the signs of the disease and its similarity to flu (78.94 vs. 65.17%, P< 0.001), the severity of the disease (55.3% vs. 35.48%. P = 0.036) and the animals that could transmit the disease (48.37% vs. 28.54%, P = 0.015), (Table 2). Both groups showed a low level of knowledge regarding the seasonal nature of the disease, and camel milk and meat as possible sources of disease transmission (Table 2). No significant differences were detected among male and female participants in both groups (Table 2). The Saudi pilgrims showed higher level of knowledge regarding the fact that being health-care workers is a risk factor (68.61 vs. 48.55, P < 0.001) and the necessity for screening for MERS-CoV when being in contact with the infected persons (61.01 vs. 46.46, P = 0.009). There was no significant differences between Saudi and non-Saudi Arabian pilgrims regarding the absence of an effective antiviral treatment (46.60 vs. 27.38) and the absence of an effective vaccine against MERS-CoV (38.99 vs. 22.54) (Table 3). No significant correlation was detected among different questions.
Table 2.
Knowledge about the MERS-CoV causative agent, signs, severity, and disease transmission

Table 3.
Knowledge and awareness to the MERS-CoV among Saudi and non-Saudi Arabian pilgrims regarding risk groups, patient isolation, treatment, and vaccination

Discussion
A total number of 2120 pilgrims were enrolled in the current study: 736 Saudi and 1384 non-Saudi Arabian pilgrims). The major source of information of the participants included the official websites of health organizations followed by the social media for Saudi and non-Saudi pilgrims, respectively. Previous study revealed that the social media constituted the main source of knowledge for medical students.17 Meanwhile, in one of our unpublished data for the general population, the health-care workers and physicians constituted the main source of information.
The Saudi pilgrims showed a good level of the overall knowledge about the nature of MERS-CoV including: The causative agent, the signs of the disease, its similarity to flu, the severity of the disease. Correct answers were expressed in considerable high percentages of the participants. Meanwhile, non-Saudi pilgrims showed a lower level of knowledge for the same questions. In contrast, both groups showed a low level of knowledge regarding the seasonal nature of the disease. High level of awareness among Saudi populations and medical students have previously detected and found consistent with our results.10,18 In comparison to the previous studies, our study demonstrates that the Saudi and Arabian non-Saudi pilgrims showed more awareness of the disease than French and Australian Pilgrims did.19,20
Although the Saudi pilgrims showed a better level of knowledge regarding the animal source of the disease in comparison to the non-Saudi Arabian pilgrims, a deficiency in the information in almost half of the population was noticed. This finding agrees with that recorded previously in Saudi Arabia.17 Raw camel milk and cooked camel meat are commonly consumed in the Arab Gulf area. There is a raised concern about the risk of consumption of raw camel products as a potential source of MERS-CoV infection.21 It was found that both Saudi Arabian and non-Saudi Arabian participants showed unsatisfactory awareness about this important matter. Pilgrims who were aware of MERS-CoV animal sources were also found oriented about risks from consuming non-heat treated camel products compared with those who were unaware. This finding agrees with the results reported previously in Tashani et al. 2014.19
Health-care workers are prone to capture infection from their close contact with infected individuals, accordingly, they are considered among the risk groups.2 In addition, asymptomatic health-care workers play an important role in spreading the illness among hospitalized patients.10 The Saudi pilgrims showed a higher level of knowledge regarding the fact that being health-care workers is a risk factor.
According to the center of disease control and prevention guidelines for monitoring persons with potential MERS-CoV exposure, both symptomatic and asymptomatic people who were exposed to laboratory confirmed cases must undergo active monitoring until 14 days after the past potential exposure.22 Interestingly, the majority of both Saudi and non-Saudi pilgrims were aware of the necessity of monitoring for MERS-CoV upon exposure to the infected persons; however, awareness level was higher in Saudi pilgrims than non-Saudi ones.
Currently, there is neither a commercially available protective vaccine nor a specific antiviral treatment for MERS-CoV.23 There was a relatively insufficient awareness about the availability of effective vaccine and antiviral agents for MERS-CoV among Saudi and non-Saudi pilgrims; however, the awareness level was higher in Saudi pilgrims in comparison to no Saudi ones.
Although the current study reveals a better level of knowledge and awareness regarding the MERS-CoV, more effort should be paid to enhance the public misconceptions regarding the animal source of the disease and animal products handling, as well as cases who should be suspected to screening to MERS-CoV. The knowledge and awareness about the disease are important for the adoption of the protective measures that minimize the risk exposure for the disease. Theoretically, health behavior style of an individual may be helpful in leading people from awareness and perception of the severity to disease susceptibility, to action.24
Conclusion
This study showed that awareness toward MERS-CoV of the Saudi pilgrims is better in the overall knowledge than non-Saudi-Arab ones. However, in both groups misperceptions toward high-risk believes still exist. The relatively lower level of knowledge among non-Saudi Arab pilgrims toward MERS-CoV may necessitate enhancing the health authorities in their countries of origin to take more active role in sharing the health information about the disease.
References
- 1.Zumla A, Alagaili AN, Cotten M, Azhar EI. Infectious diseases epidemic threats and mass gatherings: Refocusing global attention on the continuing spread of the Middle East Respiratory syndrome coronavirus (MERS-CoV) BMC Med. 2016;14:132. doi: 10.1186/s12916-016-0686-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.WHO. Summary of Current Situation, Literature Update and Risk Assessment. 2015. [[Last accessed on 2015 Jul 07]]. Available from: http://www.who.int/csr/don/2013_05_08_ncov/en/index.html .
- 3.Abdel-Moneim AS. Middle East respiratory syndrome coronavirus (MERS-CoV): Evidence and speculations. Arch Virol. 2014;159:1575–84. doi: 10.1007/s00705-014-1995-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Annan A, Baldwin HJ, Corman VM, Klose SM, Owusu M, Nkrumah EE, et al. Human betacoronavirus 2c EMC/2012-related viruses in bats, Ghana and Europe. Emerg Infect Dis. 2013;3:456–9. doi: 10.3201/eid1903.121503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Memish ZA, Mishra N, Olival KJ, Fagbo SF, Kapoor V, Epstein JH, et al. Middle East respiratory syndrome coronavirus in bats, Saudi Arabia. Emerg Infect Dis. 2013;19:1819–23. doi: 10.3201/eid1911.131172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hemida MG, Chu DK, Poon LL, Perera RA, Alhammadi MA, Ng HY, et al. MERS coronavirus in dromedary camel herd, Saudi Arabia. Emerg Infect Dis. 2014;20:1231–4. doi: 10.3201/eid2007.140571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Raj VS, Farag EA, Reusken CB, Lamers MM, Pas SD, Voermans J, et al. Isolation of MERS coronavirus from a dromedary camel, Qatar 2014. Emerg Infect Dis. 2014;20:1339–42. doi: 10.3201/eid2008.140663. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Reusken CB, Farag EA, Jonges M, Godeke GJ, El-Sayed AM, Pas SD, et al. Middle East respiratory syndrome coronavirus (MERS-CoV) RNA and neutralising antibodies in milk collected according to local customs from dromedary camels, Qatar, April 2014. Euro Surveill. 2014;19:20829. doi: 10.2807/1560-7917.es2014.19.23.20829. [DOI] [PubMed] [Google Scholar]
- 9.Penttinen P, Kaasik-Aaslav K, Friaux A, Donachie A, Sudre B, Amato-Gauci A, et al. Taking stock of the first 133 MERS coronavirus cases globally--is the epidemic changing? Euro Surveill. 2013;18:20596. doi: 10.2807/1560-7917.es2013.18.39.20596. [DOI] [PubMed] [Google Scholar]
- 10.Al-Mohrej OA, Al-Shirian SD, Al-Otaibi SK, Tamim HM, Masuadi EM, Fakhoury HM. Is the Saudi public aware of Middle East respiratory syndrome? J Infect Public Health. 2016;9:259–66. doi: 10.1016/j.jiph.2015.10.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Al-Tawfiq JA, Omrani AS, Memish ZA. Middle East respiratory syndrome coronavirus: Current situation and travel-associated concerns. Front Med. 2016;10:111–9. doi: 10.1007/s11684-016-0446-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Sridhar S, Brouqui P, Parola P, Gautret P. Imported cases of Middle East respiratory syndrome: An update. Travel Med Inf Dis. 2015;13:106–9. doi: 10.1016/j.tmaid.2014.11.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kraaij-Dirkzwager M, Timen A, Dirksen K, Gelinck L, Leyten E, Groeneveld P, et al. Middle East respiratory syndrome coronavirus (MERS-CoV) infections in two returning travellers in the Netherlands, May 2014. Euro Surveill. 2014;19:20817. doi: 10.2807/1560-7917.es2014.19.21.20817. [DOI] [PubMed] [Google Scholar]
- 14.Rojek AM, Horby PW. Modernising epidemic science: Enabling patient-centred research during epidemics. BMC Med. 2016;14:212. doi: 10.1186/s12916-016-0760-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Zumla AI, Memish ZA. Middle East respiratory syndrome coronavirus: Epidemic potential or a storm in a teacup? Eur Respir J. 2014;43:1243–8. doi: 10.1183/09031936.00227213. [DOI] [PubMed] [Google Scholar]
- 16.Abdel-Moneim AS. Middle-East respiratory syndrome coronavirus: Is it worth a world panic? World J Virol. 2015;4:185–7. doi: 10.5501/wjv.v4.i3.185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Al-Mohrej A, Agha S. Are Saudi medical students aware of Middle East respiratory syndrome coronavirus during an outbreak? J Inf Public Health. 2016;10(4):388–395. doi: 10.1016/j.jiph.2016.06.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kharma MY, Alalwani MS, Amer MF, Tarakji B, Aws G. Assessment of the awareness level of dental students toward Middle East respiratory syndrome-coronavirus. J Int Soc Prev Community Dent. 2015;5:163–9. doi: 10.4103/2231-0762.159951. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Tashani M, Alfelali M, Barasheed O, Fatema FN, Alqahtani A, Rashid H, et al. Australian Hajj pilgrims’ knowledge about MERS-CoV and other respiratory infections. Virol Sin. 2014;29:318–20. doi: 10.1007/s12250-014-3506-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Gautret P, Benkouiten S, Salaheddine I, Belhouchat K, Drali T, Parola P, et al. Hajj pilgrims knowledge about Middle East respiratory syndrome coronavirus, August to September 2013. Euro Surveill. 2013;18:20604. doi: 10.2807/1560-7917.es2013.18.41.20604. [DOI] [PubMed] [Google Scholar]
- 21.Hoda J. Identification of information types and sources by the public for promoting awareness of Middle East respiratory syndrome coronavirus in Saudi Arabia. Health Educ Res. 2016;31:12–23. doi: 10.1093/her/cyv061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.CDC. Interim U.S. Guidance for Monitoring and Movement of Persons with Potential Middle East Respiratory Syndrome Coronavirus (MERS-CoV) Exposure. 2016 [Google Scholar]
- 23.CDC. Middle East Respiratory Syndrome Coronavirus (MERS-CoV): Treatment and Prevention. 2016. [[Last accessed on 2016 Jul 13]]. Available from: https://www.cdc.gov/coronavirus/mers/about/prevention.html .
- 24.Weinstein ND, Sandman PM. A model of the precaution adoption process: Evidence from home radon testing. Health Psychol. 1992;11:170–80. doi: 10.1037//0278-6133.11.3.170. [DOI] [PubMed] [Google Scholar]