

Abstract
Background
To define the benefits of different methods for diagnosis of pediatric appendicitis in Taiwan, a nationwide cohort study was used for analysis.
Methods
We identified 44,529 patients under 18 years old who had been hospitalized with a diagnosis of acute appendicitis between 2003 and 2012. We analyzed the percentages of cases in which ultrasound (US) and/or computed tomography (CT) were performed and non-perforated and perforated appendicitis were diagnosed for each year. Multivariate logistic regression analyses were performed to evaluate risk factors for perforated appendicitis.
Results
There were more cases of non-perforated appendicitis (N = 32,491) than perforated appendicitis (N = 12,038). The rate of non-perforated cases decreased from 0.068% in 2003 to 0.049% in 2012; perforated cases remained relatively stable at 0.024%~0.023% from 2003 to 2012. The percentage of CT evaluation increased from 3% in 2003 to 20% in 2012; the rates of US or both US and CT evaluations were similar annually. The percentage of neither CT nor US evaluation gradually decreased from 97% in 2003, to 79% in 2012. The odds ratios of a perforated appendix for those patients diagnosed by US, CT, or both US and CT were 1.227 (95% confidence interval (CI) 0.91, 1.65; p = 0.173), 2.744 (95% CI 2.55, 2.95; p < 0.001), and 5.062 (95% CI = 3.14, 8.17; p < 0.001), respectively, compared to patients who did not receive US or CT. The odd ratios of a perforated appendix for those patients 7–12 and ≤6 years old were 1.756 (95% CI 1.67, 1.84; p < 0.001) and 3.094 (95% CI 2.87, 3.34; p < 0.001), respectively, compared to those 13–18 years old.
Conclusions
Our study demonstrated that using CT scan as a diagnostic tool for acute appendicitis increased annually; most patients especially those ≤6 years old who received CT evaluation had a greater risk of having perforated appendicitis. We recommend a prompt appendectomy in those pediatric patients with typical clinical symptoms and physical findings for non-complicated appendicitis to avoid the risk of appendiceal perforation.
Keywords: Appendicitis, Ultrasound, Computed tomography, National Health Insurance Database
Background
Appendectomies are one of the most common general surgical procedures performed in the pediatric population. Traditionally, a diagnosis of appendicitis in both children and adults is made by history taking and a physical examination. In general, it is more difficult to obtain a clear history and elicit specific physical examination findings in children of all ages compared to adults [1]. A clinical diagnosis of appendicitis is often difficult, and a delayed diagnosis may result in perforation of the inflamed appendix, peritonitis, or intra-abdominal abscess formation.
Recently, ultrasound (US) and computed tomography (CT) have been used to assist in diagnosing appendicitis. US was initially used [2], but focused CT has become increasingly common as a diagnostic tool in both adults and children to rule out appendicitis in hopes of improving the diagnostic accuracy [3, 4]. Both diagnostic procedures have proven to be much sensitive and specific [5]. Perforation rate of pediatric appendicitis was relatively high in preschool age group and the rate of perforation was inversely proportional to patient age, occurring in 57% ages 4–5 years to 100% aged <1 year [6]. Even with advances in US and CT imaging, perforation rates in children under 6 years was 51–100% over past decades [7–9], therefore there are still critics who question the overlap of these two diagnostic procedures and the benefits of CT over US in terms of the clinical diagnosis [10–12].
As the use of CT and US appears to be increasing, we sought to analyze a large, national database over a 10-year period to evaluate changes in the diagnostic approaches and the impact on the occurrence of perforated appendicitis.
Methods
Database
This study was a nationwide, retrospective, population-based analysis of insurance claims data from 23 million insured people obtained from Taiwan’s National Health Insurance (NHI) program. The Bureau of NHI (BNHI) in Taiwan has released a research-oriented database through the Collaboration Center for Health Information Application (CCHIA). Taiwan launched the NHI program in 1995, which covered 99% of the population of Taiwan in 2007. Therefore, the BNHI allows researchers to trace almost all utilizations of medical services for all children with appendicitis in Taiwan.
We used data sourced between 2003 and 2012 from the NHI database released by the BNHI of NHI through the CCHIA. The database includes all original claims data and registration files for beneficiaries enrolled under Taiwan’s NHI program.
This study was exempted from full review by the Taipei Medical University-Joint Institutional Review Board (No: 201,404,074) since the NHI database consists of anonymous secondary data released to the public for research purposes.
Study sample
We identified 44,529 pediatric patients (< 18 years of age) who had a first-time discharge diagnosis of acute appendicitis (International Classification of Disease, Ninth Revision, Clinical Modification (ICD-9-CM) codes 540.0, 540.1, and 540.9) between January 2003 and December 2012. If a patient had two or more hospitalizations within a 30-day period, they were regarded as the same episode, and we only included the first hospitalization.
we hypothesize that there is possible correlation of age factors in the perforation of pediatric appendicitis, patients were divided into three groups by age: ≤ 6, 7–12, and 13–18 years old. The incidence of disease and the severity of disease were compared among groups. The types of diagnosis were categorized as follows: US (19005B), CT (33070B and 33071B), both US and CT, and neither US nor CT.
We calculated the percentages of cases on which the four categories of diagnostic tools were performed for each year, and also calculated the percentages of non-perforated and perforated appendicitis cases diagnosed each year.
Outcome measures
Primary endpoint measure
Possible correlation of age factors in the perforation of pediatric appendicitis is measured. The initial hypothesis predicts that younger patients are under higher risk of perforation in appendicitis.
-
(2)
Secondary endpoint measure
Both US or CT examinations require scheduling and waiting time; we infer such latency from clinical suspicion to confirmation of diagnosis may increase the risk of appendiceal perforation.
Statistical analyses
Chi-squared tests were used to examine the difference between the perforated and non-perforated (control) groups. We then performed a multivariate logistic regression to explore the odds ratios (ORs) and the related 95% confidence interval (CI) of perforated appendicitis cases among the different age groups, between genders, and among different diagnostic groups. All statistical analyses were performed using SAS version 9.3 (SAS Institute, Cary, NC), and p < 0.05 was considered statistically significant.
Results
Characteristic of the study population
Table 1 shows the distributions of rates of acute non-perforated and acute perforated appendicitis cases between genders and among different age groups. Of the 44,529 pediatric patients under 18 years old admitted for treatment of acute appendicitis between January 2003 and December 2012, 26,792 (60%) were boys and 17,737 (40%) were girls. There were more cases of non-perforated appendicitis (N = 32,491) than perforated appendicitis (N = 12,038).
Table 1.
Baseline patient characteristics
| Non-perforated appendicitis (N = 32,491) No % |
Perforated appendicitis (N = 12,038) No. % |
p-value* | ||||
|---|---|---|---|---|---|---|
| Gender | ||||||
| Male | 19,494 | 60 | 7298 | 60.62 | 0.2346 | |
| Female | 12,997 | 40 | 4740 | 39.38 | ||
| Age group (y/o) | ||||||
| ≤ 6 | 2383 | 7.33 | 2014 | 16.73 | <0.0001* | |
| 7–12 | 11,575 | 35.63 | 5205 | 43.24 | ||
| 13–18 | 18,533 | 57.04 | 4819 | 40.03 | ||
*Significant differences: p < 0.05
Most of the patients (90.1%) were aged between 7 and 18 years. As shown in Table 1, the youngest age group patients (≤ 6 years old) experienced the highest incidence of perforated appendicitis (46%), which decreased to 31% in the 7–12 year age group and then to 21% in the 13–18 year age group.
Annual incidence of non-perforated appendicitis and perforated appendicitis
Figure 1 shows that the incidence of the cases of non-perforated appendicitis significantly decreased over the study time course. The incidence of the cases of non-perforated appendicitis were 0.068% in 2003, 0.066% in 2004, and decreased to 0.055% in 2011 and 0.049% in 2012. Interestingly, the incidence of perforated appendicitis cases remained relatively stable at 0.024%~0.023% from 2003 to 2012.
Fig. 1.
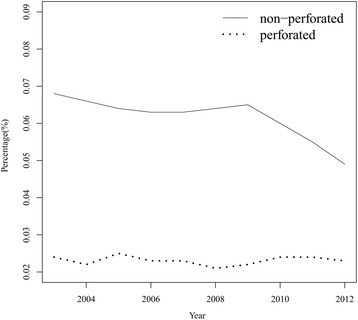
Percentages of patients with non-perforated vs. perforated appendixes from 2003 to 2012
Annul comparison of the performance of US and CT evaluation
Figure 2 shows increasing trend in the performance of CT evaluation over the 10-year period. The percentage of CT evaluation increased from 3% in 2003, 4% in 2004, to 20% in 2012, the percentage of US evaluation or combined US with CT evaluation were relatively similar from 2003 to 2012. The percentage of the patients proceeding to an appendectomy without evaluation of US and CT gradually decreased from 97% and 95% in 2003 and 2004, respectively, to 79% in 2012.
Fig. 2.
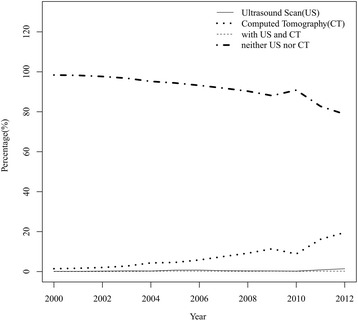
Percentages of patients who received ultrasound (US) and computed tomography (CT)
Predictors for appendiceal perforation in appendicitis
Table 2 provides the adjusted ORs for a perforated appendix. Compared to the patients without evaluation of US and CT, the adjusted ORs for a perforated appendix for those patients diagnosed by US, CT, and both US and CT were 1.227 (95% CI 0.91, 1.65; p = 0.071), 2.744 (95% CI 2.55, 2.95; p < 0.001), and 5.062 (95% CI 3.14, 8.17; p < 0.001). Higher rates of perforated appendices were detected among patients between 7 and 12 years old and <6 years old and were 1.756 (95% CI = 1.67, 1.84; p < 0.001) and 3.094 (95% CI 2.87, 3.34; p < 0.001), respectively, compared to those aged 13–18 years.
Table 2.
Adjusted odds ratios for perforated appendicitis
| Variables | ORs | 95% CI | p-value * |
|---|---|---|---|
| Gender | |||
| Male | 1 | – | – |
| Female | 0.985 | 0.94–1.03 | 0.5372 |
| Age group (y/o) | |||
| 13–18 | 1 | – | – |
| 7–12 | 1.756 | 1.67–1.84 | <0.0001* |
| ≤ 6 | 3.094 | 2.87–3.34 | <0.0001* |
| Type of diagnosis | |||
| Neither US nor CT | 1 | – | – |
| US | 1.227 | 0.91–1.65 | 0.1729 |
| CT | 2.744 | 2.55–2.95 | <0.0001* |
| Both US and CT | 5.062 | 3.14–8.17 | <0.0001* |
ORs odds ratios, CI confidence interval, US ultrasound, CT computed tomography
*Significant differences: p < 0.05
Discussion
To the best of our knowledge, this is the first study to encompass a large nationwide database to investigate diagnostic approaches for appendicitis in children. The data herein demonstrated that the percentage of children who underwent CT scan increased annually from 2003 on, and still 79% of patients with appendicitis were only diagnosed by clinical judgment. We also found that most patients, especially those aged ≤6 years, who received a CT scan were more likely to have a greater proportion of perforated appendices.
Appendicitis is the most common surgical emergency in children. Our population-based study demonstrated that the largest number of patients was in the 11–18-year age group, which represented 75% of the total population. The ratio of boys to girls was about 1.5:1. A previous report showed an incidence peak in the 10~19-year age group, and it was estimated that the risks of appendicitis were 8.6% for men and 6.7% for women [13]. In our study, the number of cases of non-perforated appendicitis (n = 32,491) was higher than that of perforated appendicitis (n = 12,038).
Despite great familiarity with this disease, appendicitis continues to pose a significant diagnostic challenge for clinicians [14]. This is especially true in very young children whose history is not typical and whose examination results are also unreliable [15, 16]. It is a trend to use US or CT examination to assist the diagnosis of appendicitis in children in these decades. In our country, majority of the hospital or medical center use US and/or CT to diagnose pediatric appendicitis. In the early 1990s, multiple institutions advocated US as a useful adjunct for diagnosing appendicitis [17–19]. In addition, initial reports by Rao using CT scans to diagnose appendicitis in adults in 1997 led to it being used more frequently in pediatric populations [3, 4]. Both diagnostic procedures have proven to be very sensitive and specific, and appeared to be the preferred imaging modalities for appendicitis in children in our country since 2003. In our series, the use of CT scan significantly increased over the 10-year period. The percentage of the patients who having CT scan increased from 3% to 20%, and the percentage of the patients proceeding to an appendectomy without evaluation of US and CT gradually decreased from 97% to 79%.
Previous studies debated the impacts of CT scans on negative appendectomy and perforation rates [7, 20, 21]. In our series, the incidence of non-perforated appendicitis significantly decreased over the study time course. Interestingly, the rate of perforations remained relatively stable at 0.024%~0.023% from 2003 to 2012. The increased utility of US and CT did not affect the outcome of perforated appendicitis over the study period, but the incidence of non-perforated appendicitis reduced. The reason may be that those patients with suspicious appendicitis without US or CT confirmation may undergo negative appendectomies. If those patients received either or both study, the negative appendectomies may be avoided. The data of ORs demonstrated that patients who received CT or both US and CT had higher rates of the occurrence of perforated appendicitis, especially patients who were ≤6 years old. In our evaluation, the youngest age group (≤ 6 year) had the highest incidence of appendiceal perforation (46%). Various studies have reported ruptured appendicitis rates of 30%~45% [22]. In the study, we are not able to collect the exact data of waiting time for the US or CT examinations in the patients, but both examinations require scheduling and waiting time that should hold true in most circumstances. We infer that the latency from clinical suspicion of acute appendicitis to confirmation of diagnosis by CT or US examinations may increase the risk of appendiceal perforation. A controversial adult report indicated that neither the use of CT nor US led to improve the diagnostic accuracy for acute appendicitis, these procedures might delay surgical consultation and necessary appendectomy. [23] Most hospital institutions have reached a general consensus that for adult patients with suspicion of acute appendicitis, selective use of imaging studies is recommended [24]. The diagnosis or exclusion of appendicitis may be made clinically. However, imaging studies may reduce the negative appendectomy rate [4]. Schuler et al. indicated that the use of CT reduced the negative appendectomy rate for adult patients from 21% without the use of preoperative CT, to 6% with the use of CT [25]. The causal relationship between imaging studies and the occurrence of perforated appendicitis in pediatric acute appendicitis is unknown due to lack of evidence in the literature or research. This is beyond the scope of current study; a future longitudinal study is needed to clarify such relationship.
There are some limitations to this study. The database (the Collaboration Center for Health Information Application) in the study did not provide the socio-economic status, duration of symptoms, and presenting complaint/physical signs. Most medical expenses are covered by national health insurance in our country; therefore socio-economic factor is relatively less relevant in the current study. First, the detailed pathologic confirmation of appendicitis was not available from the database we used, and the definition of appendicitis mainly depended on ICD-9 codes. Second, the dataset in this study had no data on pre-hospital care (the time from the onset of symptoms to first seeking medical attention) of the duration of advanced testing, and the data about the latency from the clinical suspicion of acute appendicitis to the confirmation of diagnosis by US or CT examinations was not available. Therefore, these potentially confounding factors could not be considered in our analysis. Future studies collaborating with other medical centers are expected in order to obtain more detailed clinical data for further analysis. Third, the clinical information about negative appendectomy was not available from the database of the study because negative appendectomy has no suitable ICD-9 to match, which may help to explain the reason for decreased incidence of non-perforated appendectomies in our study, a future longitudinal study is needed to clarify such relationship.
Knowledge of the risks of cumulative radiation exposure from radiographic procedures has led to campaigns aimed at increasing awareness and decreasing radiation exposure [26–30]. Children are more radiosensitive, receive large effective doses for a given level of radiation, and have a longer life expectancy during which to develop cancer [29, 30]. Some recent reports advocated the use of US followed by CT scans [31, 32]. The accuracy of pediatric US in those reports varies from 44% to 94% and the specificity from 47% to 95%. In our series, using US was not popular in the past 10-year period. We suggest that using US instead of CT as the initial modality of diagnosing appendicitis can be done to reduce radiation exposure.
Conclusions
In summary, our study demonstrated that using CT scan as a diagnostic tool for children’s acute appendicitis gradually increased annually we evaluated. The patients especially those ≤6 years old who received CT evaluation are under greater risk of perforated appendicitis. Further analysis of risk factors for a greater risk of perforated appendicitis in those younger patients who received CT scan is needed. We further emphasize the importance of prompt appendectomy in those pediatric patients with typical clinical symptoms and physical findings for an acute non-complicated appendicitis to avoid the appendiceal perforation and its related medical issue and complications.
Acknowledgements
We thank Prof. Winston W. Shen who gave constructive editorial comments on this manuscript.
Funding
This study was not funded by grants or other financial sponsors. All the authors declare that he has no any financial arrangement with a company whose product is discussed in the manuscript.
Availability of data and materials
The study did not contain confidential patient data. No further data will be shared because all the data supporting the findings is contained within the manuscript.
Abbreviations
- BNHI
Bureau of NHI
- CCHIA
Collaboration Center for Health Information Application
- CI
Confidence interval
- CT
Computed tomography
- ICD-9-CM
International Classification of Disease, Ninth Revision, Clinical Modification
- NHI
National health insurance
- ODs
Odds ratios
- US
Ultrasound
Authors’ contributions
CCL and WKC had full access to all of the data in the analysis and for the integrity of the data and the accuracy of the data analysis. CSH and HCL contributed to the design of the analysis; SMW, HCH, and RJC contributed to the data collection and analysis of the study; CCL, WKC, and HCC contributed to the interpretation of the data, preparation and writing of the manuscript; all authors reviewed the final manuscript. HCC revised the work critically for important intellectual content. All authors read and approved the final manuscript.
Ethics approval and consent to participate
The NHI database used in this study consists of anonymous secondary data released to the public for research purposes. This study did not contain confidential patient data. Taipei Medical University-Joint Institutional Review Board approved this study (No: 201,404,074). The patient’s consent to participate is not applicable in this study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Chih-Cheng Luo, Email: 102145@w.tmu.edu.tw.
Wen-Kuei Chien, Email: motorona74@gmail.com.
Chen-Sheng Huang, Email: 95119@w.tmu.edu.tw.
Hung-Chieh Lo, Email: carfishcat@yahoo.com.tw.
Sheng-Mao Wu, Email: mitralw@hotmail.com.
Hung-Chang Huang, Email: 141023@h.tmu.edu.tw.
Ray-Jade Chen, Email: rayjchen@tmu.edu.tw.
Hsun-Chin Chao, Phone: 886 3 3281200, Email: hcchao1021@gmail.com.
References
- 1.Gamal R, Moore TC. Appendicitis in children aged 13 years and younger. Am J Surg. 1990;159:589–592. doi: 10.1016/S0002-9610(06)80073-5. [DOI] [PubMed] [Google Scholar]
- 2.Rodriguez DP, Vargas S, Callahan MJ, Zurakowski D, Taylor GA. Appendicits in young children: imagine experience and clinical outcomes. AJR. 2006;186:1158–1164. doi: 10.2214/AJR.05.0055. [DOI] [PubMed] [Google Scholar]
- 3.Rao PM, Rhea JT, Novelline RA, Mustafavi AA, McCabe CJ. Effect of computed tomography of the appendix on treatment of patients and use of hospital resources. N Engl J Med. 1998;338:141–146. doi: 10.1056/NEJM199801153380301. [DOI] [PubMed] [Google Scholar]
- 4.Balthazar EJ, Rofsky NM, Zucker R. Appendicitis: the impact of computed tomography imaging in negative appendectomy and perforation rates. Am J Gastroenterol. 1998;93:768–771. doi: 10.1111/j.1572-0241.1998.222_a.x. [DOI] [PubMed] [Google Scholar]
- 5.Garcia Peña BM, Mandl KD, Kraus SJ, Fischer AC, Fleisher GR, Lund DP, Taylor GA. Ultrasonography and limited computed tomography in the diagnosis and Management of Appendicitis in children. JAMA. 1999;282:1041–1046. doi: 10.1001/jama.282.11.1041. [DOI] [PubMed] [Google Scholar]
- 6.Bonadio W, Peloquin P, Brazg J, et al. Appendicitis in preschool aged children: regression analysis of factors associated with perforation outcome. J Pediatr Surg 2015;50:1569–1573. [DOI] [PubMed]
- 7.Colvin JM, Bachur R, Kharbanda A. The presentation of appendicitis in preadolescent children. Pediatr Emerg Care. 2007;23:849–855. doi: 10.1097/pec.0b013e31815c9d7f. [DOI] [PubMed] [Google Scholar]
- 8.Sakellaris G, Tilemis S, Charissis G. Acute appendicitis in preschool-age children. Eur J Pediatr. 2005;164:80–83. doi: 10.1007/s00431-004-1568-9. [DOI] [PubMed] [Google Scholar]
- 9.Lee SL, Stark R, Yaghoubian A, Kaji A. Does age affect the outcomes and management of pediatric appendicitis? J Pediatr Surg. 2011;46:2342–2345. doi: 10.1016/j.jpedsurg.2011.09.030. [DOI] [PubMed] [Google Scholar]
- 10.Thirumoorthi AS, Fefferman NR, Ginsburg HB, Kuenzler KA, Tomita SS. Managing radiation exposure in children-reexamining the role of ultrasound in the diagnosis of appendicitis. J Pediatr Surg. 2012;47:2268–2272. doi: 10.1016/j.jpedsurg.2012.09.018. [DOI] [PubMed] [Google Scholar]
- 11.Martin AE, Vollman D, Adler B, Caniano DACT. Scans may not reduce the negative appendectomy rate in children. J Pediatr Surg. 2004;39:886–890. doi: 10.1016/j.jpedsurg.2004.02.034. [DOI] [PubMed] [Google Scholar]
- 12.Stephen AE, Segev DL, Rayn DP, Mullins ME, Kim SH, Schnitzer JJ, Doody DP. The diagnosis of acute appendicitis in a pediatric population: to CT or not CT. J Pediatr Surg. 2003;38:367–371. doi: 10.1053/jpsu.2003.50110. [DOI] [PubMed] [Google Scholar]
- 13.Addiss DG, Shaffer N, Fowler BS, Tauxe RV. The epidemiology of appendicitis and appendectomy in the United States. Am J Epidemiol. 1990;132:910–925. doi: 10.1093/oxfordjournals.aje.a115734. [DOI] [PubMed] [Google Scholar]
- 14.Wagner JM, Mckinney WP, Carpenter JL. Does this patient have appendicitis? JAMA. 1996;276:1589–1594. doi: 10.1001/jama.1996.03540190061030. [DOI] [PubMed] [Google Scholar]
- 15.Reynolds SL. Missed appendicitis in a pediatric emergency department. Pediatr Emerg Care. 1993;9:1–3. doi: 10.1097/00006565-199302000-00002. [DOI] [PubMed] [Google Scholar]
- 16.Körner H, Söndenaa K, Söreide JA, Andersen E, Nysted A, Lende TH, Kjellevold KH. Incidence of acute non-perforated and perforated appendicitis: age-specific and sex-specific analysis. World J Surg. 1997;21:313–317. doi: 10.1007/s002689900235. [DOI] [PubMed] [Google Scholar]
- 17.Rice HE, Arbesman M, Martin DJ, Brown RL, Gollin G, Gilbert JC, Caty MG, Glick PL, Azizkhan RG. Does early ultrasonography after management of pediatric appendicitis? A prospective analysis. J Pediatr Surg. 1999;34:754–759. doi: 10.1016/S0022-3468(99)90369-X. [DOI] [PubMed] [Google Scholar]
- 18.Kaiser S, Mesas-Burgos C, Söderman E, Frenckner B. Appendicits in children: impact of US and CT on the negative appendectomy rate. Eur J Pediatr Surg. 2004;14:260–264. doi: 10.1055/s-2004-817841. [DOI] [PubMed] [Google Scholar]
- 19.Dilley A, Wesson D, Munden M, Hicks J, Brandt M, Minifee P, Nuchtern J. The impact of ultrasound examination on the management of children with suspected appendicitis: a 3-year analysis. J Pediatr Surg. 2001;36:303–308. doi: 10.1053/jpsu.2001.20702. [DOI] [PubMed] [Google Scholar]
- 20.Partrick DA, Janik JE, Janik JS, Bensard DD, Karrer FM, Karrer FM. Increased CT scan utilization does not improve the diagnostic accuracy of appendicitis in children. J Pediatr Surg. 2003;38:659–662. doi: 10.1016/jpsu.2003.5017. [DOI] [PubMed] [Google Scholar]
- 21.Garcia Penặ BM, Taylor GA, Lund DP, Mandl KD. Effect of computed tomography on patient management and costs in children with suspected appendicitis. Pediatrics. 1999;104:440–446. doi: 10.1542/peds.104.3.440. [DOI] [PubMed] [Google Scholar]
- 22.Acheson J, Banerjee J. Management of suspected appendicitis in children. Arch Dis child Educ pract Ed. 2010;95:9–13. doi: 10.1136/adc.2009.168468. [DOI] [PubMed] [Google Scholar]
- 23.Lee SL, Walsh AF, Ho HS. Computed tomography and ultrasonography do not improve and may delay the diagnosis and treatment of acute appendicitis. Arch Surg. 2001;136:556–562. doi: 10.1001/archsurg.136.5.556. [DOI] [PubMed] [Google Scholar]
- 24.Van Hoe L, Miserez M. Effectiveness of imaging studies in acute appendicitis: a simplified decision model. Eur J Emerg Med. 2000;7:25–30. doi: 10.1097/00063110-200003000-00005. [DOI] [PubMed] [Google Scholar]
- 25.Schuler JG, Shortsleeve MJ, Goldenson RS, Perez-Rossello JM, Perlmutter RA, Thorsen AI. There a role for abdominal computed tomographic scans in appendicitis? Arch Surg. 1998;133:373–376. doi: 10.1001/archsurg.133.4.373. [DOI] [PubMed] [Google Scholar]
- 26.Lander A. The role of imaging in children with suspected appendicitis: the UK perspective. Pediatr Radiol. 2007;37:5–9. doi: 10.1007/s00247-006-0304-1. [DOI] [PubMed] [Google Scholar]
- 27.Slovis TL. Children, computed tomography radiation dose, and the as low as reasonably achievable (ALARA) concept. Pediatrics. 2003;112:971–972. doi: 10.1542/peds.112.4.971. [DOI] [PubMed] [Google Scholar]
- 28.Arch ME, Frush DP. Pediatric body MDCT: a 5-year follow up survey of scanning parameters used by pediatric radiologists. AJR. 2008;191:611–617. doi: 10.2214/AJR.07.2989. [DOI] [PubMed] [Google Scholar]
- 29.Ahmed BA, Connolly BL, Shroff P, Chong AL, Gordon C, Grant R, Greenberg ML, Thomas KE. Cumulative effective doses from radiologic procedures for pediatric oncology patients. Pediatrics. 2010;126:e851–e858. doi: 10.1542/peds.2009-2675. [DOI] [PubMed] [Google Scholar]
- 30.Mathews JD, Forsythe AV, Brady Z, Butler MW, Goergen SK, Byrnes GB, Giles GG, Wallace AB, Anderson PR, Guiver TA, McGale P, Cain TM, Dowty JG, Bickerstaffe AC, Darby SC. Cancer risk in 680000 people exposed to computed tomography scans in childhood and adolescence: data linkage study of 11 million Australians. BMJ. 2013;346:f2360. doi: 10.1136/bmj.f2360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Doria AS. Optimizing the role of imaging in appendicitis. Pediatr Radiol. 2009;39:S144–S148. doi: 10.1007/s00247-008-1105-5. [DOI] [PubMed] [Google Scholar]
- 32.Wan MJ, Krahn M, Ungar WJ, Caku E, Sung L, Medina LS, Doria AS. Acute appendicitis in young children: cost effectiveness of US versus CT in diagnosis-a Markov decision analytic model. Radiology. 2008;250:378–386. doi: 10.1148/radiol.2502080100. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The study did not contain confidential patient data. No further data will be shared because all the data supporting the findings is contained within the manuscript.