

Abstract
Walking up and down stairs is a common and important activity of daily living. Women with fibromyalgia often show a reduced ability to perform this task.
The objective of this study was to evaluate the test–retest reliability of stair negotiation tasks and to assess the impact of fibromyalgia symptoms on the ability to negotiate stairs.
Forty-two women with fibromyalgia participated in this descriptive correlational study. The relevance of the stair negotiation (both walking up and down) was evaluated by assessing its association with the revised version of the fibromyalgia impact questionnaire (FIQ-R) and other health-related variables. Test–retest reliability was also analyzed. The main outcome measures were time spent walking up and down stairs and impact of fibromyalgia, quality of life, number of falls, weight, and lower limb strength and endurance.
The intraclass correlation coefficient (ICC) for stair descent was 0.929 whereas that for ascent was 0.972. The score in these tests correlated significantly with the total score for the FIQ-R and the score for many of dimensions and symptoms: that is, physical function, overall impact of fibromyalgia, pain, energy, stiffness, restorative sleep, tenderness, self-perceived balance problems, and sensitivity.
Given the importance of the stair negotiation as activity of daily living and the high reliability, both stair ascent and descent tasks may be useful as outcome measures in studies on patients with fibromyalgia.
Keywords: chronic pain, falls, fear of falling, pain, stair ascent, stair descent
1. Introduction
Fibromyalgia (FM) is a chronic disease characterized by widespread pain and several associated symptoms, such as fatigue, non-restorative sleep, mood alterations, and poor health-related quality of life (HRQoL).[1,2] FM is a complex disorder that affects both physical and psychological health. These 2 components of health are often related, but the impact on physical performance is usually greater.[3] Thus, physical fitness is associated with a number of FM symptoms, including pain, anxiety, and depression.[4,5] Also, FM has an impact on fear of falling and on the number of falls due to a poor objective and subjective sense of balance.[6]
All these FM-related impairments and symptoms reduce HRQoL and limit the performance of activities of daily living. The fibromyalgia impact questionnaire (FIQ)[7] and its revised version (FIQ-R)[8] are 2 commonly used tools for assessing the impact of the disease. These 2 questionnaires support the relevance of stair ascent and descent by including a question about the capacity to climb stairs and the difficulty of performing the task. Going up and down stairs is a common and challenging activity of daily living that can increase the risk of falls and subsequent injury. Most falls among women with FM occur while walking or negotiating stairs.[9]
In addition to assessment using questionnaires, previous studies used physical tests in which patients with FM had to climb a number of steps as quickly as possible.[10–14] In 2 studies, women with FM had to climb 10 steps either empty handed or carrying a load.[12,13] In the first of these studies, the performance in the stair ascent was assessed to evaluate the effects of a training program aimed at proving that physical exercise prevents progressive loss of performance in this task.[13] The second focused on detecting differences in motor patterns between women with FM and healthy controls while using stairs.[12] Three other studies utilized a test involving stair ascent to compare the performance and/or response of FM patients and healthy controls to a training program.[10,11,14] All 3 studies concluded that patients with FM needed more time to complete the stair climbing task. However, to the best of our knowledge, no study has used a test that includes stair descent in FM patients.
Several studies have used different tests to evaluate the ability to descend stairs in different populations, such as patients with osteoarthritis of the knee,[15] adults who are functionally limited,[16] and older adults.[17,18] The number of stairs and the instructions are very variable. Most studies used a flight of stairs comprising between 7[15] to 26 steps[16] taken at the preferred speed[15,17] or “as fast as possible”.[16,18] Although many studies evaluated the reliability and validity of different stair climbing tests in several populations, none focused on people with FM. However, few studies have evaluated the test–retest reliability of stair descent in other populations. Among others, Leitner et al[17] evaluated the reliability of vertical ground reaction forces during stair ascent/descent in elderly subjects, Manini et al,[18] validated a scale for evaluating modifications in the stair ascent/descent task in older adults, and Lin et al[19] assessed the reliability of a test in which elderly participants with knee and hip osteoarthritis were asked to ascend and descend 4 steps.
For FM studies, the most common flight length is 10 steps.[10,13,14] Similarly, the most common instruction is “as quickly and safely as you can”.[10,13,14] Regarding stair descent, no study has examined this task in women with FM. Women with FM have an increased risk of falling,[6] which is higher during stair descent because adequate muscular output from the leg-extensor is needed to control the body's center of mass while stepping down.[20] Therefore, the most adequate and safe instruction for descent should be “at your naturally preferred comfortable pace”. This instruction should reduce unnecessary risk of falling during performance of the test.
The main objective of the current study was to evaluate the association between stair negotiation (walking up and down stairs) and impact of FM, quality of life, and physical conditioning. This study also aims to assess the test–retest reliability of stair negotiation tasks.
2. Methods
2.1. Participants
For this descriptive correlational study, sample size calculation indicated that 40 subjects and 2 observations per subject would achieve 98% power for detecting an intraclass correlation of 0.90 (i.e., excellent reliability according to Munro et al[21]) under the alternative hypothesis when the intraclass correlation under the null hypothesis is 0.70 (good reliability according to Munro et al,[21]), with a significance level of 0.05. However, to account for potential dropouts or women who were not able to climb 10 stairs, 2 additional participants were included.
All participants were recruited from the local FM association of Palencia (Spain) in October, 2015. The inclusion criteria were: woman and diagnosed with FM by a rheumatologist according to the criteria of the American College of Rheumatology,[22,23] aged between 30 and 75 years, diagnosed with osteoarthritis, and not suffering from an acute musculoskeletal injury (fracture, sprains, etc.).
The final sample comprised 42 women with FM. All provided written informed consent according to the updated Declaration of Helsinki. The study was approved by the Bioethical Committee of the University of Extremadura (Spain).
2.2. Procedures
First, a Tanita BC-418 (Tanita Corp., Tokyo, Japan) MA body composition analyzer was used to measure the weight of the participants. All tasks were performed wearing weight bearing insoles coupled to functional assessment of biomechanics (FAB) system (Biosyn Systems, Inc.; Surrey, BC, Canada), which allows the researcher to ascertain when the foot is on the ground and when is in the air.
Pain at 18 tender points was evaluated using an algometer (PainTest FPX 25). Two questionnaires were used to evaluate the impact of FM and quality of life: the FIQ-R and the five-level version of the EuroQoL five-dimension (EQ-5D-5L).[24] The first evaluates the impact of FM and addresses the limitations of the FIQ while retaining the essential properties of the original instrument.[8] The Spanish version of FIQ-R was validated by Salgueiro et al.[25] This questionnaire includes 3 domains: function (0–30), overall impact (0–20), and symptom (0–50). The sum of those 3 domains is the total score (0–100). Higher scores would mean higher impact of FM. The symptom domain can also be divided into 10 symptoms (pain, energy, stiffness, restorative sleep, depression, anxiety, memory, tenderness, balance troubles, and sensitiveness). The EQ-5D-5L is a widely-used generic instrument for describing and evaluating HRQoL.
Ten steps of stair ascent was selected because this is the most common flight length used in previous studies of women with FM.[10,13,14] The instruction for ascent was “as quickly and safely as you can”, which is the instruction given by previous studies.[10,13,14] To preserve coherence with the stair ascent task, the number of stairs to be descended was also 10. To reduce the risk of falling, the instruction for descent was “at your naturally preferred comfortable pace”.
Participants performed the tasks twice, with a 5-minute rest in between. A light warm-up including walking and joint mobility was carried out for 5 minutes. Participants could use handrails if required. They could also start the task with either the right or left foot.
After completing the tasks, the women rested for 5 minutes and then completed the 30 seconds chair stand test,[26] which is a commonly used test for women with FM; the test assesses the strength and endurance of the lower limbs. The participants then rested for 10 minutes before completing the 6 minutes walk test,[27] a test used widely to assess women with FM and elderly subjects.
2.3. Statistical analysis
Time spent ascending and descending the stair was recorded. Two trials were performed and the best was used for validation analysis. This time was then normalized according to age.
Relative reliability was estimated using the intraclass correlation coefficient two-way random effects model analysis of variance (ICC 2.2) with 95% confidence intervals across the 2 test repetitions.[28] Absolute reliability was determined by calculating the standard error of measurement (SEM) as follows:  ,[28] where SD is the mean standard deviation of the 2 repetitions. The smallest real difference (SRD) was calculated as
,[28] where SD is the mean standard deviation of the 2 repetitions. The smallest real difference (SRD) was calculated as  .[28]
.[28]
Both SEM and SRD were transformed to percentages to facilitate comparison with future studies. These percentages were calculated as follows: SEM% = (SEM/mean time for 2 repetitions) × 100; and SRD% = SRD/(mean time for 2 repetitions) × 100.
Correlations between the time required to ascend and descend the 10 steps and the scores for FIQ-R, including dimensions 1 (functional domain) and 2 (overall impact domain) of the FIQ-R and the total FIQ-R score, were calculated. Dimension 3 of the FIQ-R (symptom domain) was divided into the 10 symptoms evaluated by the FIQ-R and then, the correlation with the time taken to ascend/descend the steps was tested.
Finally, the association between the time required in the negotiation of stairs tasks and the utility index of the EQ-5D, the number of falls in the last year, the number of repetitions recorded in the 30 seconds chair stand test, the number of meters walked in the 6 minutes walk test, and weight were tested using bivariate correlations. All statistical analyses were performed using SPSS (IBM-SPSS, Chicago, IL) (v21).
3. Results
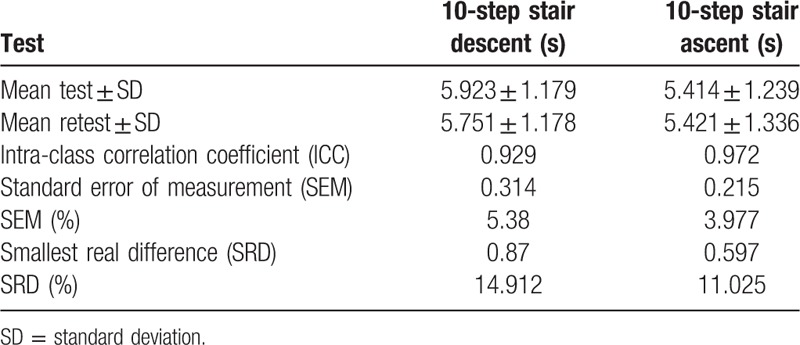
The main characteristics of the participants are listed in Table 1. The mean age of the participants was 50.24 (9.31) and the mean duration of FM symptoms was 14.00 (6.91) years. The mean score in the FIQ-R was 46.98 (18.98), which means “moderate” FM. The mean body mass index was 25.56 (2.77) kg/m2. Table 2 shows the test–retest reliability for stair ascent and descent. The mean time for stair descent was 5.923 (standard deviation [SD] 1.179) seconds, which fell to 5.751 (SD 1.178) seconds in the retest. The mean time for the first stair ascent was 5.414 (SD 1.239) seconds, which increased to 5.421 (SD 1.336) seconds on the retest. The ICC for stair descent was 0.929 and that for ascent was 0.972. Regarding absolute reliability for stair descent, the SEM and the SRD were 0.314 (5.380%) and 0.870 (14.912%), respectively. The 10-step stair ascent was more reliable than the descent, with a SEM of 0.215 (3.977%) and a SRD of 0.597 (11.025%).
Table 1.
Main characteristics of the participants (N = 42).
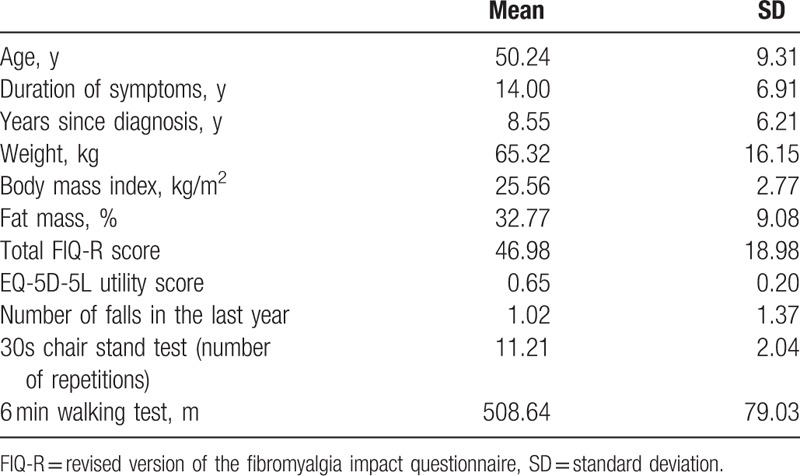
Table 2.
Test–retest reliability of stair negotiation tasks in women with fibromyalgia (n = 42).
The correlations between the time taken for stair ascent and descent and the FIQ-R are listed in Table 3. Stair descent was significantly associated with the total FIQ-R score, physical function, overall impact, pain, energy, stiffness, restorative sleep, tenderness, and self-perceived balance troubles. Stair ascent was significantly correlated with the total score, physical function, overall impact, pain, energy, self-perceived balance problems, and sensitiveness.
Table 3.
Pearson correlations between stair negotiation tasks and FIQ-R.
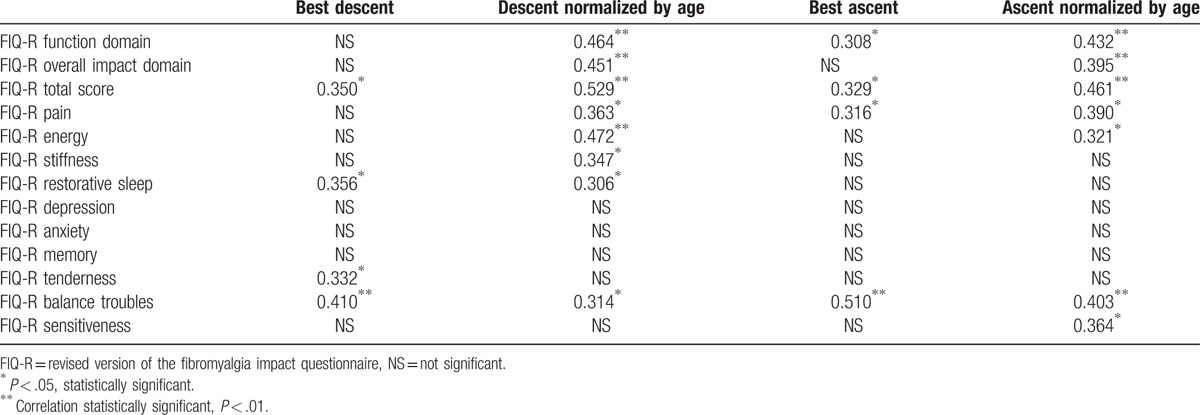
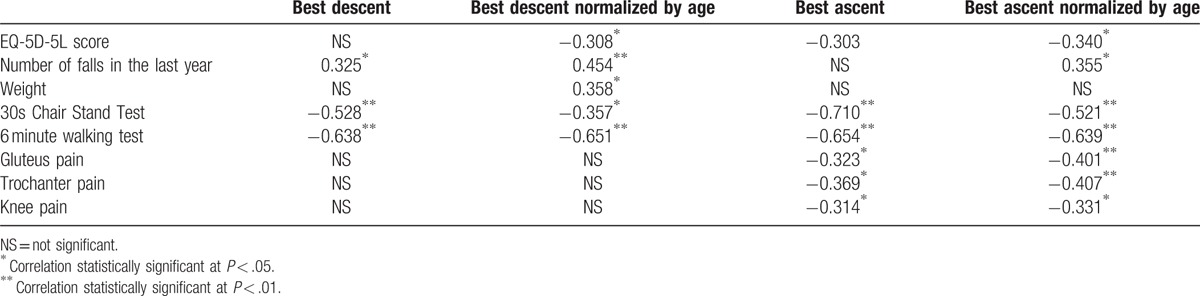
Table 4 shows the correlations between the stair negotiation tasks and different variables. Stair descent was significantly associated with HRQoL (as assessed by the EQ-5D-5L), the number of falls in the last year, weight, and the 2 test scores for physical fitness: the 30 seconds chair stand test and the 6 minutes walk test. Stair ascent correlated significantly with HRQoL, number of falls in the last year, the score in the 2 physical fitness tests, and pain in the gluteus, trochanter, and knee (evaluated using an algometer).
Table 4.
Pearson correlation between stair negotiation tasks and other measurements.
4. Discussion
This study showed that the reliability of stair ascent and descent tasks in women with FM is excellent according to the classification set by Munro et al,[21] (ICC > 0.9). The scores for both ascent and descent were significantly associated with the results of 2 other physical fitness tests: the 30 seconds chair stand test and the 6 minutes walk test. This was an inverse association, meaning that longer time required to ascend/descend a flight of 10 steps is associated with a lower number of repetitions in the 30 seconds chair stand test and shorter distance covered in 6 minutes.
A previous study found that the results of the timed up and go test (TUG) is statistically associated with a history of falls in men but not in women.[29] In that test, participants are asked to sit on a chair, stand up, walk to a mark, return to the chair, and sit down again.[30] However, based on the previous scientific literature regarding FM and falls, it was expected that the score for stairs negotiation tasks would correlate with the number of falls. We found that the stair descent test correlated more precisely with the number of falls than the stair ascent test, suggesting that descending a flight of 10 steps at a comfortable speed is more closely associated with the number of falls than stair ascent at the fastest speed. This does not necessarily contradict the study by Rutledge et al,[9] who reported that ascent more often contributes to falls than descent. Thus, the hypothesis that stair descent is a greater contributor to falls should be confirmed by future studies.
Regarding the association between stair negotiation tasks and FIQ-R, almost every correlation improved when the time was normalized by age. Only 3 symptoms (i.e., depression, anxiety, and memory) were not significantly related to stair ascent or descent. Since the main symptom of FM is pain, this was evaluated using the FIQ-R and an algometer. The results showed that pain, as assessed using the FIQ-R, showed a significant correlation with descent normalized by age, and with both normalized and non-normalized ascent. On the other hand, local pain, as assessed using an algometer, correlated significantly only with normalized and non-normalized stair ascent (note that in this case the correlation was an inverse one because higher scores mean higher tolerance to pain). A possible explanation for this may be speed of performance. The stair ascent task was performed “as fast and safely as they could”; under these conditions pain may play a bigger role than it does when descending a flight of ten steps at “a comfortable speed”.
According to Tables 3 and 4, stair descent evaluation may provide very valuable information. First, descent correlated significantly with tenderness and stiffness; second, it showed a better correlation with the function domain, the overall impact domain, the total FIQ-R score, and the number of falls in the last year than the ascent portion of the test. Therefore, including stair descent in the physical evaluation of women with FM is justified.
Data were collected using weight bearing insoles. This may increase the reliability of the test as it removed any errors introduced by a rater using a manual chronometer.[31] According to the FIQ score, the severity of FM was “moderate”: between 39 and 59.[32] The use of handrails was not controlled in the present study, although most previous studies provided directions about their use;[18,33] however, handrails do not appear to affect test performance times.[15,34] Thus, participants were instructed to climb 10 steps “as fast and safely as they could” and were allowed to use the handrails if required for safety reasons. Similarly, participants were instructed to descend the flight “at your naturally preferred comfortable pace”. Since the objective of this task is to assess the naturally preferred comfortable pace, no further instruction should be given as it could alter the natural pattern and pace.
There are 2 main limitations of this study. First, the age-related inclusion criteria allowed a wide range of ages, that is, between 30 and 75. Given the relevance of age to physical fitness, future studies should assess the performance in the tasks according to more restrictive age-related criteria, or should enroll a larger cohort that allows different age ranges to be studied. Second, the reliability parameters may be increased by the use of weight bearing insoles. Future studies should consider that using a manual chronometer is less reliable than using weight bearing insoles.
In conclusion, the stair negotiation tasks (both walking up and down) are safe and reliable for women with FM. The tasks involved participants ascending and descending of a flight of 10 stairs “as quickly and safely as they can” and at their “naturally preferred comfortable pace”, respectively. Given that negotiating stairs is an important activity of daily living, these tests may be used for both rehabilitation and research purposes since the results correlate significantly with the number of falls, HRQoL (assessed using EQ-5D-5L), weight, strength of the lower limb, endurance, pain, physical function, overall impact of FM, energy, stiffness, restorative sleep, tenderness, self-reported balance, and sensitiveness.
Acknowledgments
The authors thank Pilar Fernández and members of the Association of fibromyalgia and chronic fatigue, Palencia, Spain, for help and support.
Footnotes
Abbreviations: EQ-5D-5L = five-level version of the EuroQoL five-dimension questionnaire, FAB = functional assessment of biomechanics, FIQ = fibromyalgia impact questionnaire, FIQ-R = revised version of fibromyalgia impact questionnaire, FM = fibromyalgia, HRQoL = health-related quality of life, ICC = intraclass correlation coefficient, SEM = standard error of measurement, SRD = smallest real difference, TUG = timed up and go test.
Source of Funding: The current study has been co-funded by the Spanish Ministry of Economy and Competitiveness with the reference DEP2012-39828 and DEP2015-70356. The author DCM is supported by a grant from the Spanish Ministry of Education, Culture and Sport (FPU14/01283). The funders had no role in study design, data collection, and analysis, decision to publish, or preparation of the manuscript.
The authors have no conflicts of interest to disclose.
References
- [1].Wolfe F. Editorial: the status of fibromyalgia criteria. Arthritis Rheumatol 2015;67:330–3. [DOI] [PubMed] [Google Scholar]
- [2].Segura-Jimenez V, Alvarez-Gallardo IC, Carbonell-Baeza A, et al. Fibromyalgia has a larger impact on physical health than on psychological health, yet both are markedly affected: the al-Ándalus project. Semin Arthritis Rheum 2014;44:563–70. [DOI] [PubMed] [Google Scholar]
- [3].Segura-Jimenez V, Alvarez-Gallardo IC, Carbonell-Baeza A, et al. Fibromyalgia has a larger impact on physical health than on psychological health, yet both are markedly affected: the al-Andalus project. Semin Arthritis Rheum 2015;44:563–70. [DOI] [PubMed] [Google Scholar]
- [4].Carbonell-Baeza A, Aparicio VA, Sjostrom M, et al. Pain and functional capacity in female fibromyalgia patients. Pain Med 2011;12:1667–75. [DOI] [PubMed] [Google Scholar]
- [5].Sener U, Ucok K, Ulasli AM, et al. Evaluation of health-related physical fitness parameters and association analysis with depression, anxiety, and quality of life in patients with fibromyalgia. Int J Rheum Dis 2016;19:763–72. [DOI] [PubMed] [Google Scholar]
- [6].Collado-Mateo D, Gallego-Diaz JM, Adsuar JC, et al. Fear of falling in women with fibromyalgia and its relation with number of falls and balance performance. BioMed Res Int 2015;2015:589014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Bennett R. The Fibromyalgia impact questionnaire (FIQ): a review of its development, current version, operating characteristics and uses. Clin Exp Rheumatol 2005;23Suppl:S154–62. [PubMed] [Google Scholar]
- [8].Bennett RM, Friend R, Jones KD, et al. The Revised Fibromyalgia Impact Questionnaire (FIQR): validation and psychometric properties. Arthritis Res Ther 2009;11:R120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Rutledge DN, Martinez A, Traska TK, et al. Fall experiences of persons with fibromyalgia over 6 months. J Adv Nurs 2013;69:435–48. [DOI] [PubMed] [Google Scholar]
- [10].Valkeinen H, Hakkinen A, Alen M, et al. Physical fitness in postmenopausal women with fibromyalgia. Int J Sports Med 2008;29:408–13. [DOI] [PubMed] [Google Scholar]
- [11].Huijnen IP, Verbunt JA, Meeus M, et al. Energy expenditure during functional daily life performances in patients with fibromyalgia. Pain Pract 2015;15:748–56. [DOI] [PubMed] [Google Scholar]
- [12].Collado Mateo D, Adsuar JC, Olivares PR, et al. Performance of women with fibromyalgia in walking up stairs while carrying a load. Peer J 2016;4:e1656. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Tomas-Carus P, Gusi N, Hakkinen A, et al. Eight months of physical training in warm water improves physical and mental health in women with fibromyalgia: a randomized controlled trial. J Rehabil Med 2008;40:248–52. [DOI] [PubMed] [Google Scholar]
- [14].Valkeinen H, Alen M, Hannonen P, et al. Changes in knee extension and flexion force, EMG and functional capacity during strength training in older females with fibromyalgia and healthy controls. Rheumatology (Oxford) 2004;43:225–8. [DOI] [PubMed] [Google Scholar]
- [15].McCarthy CJ, Oldham JA. The reliability, validity and responsiveness of an aggregated locomotor function (ALF) score in patients with osteoarthritis of the knee. Rheumatology (Oxford) 2004;43:514–7. [DOI] [PubMed] [Google Scholar]
- [16].Topp R, Boardley D, Morgan AL, et al. Exercise and functional tasks among adults who are functionally limited. West J Nurs Res 2005;27:252–70. [DOI] [PubMed] [Google Scholar]
- [17].Leitner M, Schmid S, Hilfiker R, et al. Test-retest reliability of vertical ground reaction forces during stair climbing in the elderly population. Gait Posture 2011;34:421–5. [DOI] [PubMed] [Google Scholar]
- [18].Manini TM, Cook SB, VanArnam T, et al. Evaluating task modification as an objective measure of functional limitation: repeatability and comparability. J Gerontol A Biol Sci Med Sci 2006;61:718–25. [DOI] [PubMed] [Google Scholar]
- [19].Lin YC, Davey RC, Cochrane T. Tests for physical function of the elderly with knee and hip osteoarthritis. Scand J Med Sci Sports 2001;11:280–6. [DOI] [PubMed] [Google Scholar]
- [20].Bosse I, Oberlander KD, Savelberg HH, et al. Dynamic stability control in younger and older adults during stair descent. Hum Mov Sci 2012;31:1560–70. [DOI] [PubMed] [Google Scholar]
- [21].Munro B, Visintainer M, Page E. Statistical Methods for Health Care Research. Philadelphia: Lippincott Williams & Wilkins; 1986. [Google Scholar]
- [22].Wolfe F, Smythe HA, Yunus MB, et al. The American College of Rheumatology 1990 criteria for the classification of fibromyalgia. Report of the multicenter criteria committee. Arthritis Rheum 1990;33:160–72. [DOI] [PubMed] [Google Scholar]
- [23].Wolfe F, Clauw DJ, Fitzcharles MA, et al. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res (Hoboken) 2010;62:600–10. [DOI] [PubMed] [Google Scholar]
- [24].Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res 2011;20:1727–36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Salgueiro M, Garcia-Leiva JM, Ballesteros J, et al. Validation of a Spanish version of the Revised Fibromyalgia Impact Questionnaire (FIQR). Health Qual Life Outcomes 2013;11:132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Park DC, Glass JM, Minear M, et al. Cognitive function in fibromyalgia patients. Arthritis Rheum 2001;44:2125–33. [DOI] [PubMed] [Google Scholar]
- [27].Rikli RE, Jones CJ. Development and validation of a functional fitness test for community-residing older adults. J Aging Phys Activ 1999;7:129–61. [Google Scholar]
- [28].Weir JP. Quantifying test-retest reliability using the intraclass correlation coefficient and the SEM. J Strength Cond Res 2005;19:231–40. [DOI] [PubMed] [Google Scholar]
- [29].Thrane G, Joakimsen RM, Thornquist E. The association between timed up and go test and history of falls: the Tromso study. BMC Geriatr 2007;7:1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].Podsiadlo D, Richardson S. The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc 1991;39:142–8. [DOI] [PubMed] [Google Scholar]
- [31].Collado Mateo D, Dominguez Munoz FJ, Adsuar JC, et al. Reliability of the timed-up and go test in women with fibromyalgia. Rehabil Nurs 2016;doi: 10.1002/rnj.307. [Epub ahead of print]. [DOI] [PubMed] [Google Scholar]
- [32].Bennett RM, Bushmakin AG, Cappelleri JC, et al. Minimal clinically important difference in the fibromyalgia impact questionnaire. J Rheumatol 2009;36:1304–11. [DOI] [PubMed] [Google Scholar]
- [33].Naimark MB, Kegel G, O’Donnell T, et al. Knee function assessment in patients with meniscus injury: a preliminary study of reproducibility, response to treatment, and correlation with patient-reported questionnaire outcomes. Orthop J Sports Med 2014;2:2325967114550987. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [34].Bassey EJ, Fiatarone MA, O’Neill EF, et al. Leg extensor power and functional performance in very old men and women. Clin Sci 1992;82:321–7. [DOI] [PubMed] [Google Scholar]