

Abstract
Ample evidence strongly supports the fact that periodontal disease is a major risk factor for various systemic diseases namely cardio-vascular disease, diabetes mellitus, etc. Recently, investigators focussed on exploring the link between chronic periodontitis (CP) and erectile dysfunction (ED) by contributing to the endothelial dysfunction. Both the diseases share common risk factors. Various studies conducted in different parts of the world in recent years reported the evidence linking this relationship as well as improvement in ED with periodontal treatment. Systemic exposure to the periodontal pathogen and periodontal infection-induced systemic inflammation was thought to associate with these conditions. The objective of this review was to highlight the evidence of the link between CP and ED and the importance of oral health in preventing the systemic conditions.
KEYWORDS: Chronic periodontitis, erectile dysfunction, oral health, periodontal medicine
INTRODUCTION
Erectile dysfunction (ED) also known as impotence was described by the National Institutes of Health Consensus Panel on Impotence as a persistent or recurrent inability to have sufficient erection for satisfactory sexual performance.[1] ED is a major problem worldwide. It is estimated to affect more than 150 million men worldwide and affects the quality of life of patients.[1,2] It can cause stress, affect self-confidence and contribute to problems in the relationship with their partners. ED is usually experienced at the age ≥40 years.[3] In Massachusetts, the prevalence of ED was 52%, with 5–15% of complete impotence tripling in the age range of 40–70-year-old men.[2]
Periodontitis is a chronic inflammatory multifactorial disease commonly caused by plaque biofilm, involving the supporting structures of the teeth and may result in the loss of dentition if left untreated. Globally, around 5–15% of patients with 34–45 years of age suffer from severe periodontitis.[4] Chronic periodontitis (CP) has been demonstrated as a significant risk factor for various systemic diseases such as coronary heart disease, adverse pregnancy outcomes, diabetes mellitus and respiratory disease. Systemic exposure to periodontal pathogen and periodontal infection-induced systemic inflammation was thought to be associated with these systemic conditions.[5]
Both diseases are multifactorial and share common risk factors (smoking, diabetes mellitus, and cardiac diseases) and both can predispose to endothelial dysfunction.[6] Hence, studies in the recent years have tried to explore the link between periodontal disease and ED by contributing to an increased level of endothelial dysfunction.[7,8] However, the evidence is inconsistent, and hence this review highlights the link between ED and CP. It would be beneficial to increase awareness among general practitioners and the public regarding the association between two diseases.
POSSIBLE LINKING PATHWAYS FOR THE ASSOCIATION BETWEEN CHRONIC PERIODONTITIS AND ERECTILE DYSFUNCTION
ED is a multifactorial condition, which can be caused by the organic (hormonal, vascular, drug induced) or psychological reasons, or a combination of both.[9] However, the most common cause is the vascular disease. The exact pathway is still unknown. Following mechanisms have been proposed to explain this relationship.
Endothelial dysfunction
Endothelial dysfunction refers to various pathological conditions, such as alteration in anticoagulant and anti-inflammatory features of the endothelium, impaired vascular growth modulation, and dysregulation of vascular remodelling.
Atherosclerosis is the underlying pathology of the cardiac disease. Evidence suggests that atherosclerosis arises from the combination of endothelial dysfunction and inflammation. The blockage of the cavernosal arteries by atherosclerosis as well as the impairment of endothelial function or smooth muscle relaxation may result in the ED.[10] Endothelial dysfunction is the key event in the pathophysiology of ED, and this was also found in other vascular beds, in males affected with penile vascular dysfunction.[11] Atherosclerosis begins first in the small vessels such as the penile vasculature, and later in larger arteries such as the coronaries.
Advanced age is a strong predictor of endothelial dysfunction in elderly patients.[12] In ageing males, not only CP is a source of inflammation that may damage penile endothelial function, but some other common pathological conditions, such as smoking, hypertension and obesity, can also induce endothelial dysfunction.
Inflammation
Increased risk of endothelial dysfunction may be associated with high levels of inflammatory mediators such as interleukin (IL)-6, IL-8, tumour necrosis factor-alpha (TNF-α), and IL-1.[13,14] TNF-α plays a key role in the induction of endothelial dysfunction.[15] CP also induce these local and systemic elevation of proinflammatory cytokines, such as TNF-α, IL-1 and IL-6.[16,17] Furthermore, multiple studies have shown a reduction in TNF-α levels after successful periodontal treatment.[18,19] It was also evident that significant higher plasma levels of TNF-α were associated with moderate to severe ED[13,20] owing to their known effects on the vasculature.[21]
Oxidative stress
Endothelial dysfunction resulted from chronic inflammation is associated with an increase in reactive oxygen species (ROS).[22,23] This excess production of ROS resulted in the increased inactivation in nitric oxide (NO), and the damage to the antioxidant system may contribute to endothelial dysfunction in patients with periodontitis.[8] In a study on rat model, it was reported that the periodontitis-induced mild systemic inflammation resulted in the decreased expression and activity of endothelial NO synthase in penile cavernous tissue.[24]
Periodontal pathogens
Periodontal microorganism such as Porphyromonas gingivitis or their toxin could gain access into the blood circulation which may directly invade the arterial wall and subsequently lead to vascular inflammation, atherosclerosis and directly affect the endothelial function.[25]
EVIDENCE LINKING ORAL HEALTH TO ERECTILE DYSFUNCTION
Multiple studies on human have been conducted in various parts of world to explore this relationship and reported the potential association between CP and ED in past few years [Table 1].
Table 1.
Summary of human studies explored the link between CP and ED
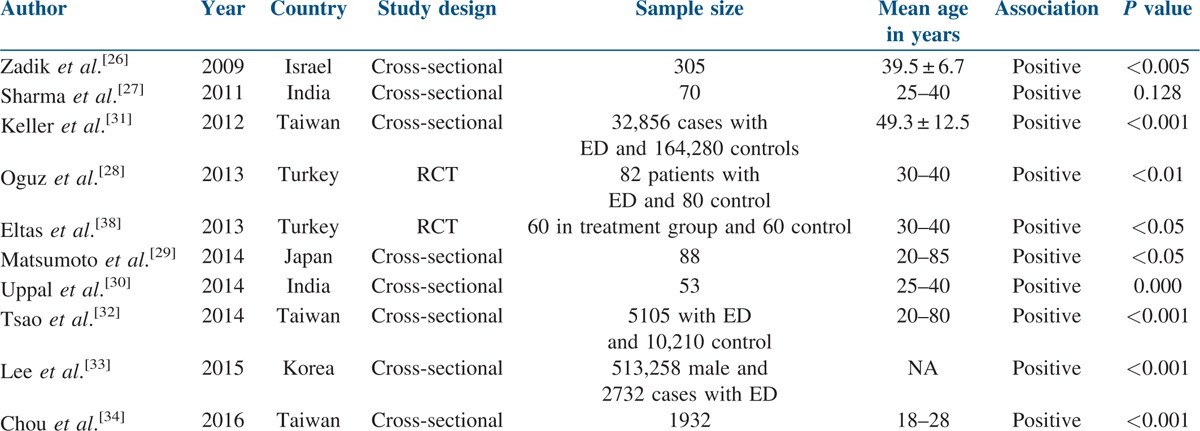
First preliminary study[26] in 2009 explored the link between ED and CP, reported the significantly higher prevalence of CP in men with mild ED and moderate to severe ED in comparison to men without ED. The authors concluded that ED might be associated with CP. The finding of this preliminary study was supporting the theories that associate these conditions, with systemic inflammation, endothelial dysfunction and atherosclerosis.
Sharma et al.[27] studied the ED patients diagnosed clinically with penile colour Doppler. Prevalence for CP was increased continuously from the mild to severe vasculogenic ED group and highest among severe vasculogenic ED group. Non-statistically significant positive correlation was found between CP and vasculogenic ED. Vascular insufficiency was found in two out of five patients randomly selected for cardiac colour Doppler.
In a single-blinded randomized controlled trial (RCT), Oguz et al.[28] reported that the ED was 3.29 times more likely in severe CP patients than periodontal healthy men and a significantly high association between ED and the severity of CP. The author suggested that it will be of benefit to consider periodontal disease as a causative clinical condition of ED in such patients.
Matsumoto et al.[29] found that ED is related to the damage caused by endothelial dysfunction and the systematic inflammatory changes associated with CP and suggested that dental health is important as a preventive medicine for ED.
Uppal et al.,[30] in a clinical cross-sectional study, found a positive correlation of ED with CP and statistically significant mean difference in radiographic bone loss in moderate and severe ED group when compared to mild ED group.
Data from the nationwide population-based, cohort studies[31,32,33] indicated the strong association of CP with ED. CP plays a key role in the pathological process of ED and is a risk factor that is independent of other morbidities and risk factors for ED. Furthermore, the much stronger association was found among the younger (<30 years of age)[31,33] population and also in older men of more than 59 years[32] and more than 69 years.[31] Recently a study,[34] in younger age group (18–28 years) highlights the significance of oral hygiene might influence sexual life even in the young male population.
Systematic reviews
Furthermore, evidence from recent systematic reviews[35,36] and meta-analysis[37] of available literature also revealed the positive association between CP and ED. The pooled odd-ratio of the included studies in meta-analysis[37] showed that patients with ED were 3.07-fold more likely than controls to be diagnosed with CP. It was emphasised that physicians should refer patients with ED to oral health care providers for a comprehensive oral evaluation and treatment. Dentists and physicians should collaborate to manage and monitor patients with either CP or ED because of their potential association not only with each other but also with more serious systemic diseases.
EFFECT OF PERIODONTAL THERAPIES ON ERECTILE DYSFUNCTION
In an RCT[38] conducted to evaluate the direct effect of periodontal treatment on ED, highlighted a statistically significant higher improvement in periodontal health and IIEF scores in the intervention group than that in the control group (P < 0.05) at 3 months. However, this study does not report the effect of periodontal treatment on the level of TNF-α but the results of this study provide evidences that periodontal treatment can help to reduce ED. Successful periodontal therapy has been also demonstrated significantly improvement in the endothelial function[39,40] in patients with associated hypertension or cardiovascular disease as well as decreases the levels of TNF-α in patients with progressive periodontitis.[18] Additionally, the lower association was reported in patients receiving a gingivectomy or periodontal flap surgery and ED than those without any treatment at all for CP.[31] The dental extractions attenuated the development of ED in CP induced inflammation of all age groups except younger population, as the dental extraction procedure involves the reduction of inflamed tissue.[32]
CONCLUSION
In the light of available literature, evidence indicated positive link in CP and ED. It was also suggested that CP should be considered risk factors for ED and treatment of CP might be helpful in the improvement of ED. The importance of oral health should be given by dentist and physician as a preventive medicine for not only ED but also for more serious systemic diseases in the best interest of patient health. Patients should be advised to visit dentist regularly for oral health screening. Further, well-designed multicentre clinical trials with long-term follow-up are required to draw stronger evidence.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Lue TF, Giuliano F, Montorsi F, Rosen RC, Andersson KE, Althof S, et al. Summary of the recommendations on sexual dysfunctions in men. J Sex Med. 2004;1:6–23. doi: 10.1111/j.1743-6109.2004.10104.x. [DOI] [PubMed] [Google Scholar]
- 2.Feldman HA, Goldstein I, Hatzichristou DG, Krane RJ, McKinlay JB. Impotence and its medical and psychosocial correlates: Results of the Massachusetts Male Aging Study. J Urol. 1994;151:54–61. doi: 10.1016/s0022-5347(17)34871-1. [DOI] [PubMed] [Google Scholar]
- 3.Krane RJ, Goldstein I, Saenz de Tejada I. Impotence. N Engl J Med. 1989;321:1648–59. doi: 10.1056/NEJM198912143212406. [DOI] [PubMed] [Google Scholar]
- 4.Petersen PE. The World Oral Health Report 2003: Continuous improvement of oral health in the 21st century − The approach of the WHO Global Oral Health Programme. Community Dent Oral Epidemiol. 2003;31(Suppl 1):3–23. doi: 10.1046/j..2003.com122.x. [DOI] [PubMed] [Google Scholar]
- 5.Seymour GJ, Ford PJ, Cullinan MP, Leishman S, Yamazaki K. Relationship between periodontal infections and systemic disease. Clin Microbiol Infect. 2007;13(Suppl 4):3–10. doi: 10.1111/j.1469-0691.2007.01798.x. [DOI] [PubMed] [Google Scholar]
- 6.Gimbrone MA., Jr Vascular endothelium: An integrator of pathophysiologic stimuli in atherosclerosis. Am J Cardiol. 1995;75:67–70B. doi: 10.1016/0002-9149(95)80016-l. [DOI] [PubMed] [Google Scholar]
- 7.Blum A, Kryuger K, Mashiach-Eizenberg M, Tatour S, Vigder F, Laster Z, et al. Periodontal care may improve endothelial function. Eur J Intern Med. 2007;18:295–8. doi: 10.1016/j.ejim.2006.12.003. [DOI] [PubMed] [Google Scholar]
- 8.Higashi Y, Goto C, Jitsuiki D, Umemura T, Nishioka K, Hidaka T, et al. Periodontal infection is associated with endothelial dysfunction in healthy subjects and hypertensive patients. Hypertension. 2008;51:446–53. doi: 10.1161/HYPERTENSIONAHA.107.101535. [DOI] [PubMed] [Google Scholar]
- 9.Heidelbaugh JJ. Management of erectile dysfunction. Am Fam Physician. 2010;81:305–12. [PubMed] [Google Scholar]
- 10.Kirby M, Jackson G, Simonsen U. Endothelial dysfunction links erectile dysfunction to heart disease. Int J Clin Pract. 2005;59:225–9. doi: 10.1111/j.1742-1241.2005.00453.x. [DOI] [PubMed] [Google Scholar]
- 11.Kaiser DR, Billups K, Mason C, Wetterling R, Lundberg JL, Bank AJ. Impaired brachial artery endothelium-dependent and −independent vasodilation in men with erectile dysfunction and no other clinical cardiovascular disease. J Am Coll Cardiol. 2004;43:179–84. doi: 10.1016/j.jacc.2003.07.042. [DOI] [PubMed] [Google Scholar]
- 12.Aversa A, Bruzziches R, Francomano D, Natali M, Gareri P, Spera G. Endothelial dysfunction and erectile dysfunction in the aging man. Int J Urol. 2010;17:38–47. doi: 10.1111/j.1442-2042.2009.02426.x. [DOI] [PubMed] [Google Scholar]
- 13.Vlachopoulos C, Aznaouridis K, Ioakeimidis N, Rokkas K, Vasiliadou C, Alexopoulos N, et al. Unfavourable endothelial and inflammatory state in erectile dysfunction patients with or without coronary artery disease. Eur Heart J. 2006;27:2640–8. doi: 10.1093/eurheartj/ehl341. [DOI] [PubMed] [Google Scholar]
- 14.Eaton CB, Liu YL, Mittleman MA, Miner M, Glasser DB, Rimm EB. Aretrospective study of the relationship between biomarkers of atherosclerosis and erectile dysfunction in 988 men. Int J Impot Res. 2007;19:218–25. doi: 10.1038/sj.ijir.3901519. [DOI] [PubMed] [Google Scholar]
- 15.Holm T, Aukrust P, Andreassen AK, Ueland T, Brosstad F, Frøland SS, et al. Peripheral endothelial dysfunction in heart transplant recipients: Possible role of proinflammatory cytokines. Clin Transpl. 2000;14:218–25. doi: 10.1034/j.1399-0012.2000.140307.x. [DOI] [PubMed] [Google Scholar]
- 16.De Nardin E. The role of inflammatory and immunological mediators in periodontitis and cardiovascular disease. Ann Periodontol. 2001;6:30–40. doi: 10.1902/annals.2001.6.1.30. [DOI] [PubMed] [Google Scholar]
- 17.Noack B, Genco RJ, De Nardin E. Relationship between periodontal disease status, periodontal organisms, and C-reactive protein. J Periodontol. 2001;72:1221–7. doi: 10.1902/jop.2000.72.9.1221. [DOI] [PubMed] [Google Scholar]
- 18.Navarro-Sanchez AB, Faria-Almeida R, Bascones-Martinez A. Effect of nonsurgical periodontal therapy on clinical and immunological response and glycaemic control in type 2 diabetic patients with moderate periodontitis. J Clin Periodontol. 2007;34:835–43. doi: 10.1111/j.1600-051X.2007.01127.x. [DOI] [PubMed] [Google Scholar]
- 19.Correa FO, Goncalves D, Figueredo CM, Gustafsson A, Orrico SR. The short term effectiveness of non-surgical treatment in reducing levels of interleukin-1beta and proteases in gingival crevicular fluid from patients with type 2 diabetes mellitus and chronic periodontitis. J Periodontol. 2008;79:2143–50. doi: 10.1902/jop.2008.080132. [DOI] [PubMed] [Google Scholar]
- 20.Vlachopoulos C, Rokkas K, Ioakeimidis N, Stefanadis C. Inflammation, metabolic syndrome, erectile dysfunction, and coronary artery disease: Common links. Eur Urol. 2007;52:1590–600. doi: 10.1016/j.eururo.2007.08.004. [DOI] [PubMed] [Google Scholar]
- 21.Carneiro FS, Webb RC, Tostes RC. Emerging role for TNF-α in erectile dysfunction. J Sex Med. 2010;7:3823–34. doi: 10.1111/j.1743-6109.2010.01762.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Higashi Y, Sasaki S, Nakagawa K, Matsuura H, Oshima T, Chayama K. Endothelial function and oxidative stress in renovascular hypertension. N Engl J Med. 2002;346:1954–62. doi: 10.1056/NEJMoa013591. [DOI] [PubMed] [Google Scholar]
- 23.Cai H, Harrison DG. Endothelial dysfunction in cardiovascular diseases: The role of oxidant stress. Circ Res. 2000;87:840–4. doi: 10.1161/01.res.87.10.840. [DOI] [PubMed] [Google Scholar]
- 24.Zuo Z, Jiang J, Jiang R, Chen F, Liu J, Yang H, et al. Effect of periodontitis on erectile function and its possible mechanism. J Sex Med. 2011;8:2598–605. doi: 10.1111/j.1743-6109.2011.02361.x. [DOI] [PubMed] [Google Scholar]
- 25.Forner L, Larsen T, Kilian M, Holmstrup P. Incidence of bacteremia after chewing, tooth brushing and scaling in individuals with periodontal inflammation. J Clin Periodontol. 2006;33:401–7. doi: 10.1111/j.1600-051X.2006.00924.x. [DOI] [PubMed] [Google Scholar]
- 26.Zadik Y, Bechor R, Galor S, Justo D, Heruti RJ. Erectile dysfunction might be associated with chronic periodontal disease: Two ends of the cardiovascular spectrum. J Sex Med. 2009;6:1111–6. doi: 10.1111/j.1743-6109.2008.01141.x. [DOI] [PubMed] [Google Scholar]
- 27.Sharma A, Pradeep AR, Raju PA. Association between chronic periodontitis and vasculogenic erectile dysfunction. J Periodontol. 2011;82:1665–9. doi: 10.1902/jop.2011.110049. [DOI] [PubMed] [Google Scholar]
- 28.Oguz F, Eltas A, Beytur A, Akdemir E, Uslu MO, Günes A. Is there a relationship between chronic periodontitis and erectile dysfunction? J Sex Med. 2013;10:838–43. doi: 10.1111/j.1743-6109.2012.02974.x. [DOI] [PubMed] [Google Scholar]
- 29.Matsumoto S, Matsuda M, Takekawa M, Okada M, Hashizume K, Wada N, et al. Association of ED with chronic periodontal disease. Int J Impot Res. 2013;26:13–5. doi: 10.1038/ijir.2013.30. [DOI] [PubMed] [Google Scholar]
- 30.Uppal RS, Bhandari R, Singh K. Association between erectile dysfunction and chronic periodontitis: A clinical study. Indian J Dent Res. 2014;25:430. doi: 10.4103/0970-9290.142516. [DOI] [PubMed] [Google Scholar]
- 31.Keller JJ, Chung SD, Lin HC. A nationwide population-based study on the association between chronic periodontitis and erectile dysfunction. J Clin Periodontol. 2012;39:507–12. doi: 10.1111/j.1600-051X.2012.01879.x. [DOI] [PubMed] [Google Scholar]
- 32.Tsao CW, Liu CY, Cha TL, Wu ST, Chen SC, Hsu CY. Exploration of the association between chronic periodontal disease and erectile dysfunction from a population-based view point. Andrologia. 2014;47:513–8. doi: 10.1111/and.12294. [DOI] [PubMed] [Google Scholar]
- 33.Lee JH, Lee JS, Park JY, Choi JK, Kim DW, Kim YT, et al. Association of lifestyle-related comorbidities with periodontitis: A Nationwide Cohort Study in Korea. Medicine (Baltimore) 2015;94:e1567. doi: 10.1097/MD.0000000000001567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Chou MH, Tsao CW, Cha TL, Wu ST, Liu CY. Chronic periodontitis as risk indicator of erectile dysfunction in young population. Int J Urol. 2016;23(Suppl 1):1–142. [Google Scholar]
- 35.Shariff JA, Ingleshwar A, Lee KC, Zavras AI. Relationship between chronic periodontitis and erectile dysfunction: A narrative review. J Oral Dis 2016. 2016 Article ID 7824321. doi: 10.1155/2016/7824321. [Google Scholar]
- 36.Kellesarian SV, Kellesarian TV, Ros Malignaggi V, Al-Askar M, Ghanem A, Malmstrom H, et al. Association between periodontal disease and erectile dysfunction: A systematic review. Am J Mens Health. 2016 doi: 10.1177/1557988316639050. doi: 10.1177/1557988316639050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Wang Q, Kang J, Cai X, Wu Y, Zhao L. The association between chronic periodontitis and vasculogenic erectile dysfunction: A systematic review and metaanalysis. J Clin Periodontol. 2016;43:206–15. doi: 10.1111/jcpe.12512. [DOI] [PubMed] [Google Scholar]
- 38.Eltas A, Oguz F, Uslu MO, Akdemir E. The effect of periodontal treatment in improving erectile dysfunction: A randomized controlled trial. J Clin Periodontol. 2013;40:148–54. doi: 10.1111/jcpe.12039. [DOI] [PubMed] [Google Scholar]
- 39.Tonetti MS, D’Aiuto F, Nibali L, Donald A, Storry C, Parkar M, et al. Treatment of periodontitis and endothelial function. N Engl J Med. 2007;356:911–20. doi: 10.1056/NEJMoa063186. [DOI] [PubMed] [Google Scholar]
- 40.Li X, Tse HF, Yiu KH, Li LS, Jin L. Effect of periodontal treatment on circulating CD34(+) cells and peripheral vascular endothelial function: A randomized controlled trial. J Clin Periodontol. 2011;38:148–56. doi: 10.1111/j.1600-051X.2010.01651.x. [DOI] [PubMed] [Google Scholar]