

Abstract
Prior evidence shows that positive and negative emotions are associated with better and worse health, respectively. However, the emotion-health relationship may be conflated since this evidence is based nearly exclusively on subjective measures of health. Here, we reviewed more recent evidence focusing on biological health and showed that the emotion-health link is more complex. First, whereas negative emotional states such as negative affect and anger expression are inversely linked to biological health among Americans, this relationship is either not present (negative affect) or even reversed (anger expression) for Japanese. Second, whereas a meaningfulness aspect of happiness (eudaimonia) is linked consistently to better biological health, the relationship between its pleasantness aspect (hedonia) and biological health is uncertain. Moreover, a contextualized sense of meaningfulness in a work setting is strongly associated with better biological health among Japanese. Altogether, the initial evidence reviewed here underscores a need to conceptualize the biological dynamics of health and wellbeing as inherently intertwined with socio-cultural processes.
Is emotion linked to health? The answer to this question would appear straightforward. Whereas positive emotions are good for health, negative emotions are bad for it [1–3]. In their review of relevant empirical evidence, Cohen and Pressman [1] observed that negative emotions including anxiety, depression, and hostility predict increased risk for illness and mortality and further noted that there also likely exists a reliable association between trait positive affect and better health as indexed by lower morbidity and decreased symptoms and pain. Nevertheless, there is an important qualification to this apparently straightforward conclusion. As Cohen and Pressman noted in the same review, the evidence is ‘more complex (page 122)’ when more objective measures of health, most notably mortality, are used. In the current paper, we will go a step further and suggest that when objective indicators of health are utilized, the link between emotion and health could be systematically moderated by certain social contextual factors including global cultural context and more local work context.
Emotion and health: biology matters
It is of great theoretical significance to examine biological indices of health because the relationship between emotion and health can be conflated when health is operationalized by subjective measures such as perceived health, the reported number of chronic health conditions, and self-reported pain. First, emotion and health share a substantial valence component. For example, most emotions are either positive or negative in valence. Similarly, whereas health is positive, ill-health is clearly negative. The resulting semantic overlap alone could yield degrees of linkage between emotion and perceived health [4]. Second, many emotions influence cognitive processes, particularly those involved in biased information search. For example, negative emotions such as worry and anxiety may lend themselves to vigilance to potential threat cues [5]. Conversely, certain positive emotions such as joy and hope may result in optimistic mindsets, which may prime people to positive cues [6]. Thus, a plausible case can be made that emotions may modulate (either augment or reduce) illness perceptions without influencing any underlying biological pathogenesis [7]. These cognitive processes may thus also conflate the emotion-health link when health is assessed subjectively.
Here, we will review recent studies focusing on objective measures of health and point out that when health is operationalized objectively, based on biological responses, a very different picture begins to present itself. The emotion-health link is neither monolithic nor straightforward, consistent with the earlier observation by Cohen and Pressman [1] that the link is quite ‘complex.’ Thus, certain negative emotions may be linked positively to biological health and, conversely, certain positive emotions may be linked negatively to biological health. We argue that to clarify the nature of this complexity, it is crucial to look closely into socio-cultural processes in which emotions are embedded. In what follows, we seek to understand the role of socio-cultural contexts with a focus on three empirical domains — that is, negative affect, anger expression, and happiness.
Three aspects of biological health
Our review focuses on three aspects of biological health: inflammation, cardiovascular malfunction, and anti-viral defense. These three are empirically and theoretically linked. Either alone or in combination, they predict morbidity and mortality. Inflammation originally evolved as a defense against pathogens, most notably bacteria, that could intrude into the bodily system upon injury [8,9•,10,11]. A series of neurochemical reactions in white blood cells are selectively recruited to the injured locations to kill the bacteria. One can argue, however, that this type of defense would be more effective if recruited preemptively in the presence of certain potent cues correlated with physical injury. In fact, whereas inflammation was originally designed to address injury of the physical body, it seems to have been conditioned such that they would be readily activated in response to current sources of ‘stress’ including social exclusion [12,13], prejudice [14], early adversity and abuse [15] and low (vs. high) socio-economic conditions [16,17], among many others. Both metaphorically and literally, inflammation is routinely recruited in response to injury to the symbolic self.
Once inflammatory responses are initiated for certain social reasons, they tend to persist and become chronic. Whereas these responses are initially designed to kill bacteria, they become an important health liability since they begin to cause harm on the cardiovascular system over time. Hence, the degree of inflammation is linked tightly to cardiovascular malfunction [10,18]. In a recent study [19••], we used data from paired surveys conducted in a nationally representative sample of Americans (Midlife in the US, MIDUS) and a representative sample of Japanese in the Tokyo metropolitan area (Midlife in Japan, MIDJA) and assessed two biomarkers of inflammation (interleukin-6 [IL-6] and C-reactive protein [CRP]) and two biomarkers of cardiovascular malfunction (systolic blood pressure [SBP] and total-to-HDL cholesterol ratio [T-to-HDL ratio]) among both Japanese and Americans. As shown in Table 1, the four biomarkers were positively correlated and when a principal component analysis was performed, they cohered together to yield a single factor for both cultural groups. In what follows, this factor score is referred to as the composite index of biological health risk.
Table 1.
Intercorrelations among the four biomarkers constituting biological health risk for Americans (top) and Japanese (bottom)
| Sample and measure | n | Correlations
|
||
|---|---|---|---|---|
| 2 | 3 | 4 | ||
| Americans | ||||
| 1. Log IL-6 | 1044 | .49*** | .13*** | .11*** |
| 2. Log CRP | 1040 | – | .15*** | .19*** |
| 3. Log SBP | 1053 | – | .13*** | |
| 4. Log T-to-HDL ratio | 1043 | – | ||
| Japanese | ||||
| 1. Log IL-6 | 382 | .50*** | .38*** | .25*** |
| 2. Log CRP | 382 | – | .27*** | .28*** |
| 3. Log SBP | 382 | – | .32*** | |
| 4. Log T-to-HDL ratio | 382 | – | ||
Adapted from [19••].
Note: Interleukin-6 (IL-6), C-reactive protein (CRP), systolic blood pressure (SBP), and total cholesterol scores were winsorized to 3 standard deviations from the mean to adjust for extreme values (calculated separately for each culture), and all biomarkers were log-transformed to reduce skewness.
p < .001.
Another important aspect of biological health that is associated with inflammation is a series of neurobiological and molecular reactions designed to defend against viruses. Unlike bacteria, viruses are mere combinations of DNAs. They infect the body, intrude into the nucleus of each cell, and cause a series of pathogenic reactions at the molecular level. One important methodological advancement involves a measurement of the molecular responses by examining transcriptional responses of genes involved in anti-viral defense [9•,15,17]. One can observe that under a variety of conditions of ‘stress’ including loneliness, social exclusion, and poverty, transcriptional responses of 30 or so genes linked to anti-viral defense are typically down-regulated whereas the transcriptional responses of an approximately equal number of genes linked to inflammation are up-regulated. In combination, these responses have been called the conserved transcriptional responses to adversity (CTRA). It is not understood why the activation of inflammation and the de-activation of anti-viral defense occur in combination in response to stress. One possibility is that the conditions that evolutionarily required inflammatory responses such as social isolation and low population density are precisely the ones that reduce the risk of viral infection [9•,20].
There is good reason to expect that CTRA would be linked to physical health outcomes. As noted by Finch in his major review on the topic [11], ‘later life dysfunctions of the vasculature, brain, and cell growth may be traced to prodromal (subclinical) inflammatory changes from early in life (page 6).’ Recent work has also provided direct empirical support for the link between CTRA and health outcomes [21•,22].
Negative affect
There is considerable evidence that negative affect is strongly correlated with poor health when subjective measures of health are tested. However, is this also the case when health is operationalized by some objective, biological indices? Miyamoto and colleagues [23] addressed this question by examining the link between negative affect and IL-6 (a potent marker of inflammation) using the MIDUS/MIDJA dataset. The average extent of experiencing six negative emotions (e.g., nervous, hopeless, worthless) ‘over the past 30 days’ was used to measure negative affect. After controlling for factors known to be associated with the level of inflammation, including age, gender, educational attainment, adiposity (measured by body-mass-index, BMI), and the reported number of health symptoms, the researchers found that negative affect is positively associated with IL-6 among Americans (Figure 1). Importantly, however, they also observed that the relationship vanished completely among Japanese.
Figure 1.
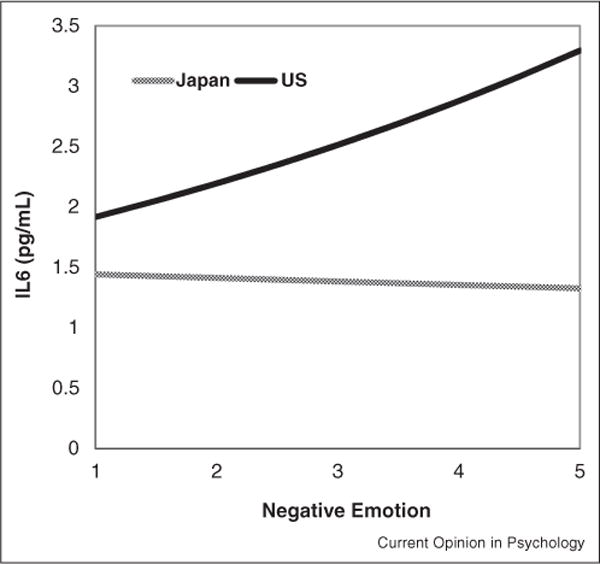
Cultural moderation of the association between negative emotions and IL-6.
Adapted from [23].
Miyamoto and colleagues argued that this cross-cultural pattern might reflect cross-culturally divergent folk theories of emotion. Previous evidence suggests that whereas Westerners have a linear theory of emotion, assuming that the valence of emotion tends to remain the same over time, Asians have a more dialectical theory and believe that emotions can change in valence over time [24,25]. Building on this evidence, Miyamoto et al. hypothesized that negative affect could be a cue for further negative emotions (and thus potentially threatening) for Westerners, and therefore, negative affect is linked to compromised health for these individuals. By contrast, for Asians negative affect could signal potential positive events in the future, reflecting their dialectical view of emotions. Thus, negative affect could be less threatening, and therefore, there is no health-compromising effect of negative affect for Asians.
Anger expression
Expression of anger is typically seen as unhealthy in common Western discourse. However, is this contingency always the case? While anger and anger expression are linked to increased mortality [26], this evidence is based nearly exclusively on Western samples. Kitayama, Park and colleagues [19••,27] have argued that the exclusive focus on Western samples may be especially problematic in the case of anger because anger has two primary components — frustration and dominance — that may entail different health consequences depending on which of the two is made salient in a given cultural context. Of course, these two aspects are functionally related. For example, when frustrated, people may experience lowering of self-esteem and self-respect. Under such conditions, they may show dominance display so as to compensate for the impaired sense of self-esteem or status [28]. Nevertheless, the two aspects may also vary in salience, resulting in culturally divergent meanings and functions of anger and anger expression.
In Western societies, the self is typically believed to be independent from others and relatively autonomous and free of social influences [29]. As a consequence, personal goals are highly salient [30]. Because of the cultural emphasis on personal goals, when individuals are prevented from pursuing their personal goals, they will be frustrated, which may serve as a major instigator of anger. Anger therefore is likely to be a potent index of the degree of exposure to socio-economic conditions that induce feelings of frustration. Supporting this view, in the MIDUS (American) sample, the extent of anger expression was substantially higher among people who were lower in subjective social status than their higher status counterparts as lower status Americans are likely to experience more frustrations in life [31]. Moreover, as may be expected from this finding, our recent work [19••] showed that among Americans, anger expression significantly predicted increases in biological health risk (assessed by the four markers noted above), presumably because the frequency of anger expression serves as a reliable index of frustration-inducing life difficulties surrounding these individuals (Figure 2).
Figure 2.
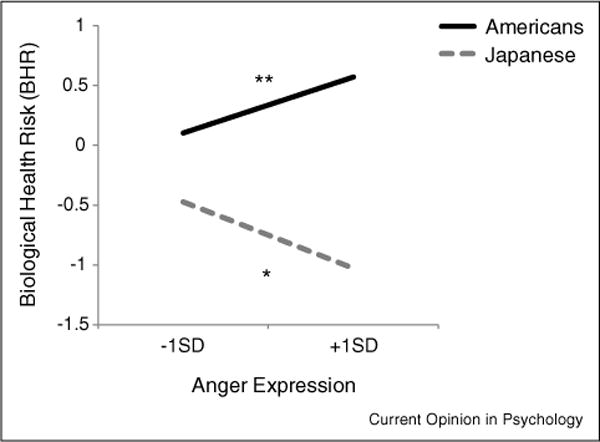
The relationships between anger expression and biological health risk for Americans (solid line) and Japanese (dotted line). *p < .05, **p < .01.
Adapted from [19••].
By contrast, in Eastern societies, the self is typically believed to be interdependent with others and embedded in social relations [29]. As a result, social roles and obligations, especially those linked to social status tend to be highly salient. Because of the cultural emphasis on social status, it is likely that anger may be more typically utilized as an expression of dominance and power. In fact, unlike in the U.S., in Japan it is people with higher objective social status who reportedly expressed more anger as these individuals are more at liberty to express anger as a display of dominance [31]. Moreover, as may also be anticipated from this analysis, among Japanese, anger expression significantly predicted decreases in biological health risk, presumably because anger in this culture is likely to index the degree to which people are empowered and entitled [19••] (Figure 2).
Happiness
If negative emotions are sometimes linked to better biological health, certain positive emotions may well be sometimes linked to poor biological health. An inquiry along this line has just begun [32,33••,34•]. This line of work draws on a distinction between two types of well-being or happiness, called eudaimonia and hedonia. Eudaimonia refers to the meaningfulness or fullness of life, realized through the identification of the self in certain moral dimensions such as purpose, improvement, generativity, and community engagement, whereas hedonia refers to the total amount of pleasure as indicated by overall positive (vs. negative) affect and life satisfaction. When self-report instruments are used to assess these two aspects of happiness, they are correlated, sometimes highly, but they are still distinct, loading on two separable factors [35].
So far, the health effects of the two types of happiness have been tested in separate studies of Americans [32,34•] and Japanese [33••]. Fredrickson, Cole, and colleagues have tested American samples and found that eudaimonia is consistently linked to reduced levels of CTRA [32,34•]. Interestingly, the association between hedonia and CTRA is never in the same direction. In fact, the effect sometimes appears to come out in the opposite direction, implying that increased levels of hedonia can be linked to increases in CTRA. These findings suggest that although pleasure is by definition good at subjective levels, it may not necessarily be good for biological health. At present, it is not clear why there is an inverse association between hedonia and biological health. The finding requires careful interpretation since the two aspects of wellbeing are highly correlated, which makes it difficult to understand the independent effect of each. Nevertheless, one might speculate that hedonic pursuit of pleasure could sometimes compromise health. For example, certain behaviors (e.g., drug use) enhance hedonic pleasure while compromising biological health. Clearly, more work is needed.
In a recent study, Kitayama and colleagues replicated and extended the analysis by Fredrickson et al. [32,34•] by testing 107 Japanese male employees at a Japanese IT firm. They similarly found that eudaimonia is linked to reduced levels of CTRA. Again, however, hedonia was linked to increased levels of CTRA [33••]. Importantly, the researchers also tested several additional factors linked to a contextualized sense of identity including perceived interdependence or independence of the self at work. These more context-specific factors, which can foster the meaningfulness in life and thus eudaimonic happiness in work settings, were significantly linked to reduced CTRA. In fact, the contextualized sense of meaningfulness was an even stronger predictor of reduced CTRA than the general eudaimonia (see Figure 3). Although there is no cross-cultural investigation focusing on CTRA, specific determinants of meaningfulness may be cross-culturally variable. For example, in the Japanese sample here, the self’s interdependence at work had a strongly salubrious effect on CTRA. Relatively speaking, the effect of the self’s independence at work had a relatively small, albeit still significant effect. Future work should test these effects in Western societies where independence is likely more strongly sanctioned than interdependence.
Figure 3.
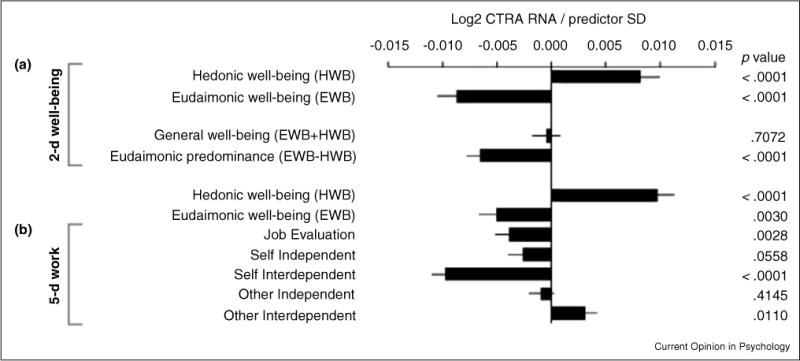
Relationships of CTRA gene expression to dimensions of generalized well-being and work-specific meaning. Each bar indicates the relative increase (positive values) or decrease (negative values) of CTRA contrasting 1.5 standard deviation (SD) higher or lower than the mean in each of the predictor variables. The statistical significance levels are indicated by the p values.
Adapted from [33••].
Conclusions
Although the cross-cultural research on emotion and biological health is in its infancy and much more must be done, two tentative conclusions seem warranted. First, biological health is related to, but somewhat distinct from its subjective counterparts. For example, certain biological conditions (e.g., early stage cancer) may have no consequences on subjective health and, conversely, certain aspects of subjective experience (e.g., placebo effects) may not necessarily have much influence on underlying biological health correlates. Accordingly, as we have shown, correlates of biological versus subjective health could be quite distinct. Second, previous work shows certain important socio-cultural moderations in predicting subjective health [36–38], but the initial evidence reviewed here suggests that similar moderations might be more dramatic in the case of biological health. We suspect that this might be the case in part because the relationship between emotion and biological health is unlikely to be conflated for semantic reasons (see [39,40] for a related debate on the use of self-report measures).
One important shortcoming of the work on emotion and biological health is the paucity of systematic empirical inquiry across cultures. In fact, the evidence reviewed here is confined to the comparisons between the U.S. and Japan. Much more empirical investigation in multiple countries is warranted in view of the initial evidence reviewed here. It remains to be seen exactly what overarching theoretical framework would emerge as a way to integrate various patterns of socio-cultural moderation. The cultural views of the self as independent or interdependent are likely to continue to be important in this domain [29,41]. Other important considerations include tightness vs. looseness of norm enforcement [42], religion [43], and migration [44•,45]. Further, numerous ecological factors including historical mode of subsistence [46,47], residential mobility [48], and pathogen threat [49] must be systematically explored [41,50]. Further, future work should also take into account genetic variability across ethnic groups. Finally, the human biological health is very complex and involves many processes and mechanisms that have so far been unexplored. Researchers in this area must be mindful of this complexity and must continue to extend the range of coverage by focusing on new bio-chemical and molecular mechanisms as well as empirical markers of these mechanisms.
Footnotes
Writing of this paper was supported by National Science Foundation grant, SES 1325881, and National Institute on Aging grant, 5R37AG027343.
Conflict of interest statement
Nothing declared.
References and recommended reading
Papers of particular interest, published within the period of review, have been highlighted as:
• of special interest
•• of outstanding interest
- 1.Cohen S, Pressman SD. Positive affect and health. Curr Dir Psychol Sci. 2006;15:122–125. [Google Scholar]
- 2.Pressman SD, Cohen S. Does positive affect influence health? Psychol Bull. 2005;131:925–971. doi: 10.1037/0033-2909.131.6.925. http://dx.doi.org/10.1037/0033-2909.131.6.925. [DOI] [PubMed] [Google Scholar]
- 3.Fredrickson BL. Positive Emotions Broaden and Build. (1st) 2013 Copyright © 2013 Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/B978-0-12-407236-7.00001-2.
- 4.Pennebaker JW, Kiecolt-Glaser JK, Glaser R. Disclosure of traumas and immune function: health implications for psychotherapy. J Consult Clin Psychol. 1988;56:239–245. doi: 10.1037//0022-006x.56.2.239. http://dx.doi.org/10.1037/0022-006X.56.2.239. [DOI] [PubMed] [Google Scholar]
- 5.Derryberry D, Reed MA. Temperament and attention: orienting toward and away from positive and negative signals. J Personal Soc Psychol. 1994;66:1128–1139. doi: 10.1037//0022-3514.66.6.1128. http://dx.doi.org/10.1037/0022-3514.66.6.1128. [DOI] [PubMed] [Google Scholar]
- 6.Fredrickson BL, Losada MF. Positive affect and the complex dynamics of human flourishing. Am Psychol. 2005;60:678–686. doi: 10.1037/0003-066X.60.7.678. http://dx.doi.org/10.1037/0003-066X.60.7.678. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Cohen S, Doyle WJ, Turner RB, Alper CM, Skoner DP. Emotional style and susceptibility to the common cold. Psychosom Med. 2003;65:652–657. doi: 10.1097/01.psy.0000077508.57784.da. http://dx.doi.org/10.1097/01.PSY.0000077508.57784.DA. [DOI] [PubMed] [Google Scholar]
- 8.Mogensen TH. Pathogen recognition and inflammatory signaling in innate immune defenses. Clin Microbiol Rev. 2009;22:240–273. doi: 10.1128/CMR.00046-08. http://dx.doi.org/10.1128/CMR.00046-08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9•.Cole SW. Human social genomics. PLoS Genet. 2015;10:e1004601. doi: 10.1371/journal.pgen.1004601. The paper provides a theoretical overview of an emerging field of social genomics, with a focus on social signal pathways that induce a conserved transcriptional response to adversity — the response composed of up-regulation of genes involved in inflammation and down-regulation of those involved in anti-viral defense. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Medzhitov R. Origin and physiological roles of inflammation. Nature. 2008;454:428–435. doi: 10.1038/nature07201. http://dx.doi.org/10.1038/nature07201. [DOI] [PubMed] [Google Scholar]
- 11.Finch CE. The Biology of Human Longevity. Academic Press; 2010. [Google Scholar]
- 12.Cole SW, Hawkley LC, Arevalo J, Cacioppo JT. Transcript origin analysis identifies antigen-presenting cells as primary targets of socially regulated gene expression in leukocytes. Proc Natl Acad Sci. 2011:3080–3085. doi: 10.1073/pnas.1014218108. http://dx.doi.org/10.1073/pnas.1014218108/-/DCSupplemental. [DOI] [PMC free article] [PubMed]
- 13.Cacioppo JT, Cacioppo S, Boomsma DI. Evolutionary mechanisms for loneliness. Cognit Emot. 2013;28:3–21. doi: 10.1080/02699931.2013.837379. http://dx.doi.org/10.1080/02699931.2013.837379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Wallace R, Wallace D, Wallace RG. Coronary heart disease, chronic inflammation, and pathogenic social hierarchy: a biological limit to possible reductions in morbidity and mortality. J Natl Med Assoc. 2004;96:609. [PMC free article] [PubMed] [Google Scholar]
- 15.Kohrt BA, Worthman CM, Adhikari RP, Luitel NP, Arevalo JMG, Ma J, et al. Psychological resilience and the gene regulatory impact of posttraumatic stress in Nepali child soldiers. Proc Natl Acad Sci. 2016;113:8156–8161. doi: 10.1073/pnas.1601301113. http://dx.doi.org/10.1073/pnas.1601301113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Sapolsky RM. Social status and health in humans and other animals. Annu Rev Anthropol. 2004;33:393–418. http://dx.doi.org/10.1146/annurev.anthro.33.070203.144000. [Google Scholar]
- 17.Chen E, Miller GE, Kobor MS, Cole SW. Maternal warmth buffers the effects of low early-life socioeconomic status on pro-inflammatory signaling in adulthood. Mol Psychiatry. 2011;16:729–737. doi: 10.1038/mp.2010.53. http://dx.doi.org/10.1038/mp.2010.53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Everson-Rose SA, Lewis TT. Psychological factors and cardiovascular diseases. Annu Rev Public Health. 2005;26:469–500. doi: 10.1146/annurev.publhealth.26.021304.144542. http://dx.doi.org/10.1146/annurev.publhealth.26.021304.144542. [DOI] [PubMed] [Google Scholar]
- 19••.Kitayama S, Park J, Boylan JM, Miyamoto Y, Levine CS, Markus HR, et al. Expression of anger and ill health in two cultures: an examination of inflammation and cardiovascular risk. Psychol Sci. 2015;26:211–220. doi: 10.1177/0956797614561268. http://dx.doi.org/10.1177/0956797614561268. Anger expression is believed to be unhealthy. However, little evidence exists if this belief is valid cross-culturally. Using a large-scale survey-based dataset, this study shows that anger expression is indeed associated with increased biological health risk among Americans. Importantly, however, the association was significantly reversed among Japanese. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Irwin MR, Cole SW. Reciprocal regulation of the neural and innate immune systems. Nat Rev Immunol. 2011;11:625–632. doi: 10.1038/nri3042. http://dx.doi.org/10.1038/nri3042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21•.Antoni MH, Bouchard LC, Jacobs JM, Lechner SC, Jutagir DR, Gudenkauf LM, et al. Stress management, leukocyte transcriptional changes and breast cancer recurrence in a randomized trial: an exploratory analysis. Psychoneuroendocrinology. 2016;74:269–277. doi: 10.1016/j.psyneuen.2016.09.012. http://dx.doi.org/10.1016/j.psyneuen.2016.09.012) An empirically-validated group-based psychosocial intervention, performed on breast cancer patients, shows a significant reduction of CTRA (transcriptional responses linked to both increased inflammation and reduced antiviral defense) post-surgery. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Knight JM, Rizzo JD, Logan BR, Wang T, Arevalo JMG, Ma J, et al. Low socioeconomic status, adverse gene expression profiles, and clinical outcomes in hematopoietic stem cell transplant recipients. Clin Cancer Res. 2016;22:69–78. doi: 10.1158/1078-0432.CCR-15-1344. http://dx.doi.org/10.1158/1078-0432.CCR-15-1344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Miyamoto Y, Boylan JM, Coe CL, Curhan KB, Levine CS, Markus HR, et al. Negative emotions predict elevated interleukin-6 in the United States but not in Japan. Brain Behavior and Immunity. 2013;34:79–85. doi: 10.1016/j.bbi.2013.07.173. http://dx.doi.org/10.1016/j.bbi.2013.07.173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Miyamoto Y, Ryff CD. Cultural differences in the dialectical and non-dialectical emotional styles and their implications for health. Cognit Emot. 2011;25:22–39. doi: 10.1080/02699931003612114. http://dx.doi.org/10.1080/02699931003612114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Uchida Y, Kitayama S. Happiness and unhappiness in east and west: themes and variations. Emotion. 2009;9:441–456. doi: 10.1037/a0015634. http://dx.doi.org/10.1037/a0015634. [DOI] [PubMed] [Google Scholar]
- 26.Chida Y, Steptoe A. The association of anger and hostility with future coronary heart disease. J Am Coll Cardiol. 2009;53:936–946. doi: 10.1016/j.jacc.2008.11.044. http://dx.doi.org/10.1016/j.jacc.2008.11.044. [DOI] [PubMed] [Google Scholar]
- 27.Park J, Kitayama S. Anger expressionandhealth:thecultural moderation hypothesis. In: Carol P, Ryff D, Krueger RF, editors. Oxford HandbookofIntegrated Health Science. Oxford University Press; in press. [Google Scholar]
- 28.Henry PJ. Low-status compensation: a theory for understanding the role of status in cultures of honor. J Personal Soc Psychol. 2009;97:451–466. doi: 10.1037/a0015476. http://dx.doi.org/10.1037/a0015476. [DOI] [PubMed] [Google Scholar]
- 29.Markus HR, Kitayama S. Culture and the self: implications for cognition, emotion, and motivation. Psychol Rev. 1991;98:224–253. [Google Scholar]
- 30.Oishi S, Diener E. Goals, culture, and subjective well-being. Personal Soc Psychol Bull. 2001;27:1674–1682. http://dx.doi.org/10.1177/01461672012712010. [Google Scholar]
- 31.Park J, Kitayama S, Markus HR, Coe CL, Miyamoto Y, Karasawa M, et al. Social status and anger expression: the cultural moderation hypothesis. Emotion. 2013;13:1122–1131. doi: 10.1037/a0034273. http://dx.doi.org/10.1037/a0034273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Fredrickson BL, Grewen KM, Coffey KA, Algoe SB, Firestine AM, Arevalo JMG, et al. A functional genomic perspective on human well-being. Proc Natl Acad Sci. 2013;110:13684–13689. doi: 10.1073/pnas.1305419110. http://dx.doi.org/10.1073/pnas.1305419110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33••.Kitayama S, Akutsu S, Uchida Y, Cole SW. Work, meaning, and gene regulation: findings from a Japanese information technology firm. Psychoneuroendocrinology. 2016;72:175–181. doi: 10.1016/j.psyneuen.2016.07.004. http://dx.doi.org/10.1016/j.psyneuen.2016.07.004. Based on prior work showing that CTRA (transcriptional responses linked to increased inflammation and decreased antiviral defense) is associated with eudaimonic wellbeing, this study finds that an analogous association is observed with meaningfulness at workplace among male Japanese workers. [DOI] [PubMed] [Google Scholar]
- 34•.Fredrickson BL, Grewen KM, Algoe SB, Firestine AM, Arevalo JMG, Ma J, et al. Psychological well-being and the human conserved transcriptional response to adversity. PLOS ONE. 2015;10:e0121839. doi: 10.1371/journal.pone.0121839. http://dx.doi.org/10.1371/journal.pone.0121839.s008. This study provides a comprehensive replication of a prior finding that CTRA (transcriptional responses linked to increased inflammation and decreased antiviral defense) is linked inversely to eudaimonic wellbeing. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Keyes CLM, Shmotkin D, Ryff CD. Optimizing well-being: the empirical encounter of two traditions. J Personal Soc Psychol. 2002;82:1007–1022. http://dx.doi.org/10.1037//0022-3514.82.6.1007. [PubMed] [Google Scholar]
- 36.Park J, Kitayama S, Karasawa M, Curhan K, Markus HR, Kawakami N, et al. Clarifying the links between social support and health: culture, stress, and neuroticism matter. J Health Psychol. 2013;18:226–235. doi: 10.1177/1359105312439731. http://dx.doi.org/10.1177/1359105312439731. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Curhan KB, Sims T, Markus HR, Kitayama S, Karasawa M, Kawakami N, et al. Just how bad negative affect is for your health depends on culture. Psychol Sci. 2014;25:2277–2280. doi: 10.1177/0956797614543802. http://dx.doi.org/10.1177/0956797614543802. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Curhan KB, Levine CS, Markus HR, Kitayama S, Park J, Karasawa M, et al. Subjective and objective hierarchies and their relations to psychological well-being: a U.S./Japan comparison. Soc Psychol Personal Sci. 2014;5:855–864. doi: 10.1177/1948550614538461. http://dx.doi.org/10.1177/1948550614538461. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Oishi S, Roth DP. J Res Personal. 2009;43:107–109. http://dx.doi.org/10.1016/j.jrp.2008.11.002. [Google Scholar]
- 40.Heine SJ, Lehman DR, Peng K, Greenholtz J. What’s wrong with cross-cultural comparisons of subjective Likert scales?: the reference-group effect. J Personal Soc Psychol. 2002;82:903–918. http://dx.doi.org/10.1037/0022-3514.82.6.903. [PubMed] [Google Scholar]
- 41.Kitayama S, Uskul AK. Culture, mind, and the brain: current evidence and future directions. Annu Rev Psychol. 2011;62:419–449. doi: 10.1146/annurev-psych-120709-145357. http://dx.doi.org/10.1146/annurev-psych-120709-145357. [DOI] [PubMed] [Google Scholar]
- 42.Gelfand MJ, Raver JL, Nishii L, Leslie LM, Lun J, Lim BC, et al. Differences between tight and loose cultures: a 33-nation study. Science. 2011;332:1100–1104. doi: 10.1126/science.1197754. http://dx.doi.org/10.1126/science.1197754. [DOI] [PubMed] [Google Scholar]
- 43.Norenzayan A, Shariff AF. The origin and evolution of religious prosociality. Science. 2008;322:58–62. doi: 10.1126/science.1158757. http://dx.doi.org/10.1126/science.1158757. [DOI] [PubMed] [Google Scholar]
- 44•.Rychlowska M, Miyamoto Y, Matsumoto D, Hess U, Gilboa-Schechtman E, Kamble S, et al. Heterogeneity of long-history migration explains cultural differences in reports of emotional expressivity and the functions of smiles. Proc Natl Acad Sci. 2015;112:E2429–E2436. doi: 10.1073/pnas.1413661112. http://dx.doi.org/10.1073/pnas.1413661112. Using a comprehensive cross-cultural database, this study shows that the expressivity of ‘smile’ is strongly linked to the historical heterogeneity of countries or regions of origin for people who settled in various contemporary cultures. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Kitayama S, Ishii K, Imada T, Takemura K, Ramaswamy J. Voluntary settlement and the spirit of independence: evidence from Japan’s ‘northern frontier’. J Personal Soc Psychol. 2006;91:369–384. doi: 10.1037/0022-3514.91.3.369. http://dx.doi.org/10.1037/0022-3514.91.3.369. [DOI] [PubMed] [Google Scholar]
- 46.Uskul AK, Kitayama S, Nisbett RE. Ecocultural basis of cognition: farmers and fishermen are more holistic than herders. Proc Natl Acad Sci. 2008;105:8552–8556. doi: 10.1073/pnas.0803874105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Talhelm T, Zhang X, Oishi S, Shimin C, Duan D, Lan X, et al. Large-scale psychological differences within China explained by rice versus wheat agriculture. Science. 2014;344:603–608. doi: 10.1126/science.1246850. http://dx.doi.org/10.1126/science.1246850. [DOI] [PubMed] [Google Scholar]
- 48.Oishi S, Schimmack U. Residential mobility, well-being, and mortality. J Personal Soc Psychol. 2010;98:980–994. doi: 10.1037/a0019389. http://dx.doi.org/10.1037/a0019389. [DOI] [PubMed] [Google Scholar]
- 49.Fincher CL, Thornhill R, Murray DR, Schaller M. Pathogen prevalence predicts human cross-cultural variability in individualism/collectivism. Proc R Soc Lond B Biol Sci. 2008;275:1279–1285. doi: 10.1098/rspb.2008.0094. http://dx.doi.org/10.1098/rspb.2008.0094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Oishi S. Socioecological psychology. Annu Rev Psychol. 2014;65:581–609. doi: 10.1146/annurev-psych-030413-152156. http://dx.doi.org/10.1146/annurev-psych-030413-152156. [DOI] [PubMed] [Google Scholar]