

Abstract
Excessive fat accumulation in the body may impair health leading to a significant long-term health consequences including the development of diabetes, coronary heart disease, and osteoarthritis as well as increasing the risk of developing certain cancers and influencing their outcomes. England has some of the worst figures and trends in obesity compared with the rest of the Europe. In the majority of European countries the trend has increased from 10% to 40% in the last 10 years, whereas in England prevalence has more than doubled. This article outlines the public health impact of rising obesity levels.
Keywords: Obesity, Overweight, Public health
Introduction
Obesity is an abnormal accumulation of body fat (usually 20% above the normal ideal body weight) to the extent that it may have an adverse effect on health1. It is a chronic disorder, officially classified as a disease (ICD-10 E66.0) in 1990 and defined as a body mass index (BMI) of 30 kg/m2 or more (Fig. 1)2,3. Obesity is a rapidly growing public health problem affecting an increasing number of countries worldwide because of its prevalence, costs, and health effects4.
Figure 1.
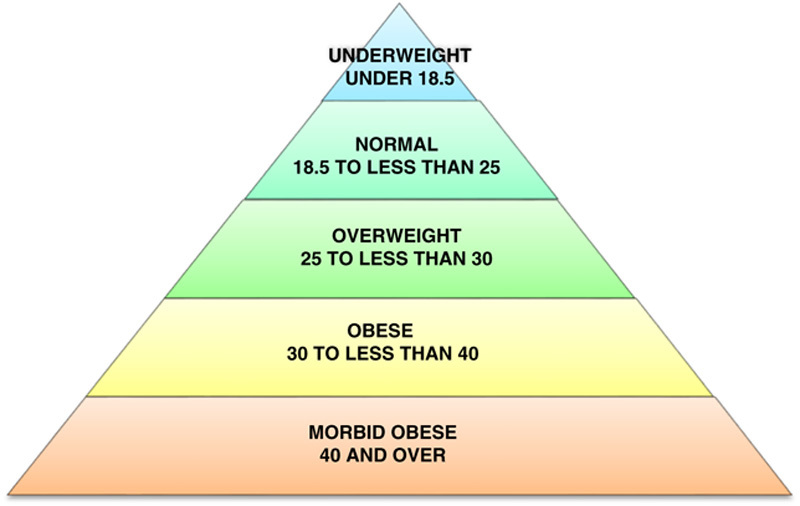
Body mass index definitions (kg/m2). Source: Centres for Disease Control and Prevention, 2011.
Compared with the medical definition of obesity5, the public health explanation places emphasis on the preventive and causative factors. Effective treatment requires identification and modification of these etiological vectors6. However, the causes are often complex or not well understood. In addition, every discipline has dimensionalized the problem along different lines (Fig. 2)7.
Figure 2.
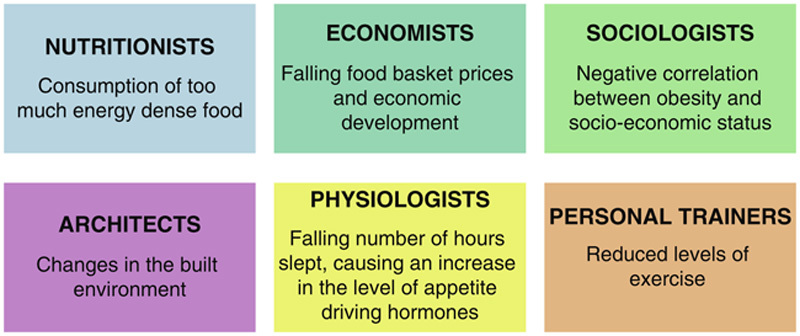
Causes of obesity.
Obesity a growing public health problem
In 1995, there were an estimated 200 million obese adults worldwide. However, by the year 2000 the number had grown to 300 million and has continued to increase since then8.
The trends for increasing obesity are broadly repeated throughout Western Europe and a similar rise has been observed in the United States. In 1986, 1 in 200 adults in America were morbidly obese; by 2004, the figure was 1 in 50. Currently, 1 in 5 adults are morbidly obese in America9.
The rates of obesity have similarly increased in the United Kingdom since the 1980s, this rise is projected to continue. The 2008 Health Survey for England report indicated that 1 in 4 adults were obese10.
Since 1991 the prevalence of obesity has increased by 65% in men, and 25% in women. It was estimated that in 2010, England contained 6.6 million obese men (33% of the population) and 5.9 million obese women (28% of the population)11. The proportion of men predicted to be obese was greater than the proportion of women12. It has been estimated that on current trends, by 2050, 60% of males and 50% of females will be obese13.
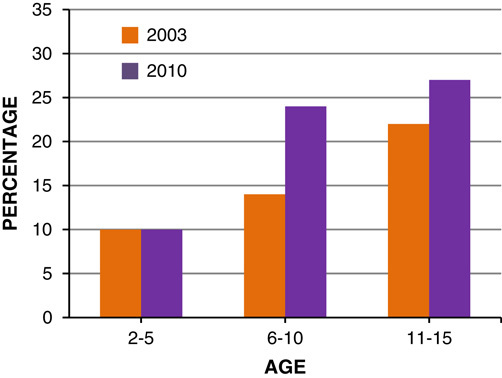
The current trend shows that around 8% of 1–2-year-old obese children will become obese adults, and 80% of 10–14-year olds will become obese adults14. In 2003, approximately 750,000 boys and 676,000 girls were obese in England. If the same trend is applied to mid-2010 population, it is estimated that 792,321 (19% of population) boys and 910,630 (22% of population) girls were obese in 2010 (Figs. 3, 4)8.
Figure 3.

Prevalence of boys overweight and obese in 2003 and 2010, by age.
Figure 4.
Prevalence of girls overweight and obese in 2003 and 2010, by age.
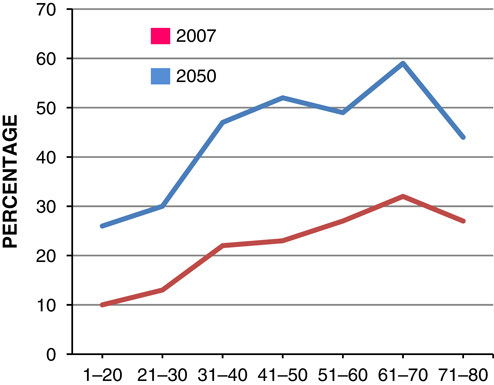
Evidence suggests that by 2050, among children aged 6–10 years, the number of obesity among boys will be greater than girls with an estimate of 50% of boys being obese by 2050 (Figs. 5, 6)10.
Figure 5.
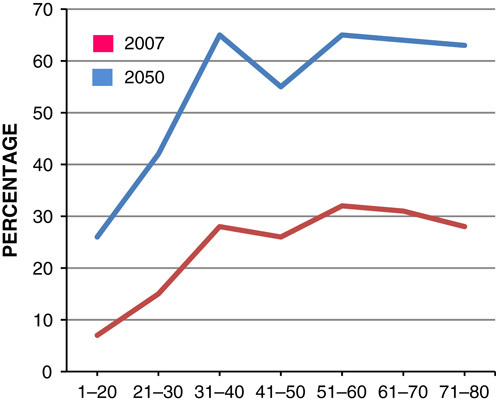
Estimated percentage of male obese at 2007 and 2050.
Figure 6.
Estimated percentage of female obese at 2007 and 2050.
Adults working in unskilled manual profession are over 4 times more likely to be classified as morbidly obese compared with those in professional employments, with women showing a larger difference than men (Figs. 7, 8)15. It is estimated that by 2050, 15% of females belonging to social class I and 62% for the females belonging to social class V will be obese. However, the predicted difference is lower for male adults, 52% of males belonging to social class I will be obese compared with 60% of social class V males15.
Figure 7.
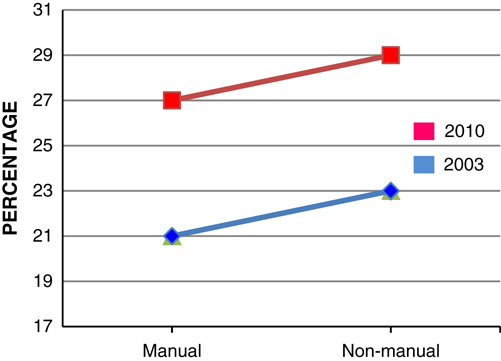
Prevalence of men obese in England in 2003 and 2010 by social class.
Figure 8.
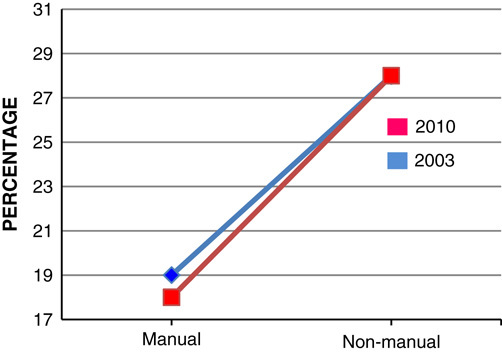
Prevalence of females obese in England in 2003 and 2010 by social class.
The prevalence of obesity is higher in children who live in households where both the parents are overweight or obese. In 2010, around 415,844 boys and 320,727 girls were estimated to be obese by their parental obesity status11. Therefore, boys may be more affected by their parental weight than girls (Figs. 9, 10). If 1 parent is obese the odds ratio of a 1–2-year old being an obese adult is 30% more than nonobese and it increases by 17-fold for a 15–17-year old. The increased prevalence of obesity in childhood is likely to continue to adult life making them more susceptible to illness11.
Figure 9.
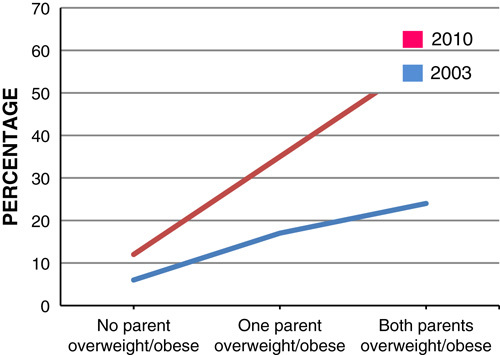
Prevalence of boys overweight and obese in 2003 and 2010, by parental body mass index status.
Figure 10.
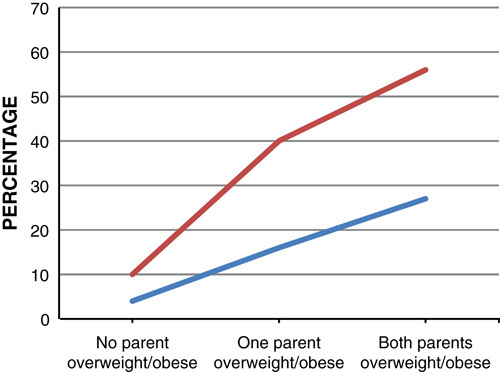
Prevalence of girls overweight and obese in 2003 and 2010, by parental body mass index status.
Ethnicity is one of the major determinants in obesity trends. It is estimated that by 2050, people belonging to Black Caribbean and Chinese ethnic backgrounds will be less obese than the current value. Asian children are also 4 times more likely to be obese than white children (Figs. 11, 12)16.
Figure 11.
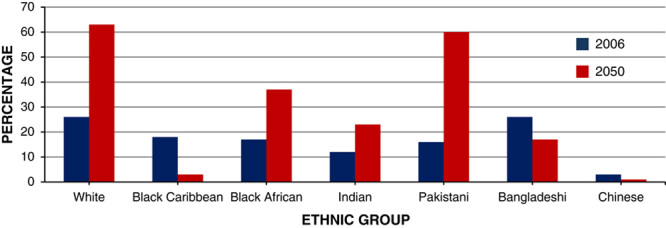
Predicted percentage of male population obese at 2006 and 2050, by ethnic group.
Figure 12.
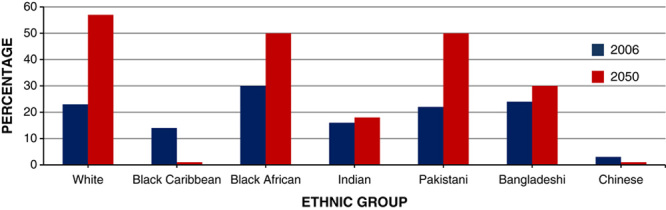
Predicted percentage of female population obese at 2006 and 2050, by ethnic group.
Evidence suggests that a significant difference exists between regions in England. By 2050, estimates suggest that 70% of women in Yorkshire and Humberside will be obese, whereas in other regions such as the south-west of England it will be 7% (Fig. 13).
Figure 13.
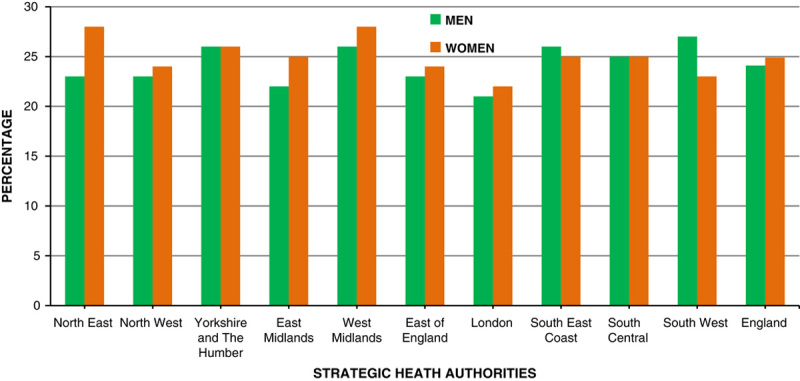
Obesity prevalence rate 2008/2009.
The impact of increased prevalence of obesity on public health
Life expectancy
Overall life expectancy is expected to rise 8 years for males and 7 years for females by the mid-21st century17. However, the increased prevalence of obesity may have long-term ramifications for this trend among young adults and children. If the prevalence of obesity increases as predicted, females will lose around a fifth of a year and males around a third by the middle of the 21st century18. Therefore, the rising trend for obesity will significantly affect the health of the population as well their contribution to the economy and society4. Concomitantly, health care costs and the rates of diseases/conditions caused and influenced by obesity will increase. These are further downward drivers life expectancy19.
Employment
Obesity has become stigmatized, and discrimination presents significant challenges in education, health care, and employment. There is weak evidence that the IQ of overweight children is lower than those of normal weight20–22. This results in stress, psychological distress, depression, social isolation, low self-esteem, and poor body image. Therefore, due to the increased prevalence of obesity, unemployment may increase and appropriately qualified obese individuals may stay unemployed due to discrimination or fear of it in the workplace23.
Quality of life
Evidence suggests that obesity is associated with shortness of breath, back pain, reduced mobility, poor quality of life, and increased psychological and social burden24.
In the older population, obesity causes cartilage degradation and increases the risk of physical and cognitive disability25,26. These are major risk factors associated with institutionalization, greater health care costs, dependency, utilization of health care services, poor health outcomes, reduced exercise capacity, and mortality27.
Sarcopenia is a condition of age-related loss of muscle mass and strength and is a common problem in old age. Evidence suggests that older people with sarcopenia and obesity have worse physical function than those with sarcopenia alone. Such effects on disability and quality of life may not just be additive but synergistic28–30.
Obesity-associated diseases
In the United Kingdom, it is estimated that each year 9000 premature deaths are due to obesity, accounting for 8.7% of all deaths31. It is highly associated with other health problems and diseases leading to disability and in many cases death (Fig. 14)32. Because obesity rates vary among different ethnicities, the diseases associated with it may result in health inequalities (Figs. 13, 14)33. Among adults the most common chronic conditions associated with obesity include: arthritis, hypertension, heart disease, stroke, cancer, and diabetes34. We have talked about the impact on preconceptual and pregnant women elsewhere35.
Figure 14.
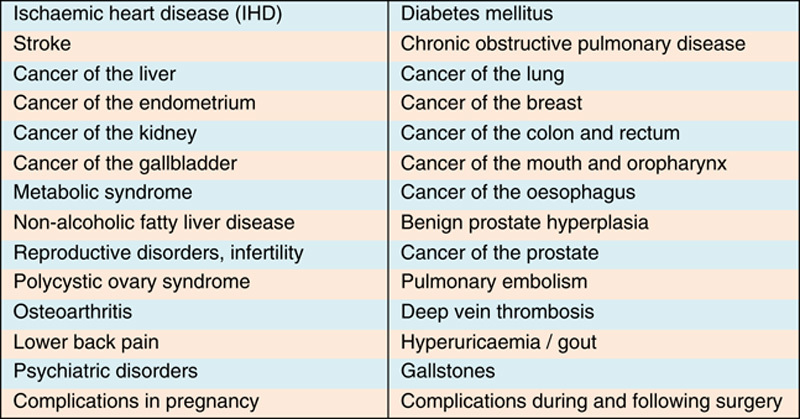
Diseases associate with obesity.
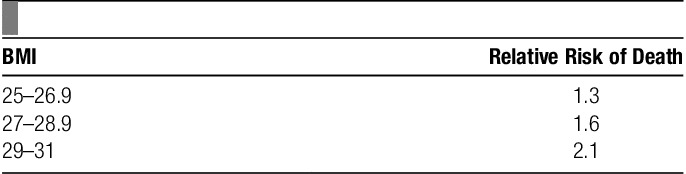
The result of these associations is that the relative risk of death increases with BMI in a nonlinear manner (Table 1)36.
Table 1.
Classification of body mass index (BMI) and relative risk of death.
Diabetes
Diabetes associated with obesity, is a massive and a growing threat to public health37. The susceptibility of diabetes is 80 times greater among obese adults than nonobese. Professor Sir George Alberti, President of the International Diabetes Federation, has stated that those with a BMI of 35 have “a 92-fold increase in the risk of diabetes” compared with those with a BMI of 2238. The consequences associated with diabetes include: congestive heart disease, blindness, kidney failure, stroke, osteoarthritis, leg ulcers, and limb amputation. It was projected that there were 3 million (15%) diabetes patients living in the United Kingdom in 201039 and this is expected to increase to 70% in 2035. If the obesity trend continues the same way, by 2025 a quarter of the health budget will be spent on diabetes40.
Coronary heart disease (CHD)
CHD susceptibility increases 2–3 times more in obese adults. It is estimated that obesity accounts for 5% of CHD deaths in men and 6% in women40. If the obesity trend continues, it will increase from 10% in 2010 to 20% in 203541.
Cancer
Obese adults are 40% more likely to die from cancer than nonobese. Post menopausal obese women also have a higher risk of developing breast and endometrial cancers41. Although both obese men and women have a higher risk of developing cancers of the esophagous, colon, rectum, kidney, pancreas, thyroid, and gallbladder, cancer due to obesity accounts for 14% of deaths in men and 20% in women42. Obesity has been considered as the most important avoidable cause of cancer in nonsmokers, as proposed by Professor Julian Peto43. A recent survey showed that, although obesity is the main preventable risk factor after tobacco, only 3% of the UK population knew that cancer is associated with obesity44.
Osteoarthritis
Osteoarthritis associated with obesity affects the knees, hips, and the lower back by placing extra pressure on these joints and wearing away the cartilage44. This results in back, knee, and hip pain and therefore leading to difficulty in walking. More than 11 million working days are lost each year due to obesity in Britain and increasing prevalence means losing more days causing greater economic disruption45.
Emotional and psychological damage
Emotional and psychological problems due to obesity is a massive public health problem46. This results in lower self-esteem, anxiety, clinical depression, and suicidal attempts in extreme cases. Obese people are 3–4 times more likely to be depressed than nonobese47. Obese women are 37% more likely to commit suicide48. The emotional damage caused by obesity results in binge-eating, low confidence, social isolation, and humiliation49. Professor Hubert Lacey, from the Royal College of Psychiatrists said that obesity causes depression rather than depression causing obesity15.
Economic costs
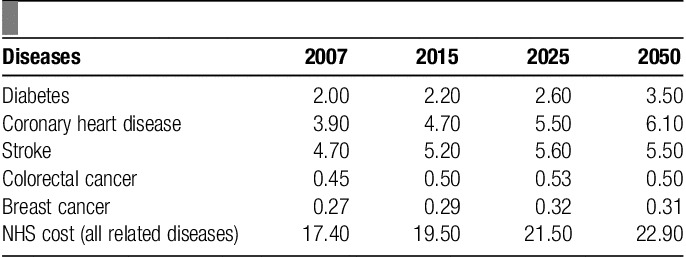
The increase in the prevalence of obesity will cause a significant impact on the National Health Service (NHS) budget. Other costs include: absence from work, morbidity not treated in the health service, and the affect on quality of life (Table 2).
Table 2.
Estimated future NHS costs of diseases related to body mass index, 2007–2050 (£billion/y).
In 1998, the direct cost of treating obesity and its associated consequences was £480 million (1.5% of NHS expenditure) and indirect costs such as loss of earnings and premature mortality was £2.1 billion, giving an overall total of £2.58 billion. It had been projected that the total figure would rise to £3.6 billion in 201050. However, due to the unexpected increases in the prevalence of obesity, NHS and drug costs from 1998 to 2010 has increased to £6.6–7.4 billion per year by the Clerk’s Department Scrutiny Unit51.
The health care costs associated with obesity among adults is higher among the middle aged52. As a consequence of increased cost and downward pressures on budgets, there may be increases in the cost of medicines, health care services, and taxes to compensate for the loss.
Conclusions
The gloomier picture of the likely threat that the increased prevalence of obesity possesses is concerning. If the trend continues unabated, in future decades the sight of overweight and obese individuals will be greater than the normal weight population on the streets of the United Kingdom. Ultimately, this will result in increase in the number of amputees, blind people, cancer patients, and the demand for kidney dialysis will increase subsequently. The positive trends of fighting heart disease (mainly due to reduced smoking) in the recent decades will be reversed. De facto, the increased prevalence of childhood obesity is so serious that as a consequence, this will be the first generation in which children will die before their parents in significant numbers52. Therefore, obesity is likely to supersede tobacco as the biggest cause of premature death. It is the responsibility of many government departments besides the Department of Health to tackle this amplifying issue53.
Acknowledgments
Conflict of interest statement
The authors declare that they have no financial conflict of interest with regard to the content of this report.
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Published online 22 June 2017
References
- 1.National Heart Lung and Blood Institute. Overweight and Obesity. 2010. Available at: www.nhlbi.nih.gov/health/dci/Diseases/obe/obe_whatare.html. Accessed March 4, 2012.
- 2.World Health Organization. Obesity and overweight. 2006. Available at: www.who.int/mediacentre/factsheets/fs311/en/index.html. Accessed March 28, 2012.
- 3.Centres for Disease Control and Prevention (CDC). Defining childhood overweight and obesity. 2011. Available at: www.cdc.gov/obesity/childhood/defining.html. Accessed March 6, 2012.
- 4.National Institute for Health and Clinical Excellence (NICE). Obesity: the prevention, identification, assessment and management of overweight and obesity in adults and children. 2006. Available at: www.nice.org.uk/guidance/CG43. Accessed March 12, 2012.
- 5.Weight Management Centre. Obesity—a public health crisis. 2010. Available at: www.wmc.uk.com/pdfs/Obesity%20Epidemic.pdf. Accessed January 14, 2012.
- 6.Marcus MD. Effects of obesity on the quality of life. 2002. Available at: www.endotext.org/obesity/obesity14/obesityframe14.htm. Accessed January 14, 2012.
- 7.Department for Business Innovation and Skills (BSI). Scoping the foresight project on tackling obesities: future choices. 2009. Available at: www.bis.gov.uk/foresight/our-work/projects/published-projects/tackling-obesities/reports-and-publications/results-of-scoping. Accessed March 12, 2012.
- 8.House of Commons Health Committee. Obesity third report session 2003-04. 2004. Available at: www.publications.parliament.uk/pa/cm200304/cmselect/cmhealth/23/23.pdf. Accessed March 17, 2012.
- 9.Patient UK. Obesity in adults. 2009. Available at: www.patient.co.uk/doctor/Obesity-Management-in-Adults.htm. Accessed March 4, 2012.
- 10.The NHS Information Centre. Statistics on obesity, physical activity and diet: England. 2010. Available at: www.ic.nhs.uk/webfiles/publications/opad10/Statistics_on_Obesity_Physical_Activity_and_Diet_England_2010.pdf. Accessed March 18, 2012.
- 11.Government Office for Science. Foresight—tackling obesities: future choices—modelling future trends in obesity & their impact on health. 2009. Available at: www.bis.gov.uk/assets/bispartners/foresight/docs/obesity/14.pdf. Accessed March 18, 2012.
- 12.Department of Health. Forecasting obesity 2010. 2006. Available at: www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/documents/digitalasset/dh_073033.pdf. Accessed March 19, 2012.
- 13.Lobstein T, Leach RJ. Foresight tackling obesities: future choices international comparisons of obesity trends, determinants and responses—evidence review. 2007. Available at: www.bis.gov.uk/assets/bispartners/foresight/docs/obesity/06%20part%2002.pdf. Accessed March 19, 2012.
- 14.Whitaker RC, Wright JA, Pepe MS, et al. Predicting obesity in young adulthood from childhood and parental obesity. N Engl J Med 1997;337:926.–. [DOI] [PubMed] [Google Scholar]
- 15.UK Parliament. Select Committee on health—third report. 2004. Available at: www.parliament.the-stationery-office.co.uk/pa/cm200304/cmselect/cmhealth/23/2304.htm#n37. Accessed March 10, 2012.
- 16.Jebb SA, Rennie KL, Cole TJ. Prevalence of overweight and obesity among young people in Great Britain. Public Health Nutrition 2003;7:461–5. [DOI] [PubMed] [Google Scholar]
- 17.Medical Research Council. Moderate obesity takes years off life expectancy, though not as many as smoking. 2009. Available at: www.mrc.ac.uk/Newspublications/News/MRC005722. Accessed March 17, 2012.
- 18.Royal College of Physicians of London. Storing up problems—the medical case for a slimmer nation. 2004. Available at: http://bookshop.rcplondon.ac.uk/contents/pub154-c4c29a84-e040-4293-be96-29a648a15fc9.pdf. Accessed March 17, 2012.
- 19.Science Daily. Moderate obesity takes years off life expectancy. 2009. Available at: www.sciencedaily.com/releases/2009/03/090319224823.htm. Accessed March 17, 2012.
- 20.Eisenberg ME, Neumark-Sztainer D, Story M. Associations of weight-based teasing and emotional well-being among adolescents. Arch Paediatr Adolesc Med 2003;157:733–8. [DOI] [PubMed] [Google Scholar]
- 21.Libbey HP, Story MT, Neumark-Sztainer DR, et al. Teasing, eating disordered behaviors and psychological morbidities among overweight adolescents. Obesity 2008;16:S24–9. [DOI] [PubMed] [Google Scholar]
- 22.Keery H, Boutelle K, van den Berg P, et al. The impact of appearance related teasing by family members. J Adolesc Health 2005;37:120–7. [DOI] [PubMed] [Google Scholar]
- 23.Northstone K, Joinson C, Emmett P, et al. Are dietary patterns in childhood associated with IQ at 8 years of age? A population-based cohort study. J Epidemiol Community Health 2010;66:624–8. [DOI] [PubMed] [Google Scholar]
- 24.World Health Organisation (WHO). The challenge of obesity in the WHO European Region and the strategies for response. 2007. Available at: www.euro.who.int/__data/assets/pdf_file/0010/74746/E90711.pdf. Accessed March 17, 2012.
- 25.Beydoun MA, Beydoun HA, Wang Y. Obesity and central obesity as risk factors for incident dementia and its subtypes: a systematic review and meta-analysis. Obes Rev 2008;9:204–18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Jensen GL. Obesity and functional decline: Epidemiology and geriatric consequences. Clin Geriatr Med 2005;21:677–87. [DOI] [PubMed] [Google Scholar]
- 27.Guralnik JM, Fried LP, Salive ME. Disability as a public health outcome in the aging population. Ann Rev Public Health 1996;17:25–46. [DOI] [PubMed] [Google Scholar]
- 28.Baumgartner RN, Wayne SJ, Waters D, et al. Sarcopenic obesity predicts instrumental activities of daily living disability in the elderly. Obes Res 2004;12:1995–2004. [DOI] [PubMed] [Google Scholar]
- 29.Villareal DT, Banks M, Siener C, et al. Physical frailty and body composition in obese elderly men and women. Obes Res 2004;12:913–20. [DOI] [PubMed] [Google Scholar]
- 30.Baumgartner RN. Body composition in healthy aging. Ann N Y Acad Sci 2000;904:437–48. [DOI] [PubMed] [Google Scholar]
- 31.Kelly C, Pashayan N, Munisamy S, et al. Mortality attributable to excess adiposity in England and Wales in 2003 and 2015: explorations with a spreadsheet implementation of the Comparative Risk Assessment methodology. Popul Health Metrics 2009;7:201–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.International Association for the Study of Obesity. Estimating the association between overweight and risk of disease. Available at: www.iaso.org/policy/healthimpactobesity/. Accessed March 18, 2012.
- 33.Ealing Primary Care Trust Local Care Group. Diabetes. 2006. Available at: www.ealingpct.nhs.uk. Accessed March 17, 2012.
- 34.Villareal DT, Apovian CM, Kushner RF, et al. Obesity in older adults: technical review and position statement of the American Society for Nutrition and NAASO, The Obesity Society. Am J Clin Nutr 2005;82:923–34. [DOI] [PubMed] [Google Scholar]
- 35.Agha M, Agha RA, Sandall J. Interventions to reduce and prevent obesity in pre-conceptual and pregnant women: a systematic review and meta-analysis. PLoS One 2014;9:e95132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Pajak A, Topor-Madry R, Waskiewicz A, et al. Body mass index and risk of death in middle-aged men and women in Poland Results of POL-MONICA cohort study. Kardologia Polska 2005;62:95–105. [PubMed] [Google Scholar]
- 37.Diabetes UK. Diabetes and obesity rates soar. 2009. Available at: www.diabetes.org.uk/About_us/News_Landing_Page/Diabetes-and-obesity-rates-soar/. Accessed March 17, 2012.
- 38.UK Parliament. Select committee on health minutes of evidence. 2003. Available at: www.parliament.the-stationery-office.co.uk/pa/cm200304/cmselect/cmhealth/23/3062604.htm. Accessed March 17, 2012.
- 39.Diabetes UK. Diabetes in the UK 2010: key statistics on diabetes. 2010. Available at: www.diabetes.org.uk/Documents/Reports/Diabetes_in_the_UK_2010.pdf. Accessed March 17, 2012.
- 40.Huff E. Twenty percent of hospital patients have diabetes. 2010. Available at: www.naturalnews.com/028487_hospitals_diabetes.html. Accessed March 17, 2012.
- 41.British Heart Foundation. Scotland coronary heart disease statistics 2009-10. 2010. Available at: www.bhf.org.uk/plugins/PublicationsSearchResults/DownloadFile.aspx?docid=ea0d5fc4-745c-412e-8bfe-64e71f4d1d4c&version=-1&title=G30S+Scotland+CHD+statistics+2009-10&resource=G30S%2F0210. Accessed March 17, 2012.
- 42.National Cancer Institute. Obesity and cancer: questions and answers. 2004. Available at: www.cancer.gov/cancertopics/factsheet/Risk/obesity. Accessed March 17, 2012.
- 43.BBC News. Obesity link to cancer. 2001. Available at: http://news.bbc.co.uk/1/hi/health/1334311.stm. Accessed March 17, 2012.
- 44.Smith D. Britons “unaware’ of links between obesity and cancer. 2004. Available at: www.guardian.co.uk/society/2004/apr/05/medicineandhealth.lifeandhealth?INTCMP=ILCNETTXT3487. Accessed March 17, 2012.
- 45.East Midlands Public Health. The real costs of obesity in the east midlands. What can your business do to help?. 2008. Available at: www.emphasisnetwork.org.uk/platform/downloads/WHATCANYOURBUSINESSDOTOHELP.pdf. Accessed March 17, 2012.
- 46.Willie N, Earhart M, Petersen C, et al. The impact of overweight and obesity on health-related quality of life in childhood – results from an intervention study. BMC Public Health 2008;421:8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Medical News Today. Women’s body image based more on others’ opinions than their own weight. 2011. Available at: www.medicalnewstoday.com/articles/220591.php. Accessed April 2, 2012.
- 48.Faculty of Public Health. Overweight and obesity: the public health problem. 1998. Available at: www.fph.org.uk/uploads/HealthyWeight_SectA.pdf. Accessed April 2, 2012.
- 49.Rush AJ. A study to investigate bariatric care in the community. 2002. Available at: www.safeliftingportal.com/hottopics/documents/OverviewofBariatricManagement.pdf. Accessed March 17, 2012.
- 50.NHS Primary Care Trusts. Tackling obesity—a strategy for children and adults in South West London (2006—10). 2010. Available at: www.mertonpartnership.org/mp-home/information-library/obesity06.pdf. Accessed March 17, 2012.
- 51.National Obesity Forum. Waist circumference. 2011. Available at: www.nationalobesityforum.org.uk/healthcare-professionals-mainmenu-155/assessment-mainmenu-168/171-waist-circumference.html. Accessed March 14, 2012.
- 52.Wee CC, Phillips RS, Legedza AT, et al. Health care expenditures associated with overweight and obesity among US adults: Importance of age and race. Am J Public Health 2005;95:159–65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Administration on Aging. Nutrition services (OAA Title IIIC). 2011. Available at: www.aoa.gov/AoARoot/AoA_Programs/HCLTC/Nutrition_Services/index.aspx. Accessed April 2, 2012.