

Abstract
Advances in surgical techniques have led to the survival of most patients with congenital heart disease (CHD) up to their adulthood. During their lifetime, many of them develop atrial tachyarrhythmias due to atrial dilatation and scarring from surgical procedures. More complex defects and palliative repairs are linked to a higher incidence and earlier occurrence of arrhythmias. Atrial fibrillation (AF) is common in patients who have atrial septal defects repaired after age 55 and in patients with tetralogy of Fallot repaired after age 45. Patients with dextrotransposition of the great arteries who undergo Mustard or Senning atrial switch procedures have an increased risk of atrial flutter due to atrial baffle suture lines. Patients with Ebstein’s anomaly are also prone to supraventricular tachycardias caused by accessory bypass tracts. Patients with a single ventricle who undergo Fontan palliation are at risk of developing persistent or permanent AF due to extreme atrial enlargement and hypertrophy. In addition, obtaining vascular access to the pulmonary venous atrium can present unique challenges during radiofrequency ablation for patients with a Fontan palliation. Patients with cyanotic CHD who develop AF have substantial morbidity because of limited hemodynamic reserve and a high viscosity state. Amiodarone is an effective therapy for patients with arrhythmias from CHD, but its use carries long-term risks for toxicity. Dofetilide and sotalol have good short-term effectiveness and are reasonable alternatives to amiodarone. Pulmonary vein isolation is associated with better outcomes in patients taking antiarrhythmic medications. Anticoagulants are challenging to prescribe for patients with CHD because of a lack of data that can be extrapolated to this patient population. Surgical ablation is the gold standard for invasive rhythm control in patients with CHD and should be considered at the time of surgical repair or revision of congenital heart defects. When possible, patients with complex CHD should be referred for care to an adult congenital heart disease center of excellence.
Keywords: Atrial Fibrillation, Fontan, Congenital Heart Disease
Introduction
Congenital heart defects occur in approximately 9 per 1,000 newborns and are responsible for nearly 30% of all major congenital birth defects.[1] In the modern era of advanced surgical techniques and postoperative care and management, more than 90% of children with congenital heart disease (CHD) will reach adulthood.[2],[3] The successful outcomes of the earlier surgical era have resulted in an ever-increasing number of adults with CHD. As of 2011, more adults than children are alive with CHD. Estimates suggest that there may be as many as 3 million adult survivors of CHD throughout North America and Europe. As this population has aged and the time from surgical palliation lengthened, new comorbidities have been increasingly recognized.[4] Repaired and unrepaired CHD is commonly associated with atrial tachyarrhythmias as a consequence of atrial dilatation, atrial scar, sinus nodal dysfunction, and congenital conduction system abnormalities.[5] Atrial tachyarrhythmias, including atrial fibrillation (AF), and atrial flutter, are associated with thromboembolic phenomena and hemodynamic compromise and are, thus, a major cause of morbidity and mortality in patients with and without CHD.[1]-[5] The higher incidence of AF is also linked to increasing rates of hospitalization and longer hospital stays, leading to higher use of health care resources. As the number of CHD patients continues to increase, a pressing need exists for effective and novel strategies to manage the care of these patients and yet minimize the impact on their otherwise complex pathophysiology. Our aim is to review the most recent literature for epidemiology, pathophysiology, and outcomes of available treatment modalities for AF and other atrial arrhythmias for patients with CHD.
Epidemiology
The incidence of AF in patients with CHD has been reported primarily for adults with simple, palliated CHD. The more complicated the congenital heart defect and the palliation required, the higher and earlier the incidence of atrial arrhythmias. Patients who underwent surgical closure of an atrial septal defect (ASD) before 15 years of age had a 0% incidence of AF and a 2% incidence of atrial flutter, confirmed by 24-hour Holter monitoring, at 33-year and 35-year follow-up in 2 studies.[6], [7] In contrast, the incidence of atrial arrhythmias was higher when ASD repair occurred during adulthood. [6],[7] In a study of 213 patients who underwent surgical closure of the ASD after age 40 years, 23% had AF or atrial flutter preoperatively.[8] Of these patients, only 60% continued to have these atrial arrhythmias during follow-up. Of the total patient cohort, an additional 2.9% developed new onset AF or atrial flutter. Predictors of late postoperative AF or atrial flutter were age greater than 40 years at the time of surgery, preoperative atrial flutter or fibrillation, and early postoperative atrial flutter or fibrillation or junctional rhythm. Similarly, patients who underwent percutaneous ASD closure after age 55 had an increased incidence of new onset atrial tachyarrhythmias.[9]
Tetralogy of Fallot is the most common cyanotic congenital heart defect, affecting 0.02% of live births. Tetralogy of Fallot is most commonly associated with ventricular tachycardia, although AF is also frequently observed. Khairy et al[10] reported a 7% overall prevalence of AF in 556 patients with tetralogy of Fallot. AF occurred more frequently in patients over age 45, with a prevalence of more than 30% by the age of 55. Similar to patients without CHD, AF in these patients is associated with increased left atrial volumes and may lead to a decrease in left ventricular systolic ejection fraction.
Before the arterial switch procedure for palliation of dextrotransposition of the great arteries (D-TGA) became common practice in the 1980s, the atrial switch procedure (Mustard or Senning) was the standard of care since the mid-1960s. As a result, there is a large, albeit finite, cohort of patients with this type of palliation moving through adulthood. After a Mustard procedure, sinus rhythm progressively deteriorates at a rate of 2.4% per year.[11] Patients often present with a junctional rhythm and are at increased risk of atrial flutter.[12] In a single-center study of patients with D-TGA who had undergone Mustard repair, 24% of patients had developed atrial flutter and 11% of patients had undergone pacemaker implantation at 20-year follow-up.[13]
Ebstein’s anomaly is a rare condition characterized by atrialization of the right ventricle and is frequently associated with additional structural defects, including persistent atrioventricular canal defects and accessory bypass tracts. Supraventricular tachycardias from rapid conduction through these accessory bypass tracts can result in profound hemodynamic compromise and even death. Chauvaud et al[14] evaluated 98 patients with Ebstein’s anomaly; 45 of the patients had preoperative arrhythmias, including 12 with AF or atrial flutter. Increasing age was a significant risk factor for the development of arrhythmia. Interestingly, preoperative tricuspid regurgitation, ASD, and severity of Ebstein’s anomaly were not associated with AF. Early postoperative AF developed in 8 patients, 6 of whom had preoperative AF. On follow-up, 5 patients with preoperative or early postoperative AF had recurrence, and 2 patients died suddenly.
Single ventricle disease, which encompasses tricuspid atresia, double-inlet left ventricle, double-outlet right ventricle, heterotaxy, and hypoplastic left heart syndrome, are the most complex CHD diagnoses. The final stage in palliation, the Fontan procedure, first performed in 1968, was established as a standard of care in the early 1970s. Peters et al[15] reported that 6 out of 60 patients (10%) who underwent a Fontan palliation had early postoperative AF. This was more frequently seen in patients with double-inlet left ventricle than in patients with tricuspid atresia. One patient had preoperative AF, with recurrence in the early postoperative period. All 6 patients in the study with early postoperative AF died because of progressive hemodynamic instability. During the follow-up period, another 3 patients developed AF. Fujita et al[16] reported on the incidence of postoperative AF in 199 patients with a single ventricle. After a follow-up period of 20 years, 16 patients (8%) had developed AF, 10 of whom had either persistent or permanent AF.
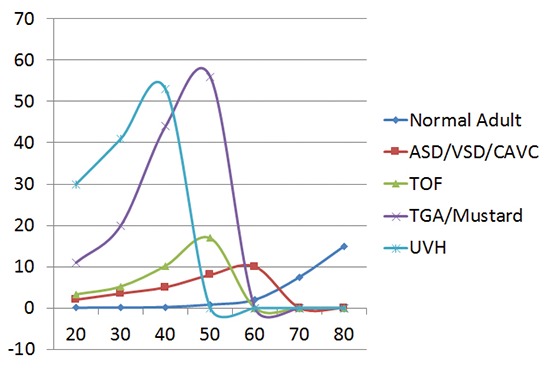
In CHD populations, AF develops with increasing age, increasing complexity of CHD, and increasing numbers of surgical interventions [Figure 1]. Acquired cardiovascular comorbidities, such as hypertension, obesity, sleep apnea, and coronary disease, will continue to occur in patients with CHD as they grow older, which will result in an increase in the incidence and burden of AF.
Figure 1. AP Fontan atrium obtained at time of transplant 2 weeks after 8mm high power RF ablation.

Panel A shows a low (4x) power cross section of right atrial tissue in an AP Fontan patient 2 weeks after RF ablation. Notice the extreme atrial hypertrophy with alternating areas of myocytes and fibrous connective tissue.
Panel B shows a higher (20x) magnification image showing residual areas of viable myocytes following extensive high power endocardial RF ablation.
Pathophysiology
In patient populations without cardiac structural abnormalities, there are well-established risk factors for the development of AF, including increasing age, hypertension, congestive heart failure, diabetes mellitus, obesity, obstructive sleep apnea, myocardial infarction, valvular heart disease, alcohol use, hyperthyroidism, cardiothoracic surgery, and left atrial enlargement on echocardiography.[17] In addition to these risk factors, patients with CHD have a unique set of risk factors specific to those with corrected and uncorrected lesions. These include atrial enlargement caused by ASD (primum, secundum, and sinus venosus), increased atrial volume after operative intervention, and Fontan palliation. Atrial scarring leading to arrhythmogenic foci may develop after surgical repair of an ASD or patent foramen ovale, unifocalization of anomalous pulmonary venous return, repair of coronary fistulae, or construction of an interatrial baffle during an atrial switch procedure (ie, Mustard or Senning).[18] [Figure 2] The scars created by atrial baffles also provide an ideal environment for isthmus-dependent atrial flutter although the isthmus is located on the pulmonary venous side of the baffle. After a Mustard procedure, atrial flutter is associated with an increased risk of sudden death, which may be related to rapid ventricular response from 1:1 atrioventricular conduction or from further impairment of ventricular filling, reducing cardiac output.[19]
Figure 2. A and B. Pulmonary Vein focus driving coarse atrial fibrillation in a patient with complex atrioventricular septal defect repair. C. pulmonary vein pre-ablation D. pulmonary vein post-ablation.

Fontan surgical procedures create multiple right atrial scars and Fontan hemodynamics create atrial enlargement and hypertrophy which also increase the risk of atypical atrial flutters (incisional reentry or IART) as well as AF. Specific sequelae of the Fontan procedure that further increase this risk include right atrial gigantism with subsequent right upper pulmonary vein compression, as well as right atrial substrate changes, such as hypertrophy of the right atrial wall. Approximately 50% of patients with right atrial–right ventricular or atriopulmonary Fontan procedures develop atrial tachycardia within 10 years of their palliative procedure. Risk factors include older age at palliation and increased time to follow-up.[20] Improved surgical techniques have begun to improve risks, which will benefit future patients.
Congenital structural abnormalities allow for the development of AF attributable to effects on the conduction system. One such example is Ebstein’s anomaly, which is associated with the presence of accessory bypass tracts, as well as a fractured conduction system.[13] Surgical palliation of CHD places patients at risk for the development of postoperative AF, which is similar to that of adult patients without CHD who undergo other cardiac surgical procedures. Many CHD patients have had multiple cardiac and non-cardiac operations before the age of 18, and each episode of postoperative AF has a cumulative risk for the further development of AF that is not related to surgery. With each such episode, the underlying atrial substrate undergoes fundamental changes.[21], [22]
Patients with CHD are more likely to have comorbid conditions that contribute to the risk of developing AF, including scoliosis with pulmonary restriction, pulmonary hypertension, and premature systemic hypertension. Patients with cyanosis are also at increased risk for AF due to chronic subendocardial ischemia. Their baseline hemodynamic state is precarious, with limited oxygen reserves and a high viscosity state.[23] If patients with CHD develop AF, they are more likely to have substantial morbidity due to poorly tolerated rapid rates and thromboembolic events. Compared with patients who do not have CHD, patients with CHD develop AF at a younger age, and their AF is more challenging to manage medically, minimally invasively, or surgically.
Pharmacotherapy
AF is poorly tolerated in patients with CHD and requires multimodality and multidrug regimens for adequate rhythm control. Limited knowledge exists regarding safety and efficacy of drug therapy in CHD. Class I antiarrhythmic agents can depress ventricular function, particularly in patients with decreased systolic ejection fraction.[24] Of the class IA agents, quinidine carries a black box warning for use in structural heart disease, and procainamide is relatively contraindicated in the setting of depressed myocardial contractility. The class IC agents, propafenone and flecainide, are relatively contraindicated in structural heart disease, including after a myocardial infarction.[25] They also increase the defibrillation threshold in patients with implantable cardioverter defibrillators (ICDs).[26]-[28] Although class IC agents may be useful for CHD patients with AF who also have an ICD, little data are available to support their use in this setting. The use of non-dihydropyridine calcium channel blockers, verapamil and diltiazem, should be avoided in those with more than mild systemic ventricular dysfunction because they cause depressed myocardial contractility.
Amiodarone has been used for adults since the 1960s and is widely considered to be the most effective antiarrhythmic drug, even for the CHD population. Amiodarone is effective at controlling incessant postoperative atrial arrhythmias, including junctional ectopic tachycardia.[29] It should be administered with caution in adolescents and children because of its daunting long-term side-effect profile, which includes thyroid dysfunction, pulmonary fibrosis, hepatic dysfunction, and corneal deposition.[30] Patients with CHD are more likely to present with arrhythmias that are refractory to single-drug therapy, demonstrate depressed myocardial function, and have an intolerance of agents with negative inotropic effects.[31] Amiodarone also carries additional risks for toxicity in patients with CHD, particularly women, patients with unrepaired cyanotic lesions, and patients who have a prior history of Fontan-type palliation.[32] Close monitoring is necessary in these high-risk groups.[33]
Other class III antiarrhythmic agents have also been used with variable success to manage atrial arrhythmias in patients with CHD. In a small, multicenter, retrospective review of dofetilide treatment in CHD patients with AF, 85% of patients initially responded well, and 55% were free from arrhythmia at 1-year follow-up. Long-term suppression was achieved in 35% of patients.[34] In a study of sotalol treatment in children after palliative surgery for CHD, freedom from arrhythmia was observed to be 96% and 81% after 1 and 2 years, respectively.[35] In a study of CHD patients with refractory tachyarrhythmias treated with sotalol, complete rhythm control was achieved in 41% of patients, and partial rhythm control was achieved in 35% of patients at 13-month follow-up.[36] Amiodarone, dofetilide, and sotalol should all be initiated at lower doses in patients with CHD because medication toxicity appears to be higher. Additionally, intravenous ibutilide has also demonstrated a 71% success rate in cardioverting AF and atrial flutter in children with CHD, which is comparable to the success rate in non-CHD populations.[37]
Anticoagulation is recommended for AF to decrease the risk of thromboembolic phenomena. The 2014 management guidelines for AF recommend anticoagulation for a CHA2DS2-VASc score of 1 or more; however, this scoring system has not been validated for CHD patients.[17] Patients with CHD and atrial tachyarrhythmias have been reported to have a 42% prevalence of left or right atrial thrombi during preprocedural transesophageal echocardiography before cardioversion.[38] Fortunately, thromboembolic stroke after cardioversion appears to be rare, particularly in patients with a single atrium or single ventricle. Additionally, patients with single ventricle who have undergone surgical repair before the routine use of the Damus-Kaye-Stansel reconstruction have a pulmonary artery stump that is oversewn with a resultant pulsatile swirling of blood, creating a high-risk nidus for thrombus formation. This type of repair necessitates life-long anticoagulation even in the setting of normal rhythm.[39] Patients with Fontan repairs are uniquely challenging because they are likely to develop progressive cardiac cirrhosis, leading to changes in the intrinsic and extrinsic clotting cascade. Such changes may increase the risk of both bleeding and thrombosis due to decreased production of vitamin K–dependent clotting factors (factors II, VII, IX, and X), as well as the anticoagulants protein C and protein S.40 Additionally, the novel oral anticoagulants dabigatran, rivaroxaban, apixaban, and edoxaban do not have indications or data to support their use in patients with CHD. Thus peri procedural and long term anticoagulation in this group of patients is largely accomplished through the use of well monitored warfarin and/or LMW heparin.
Transcatheter Therapies
The pathophysiology of AF in CHD appears to be comparable to that of normal adults in that pulmonary vein foci drive coarse AF. Isolation of the pulmonary veins through radiofrequency ablation appears to be of comparable therapeutic benefit. [Figure 3]. Only one study to date has evaluated the success of pulmonary vein isolation in patients with complex CHD, which included 36 patients with CHD and drug-refractory AF who underwent pulmonary vein isolation.[41] Freedom from symptomatic AF at 300 days post-ablation was 42% in patients in the absence of antiarrhythmic therapy and 84% in patients taking antiarrhythmic therapy. At 4-year follow-up, these success rates decreased to 27% and 61%, respectively. Additionally, atypical atrial flutter may mimic AF on the surface electrocardiogram [Figure 4]; however, the true mechanism of arrhythmia may only become apparent during an electrophysiologic study at the time of ablation. An electrophysiology study revealed rapid scar based left atrial intraatrial reentrant tachycardia with a slowly conducting critical zone accounting for 97/205 milliseconds of the atrial flutter cycle length. Ablation of the critical zone resulted in atrial flutter termination.
Figure 3. Automaticity demonstrated pre-and post ablation in a patient with single ventricle heart disease who is status post-Fontan.

Figure 4. Prevalence of atrial fibrillation by age and defect.
1.Stefansdottir H, Aspelund T, Gudnason T, Arnar DO. Trends in the incidence and prevalence of atrial fibrillation in Iceland and future projections. Europace 2011;13:1110–7.
2.Teuwen C, Ramdjan T, Gotte M, Brundel B, Evertz, Vriend J, Molhoek S, Dorman H, Opstal J, Konings T, van der Voort P, Delacretaz E, Houck C, Yaksh A, Jansz L, Witsenburg M, Roos-Hesselink J, Triedman J Bogers A, de Groot N. Circ: Arrhythmia and EP. 2015;8:1065-72.
Obtaining vascular access for ablation procedures in CHD patients may be challenging due to the presence of scar tissue, particularly in patients who have had a number of cardiac catheterization procedures, percutaneously inserted central lines, or periods of extracorporeal membrane oxygenation. Femoral and internal jugular venous access sites are also frequently occluded. In order to use catheter-based ablation techniques, the first hurdle to overcome is access into the pulmonary venous atrium. Although the incidence of atrial tachycardia after Fontan surgery is high, access to the pulmonary venous atrium, a frequent site of arrhythmia origin, is often limited. Thus conventional transseptal access to the left atrium is usually achievable in those CHD patients with a separated 2 ventricle circulation. In Fontan patients, transseptal access is largely limited to those with an “old style” atriopulmonary Fontan and can be quite challenging due to the degree of atrial enlargement and hypertrophy and the lack of commercially available appropriately sized transeptal catheters. In atrial switch (Mustard or Senning) patients, transcatheter access to the pulmonary veins can only be accomplished with a magnetic navigation catheter ablation system.
The transhepatic approach is well documented in a number of fields, with indications for treatment of portal hypertension, hemodialysis, and also catheter-based ablation therapies.[42],[43] Under fluoroscopic and ultrasound guidance, a percutaneous needle is advanced into a hepatic vein and exchanged for a vascular sheath over a wire. Catheters are then advanced into the systemic venous atrium for mapping and ablation.[44] This approach is useful in those CHD patients with acquired occlusion of the IVC and those patients with heterotaxy syndrome and congenital interruption of the IVC with azygous vein continuation. The presence of conventional basket type IVC filters has not been a significant impediment to catheterization.
Transthoracic percutaneous access with fluoroscopic guidance provides a direct route to the pulmonary venous atrium for successful mapping and radiofrequency ablation in patients after a Fontan palliation. Nehgme et al[45] performed 6 transthoracic ablation procedures in patients with a lateral-tunnel Fontan. Under biplane fluoroscopy, a percutaneous needle was advanced toward the pulmonary venous atrium. Mapping and ablation catheters were placed in the atrium, and additional catheters were placed in the baffle and esophagus for pacing and reference. Complications included 1 pneumothorax and 2 hemothoraces that were drained. Another new procedure that was recently described involves a CT-guided transconduit puncture in patients with an extracardiac Fontan, in which the dilator tip is grasped with a snare catheter.[46] Subxiphoid and epicardial approaches may be used in patients without CHD, however, they are generally not employed for patients with CHD.[47] Both these approaches rely on the ability to access the pericardial sac in patients who have had multiple sternotomies. Nevertheless, these patients frequently have a pericardium that is immobile and often scarred with thick adhesions.[48]
Surgical Therapies
Surgical ablation is considered the gold standard for invasive rhythm control in patients with CHD. The initial surgical treatment of CHD with concomitant surgical ablation began with an atriopulmonary to total cavopulmonary Fontan conversion performed in conjunction with surgical ablation for AF.[49] Fontan conversion that did not include surgical ablation has been associated with a high incidence of atrial arrhythmias postoperatively.[50] The surgical approach has since progressed from isthmus ablation, to a modified right-sided maze procedure, and eventually to the MAZE-Cox III (right and left-sided maze) procedure for AF.[51],[52] Referral for surgical ablation includes patients for whom catheter ablation has failed, patients with concomitant CHD and arrhythmias, and patients with low body mass for whom size precludes the use of catheter-based approaches.[53],[54] In one study, ablative surgery during surgical revision of complex congenital heart defects had a 93% success rate with approximately 7% rate of recurrence.[55] A right-sided atrial maze performed during surgical repair of Ebstein’s anomaly has also been associated with good short-term outcomes.[56]
A surgical approach that incorporates a modification to the Fontan for the prophylaxis of intraatrial reentrant tachycardia should be considered as a part of preoperative planning. In a small feasibility study, an interventional atrial incision placed during the Fontan operation resulted in an increase in intraatrial conduction time without any spontaneous or inducible intraatrial reentrant tachycardias during electrophysiologic testing.[57] Although the procedure was shown to fundamentally change the atrial substrate, its long-term efficacy in reducing the incidence of intraatrial reentrant tachycardias is unknown.
A hybrid approach may be useful in select situations, for example, in patients with tetralogy of Fallot and inducible ventricular tachycardia on electrophysiologic testing before they undergo thoracotomy for other congenital cardiac surgery.[58],[59] With 3-dimensional mapping and pace-mapping techniques, the focus of ventricular arrhythmias can by marked by an ablation catheter. This allows for the localization and surgical excision of the arrhythmogenic tissue, thereby substantially reducing the possibility of future ventricular arrhythmias and resultant ICD discharges.[60] Patients with a single ventricle that are scheduled to undergo Fontan revision may be appropriate candidates for similar hybrid approaches that include surgical resection of arrhythmogenic atrial tissue. With advanced planning, patients undergoing open-thoracotomy procedures can have epicardial leads placed intraoperatively, potentially avoiding another open thoracotomy if they develop a pacing indication in the future.
Care of patients who have undergone Fontan palliation continues to be challenging both from an arrhythmia and an access perspective. Fontan surgery has progressed from a classic Fontan (right atrial to pulmonary artery), to a lateral-tunnel Fontan (inferior vena cava and superior vena cava to the pulmonary artery within the right atrium), and finally to an extracardiac Fontan circuit. Each of these procedures has a unique set of access and arrhythmia challenges.[61]-[63] Therefore, any opportunity to perform a surgical ablation during an open-thoracotomy procedure should be considered as a part of the preoperative planning discussion. Finally, elective surgical excision of thrombogenic structures such as the left atrial appendage and residual ligated blind ended pulmonary artery stump should be performed at the time of concomitant open heart cardiac surgical repairs.
Conclusions
The adult CHD population is increasing rapidly, and patients with CHD are more likely to be referred for cardiac electrophysiology procedures. AF occurs at a younger age in patients with CHD who are less tolerant of the arrhythmia and whose comorbid conditions make medical arrhythmia therapy more difficult to manage. Multiple drugs and many interventions will likely be required. Amiodarone is an effective antiarrhythmic agent but has long-term toxicity risks for this young population but is a very good short term bridging therapy; dofetilide and sotalol may be viable long term alternatives. Before any catheter-based therapy is undertaken, identification of vascular access to the systemic and pulmonary venous atria is essential. This generally mandates the use of advanced imaging such as CT or MRI with 3D reconstruction. Any time an open-thoracotomy operation is planned, a discussion of concomitant surgical ablation of the arrhythmogenic substrate and excision or exclusion of residual thrombogenic structures should occur. A preoperative diagnostic EP study without ablation is often useful in guiding subsequent surgical ablation. In conclusion, patients with complicated CHD and atrial arrhythmias should have the benefit of referral to or collaboration with an adult congenital center of excellence prior to invasive rhythm management therapies.
Conflict Of Interests
None.
Disclosures
None.
References
- 1.van der Linde Denise, Konings Elisabeth E M, Slager Maarten A, Witsenburg Maarten, Helbing Willem A, Takkenberg Johanna J M, Roos-Hesselink Jolien W. Birth prevalence of congenital heart disease worldwide: a systematic review and meta-analysis. J. Am. Coll. Cardiol. 2011 Nov 15;58 (21):2241–7. doi: 10.1016/j.jacc.2011.08.025. [DOI] [PubMed] [Google Scholar]
- 2.Moons Philip, Bovijn Lore, Budts Werner, Belmans Ann, Gewillig Marc. Temporal trends in survival to adulthood among patients born with congenital heart disease from 1970 to 1992 in Belgium. Circulation. 2010 Nov 30;122 (22):2264–72. doi: 10.1161/CIRCULATIONAHA.110.946343. [DOI] [PubMed] [Google Scholar]
- 3.Warnes C A, Liberthson R, Danielson G K, Dore A, Harris L, Hoffman J I, Somerville J, Williams R G, Webb G D. Task force 1: the changing profile of congenital heart disease in adult life. J. Am. Coll. Cardiol. 2001 Apr;37 (5):1170–5. doi: 10.1016/s0735-1097(01)01272-4. [DOI] [PubMed] [Google Scholar]
- 4.Giamberti Alessandro, Chessa Massimo, Abella Raul, Butera Gianfranco, Negura Diana, Foresti Sara, Carminati Mario, Cappato Riccardo, Frigiola Alessandro. Surgical treatment of arrhythmias in adults with congenital heart defects. Int. J. Cardiol. 2008 Sep 16;129 (1):37–41. doi: 10.1016/j.ijcard.2007.06.019. [DOI] [PubMed] [Google Scholar]
- 5.Mavroudis Constantine, Deal Barbara J, Backer Carl L. Surgery for arrhythmias in children. Int. J. Cardiol. 2004 Dec;97 Suppl 1 ():39–51. doi: 10.1016/j.ijcard.2004.08.008. [DOI] [PubMed] [Google Scholar]
- 6.Roos-Hesselink J W, Meijboom F J, Spitaels S E C, van Domburg R, van Rijen E H M, Utens E M W J, Bogers A J J C, Simoons M L. Excellent survival and low incidence of arrhythmias, stroke and heart failure long-term after surgical ASD closure at young age. A prospective follow-up study of 21-33 years. Eur. Heart J. 2003 Jan;24 (2):190–7. doi: 10.1016/s0195-668x(02)00383-4. [DOI] [PubMed] [Google Scholar]
- 7.Cuypers Judith A A E, Opić Petra, Menting Myrthe E, Utens Elisabeth M W J, Witsenburg Maarten, Helbing Wim A, van den Bosch Annemien E, Ouhlous Mohamed, van Domburg Ron T, Meijboom Folkert J, Bogers Ad J J C, Roos-Hesselink Jolien W. The unnatural history of an atrial septal defect: longitudinal 35 year follow up after surgical closure at young age. Heart. 2013 Sep;99 (18):1346–52. doi: 10.1136/heartjnl-2013-304225. [DOI] [PubMed] [Google Scholar]
- 8.Gatzoulis M A, Freeman M A, Siu S C, Webb G D, Harris L. Atrial arrhythmia after surgical closure of atrial septal defects in adults. N. Engl. J. Med. 1999 Mar 18;340 (11):839–46. doi: 10.1056/NEJM199903183401103. [DOI] [PubMed] [Google Scholar]
- 9.Silversides Candice K, Haberer Kym, Siu Samuel C, Webb Gary D, Benson Lee N, McLaughlin Peter R, Harris Louise. Predictors of atrial arrhythmias after device closure of secundum type atrial septal defects in adults. Am. J. Cardiol. 2008 Mar 01;101 (5):683–7. doi: 10.1016/j.amjcard.2007.10.035. [DOI] [PubMed] [Google Scholar]
- 10.Khairy Paul, Aboulhosn Jamil, Gurvitz Michelle Z, Opotowsky Alexander R, Mongeon François-Pierre, Kay Joseph, Valente Anne Marie, Earing Michael G, Lui George, Gersony Deborah R, Cook Stephen, Ting Jennifer Grando, Nickolaus Michelle J, Webb Gary, Landzberg Michael J, Broberg Craig S. Arrhythmia burden in adults with surgically repaired tetralogy of Fallot: a multi-institutional study. Circulation. 2010 Aug 31;122 (9):868–75. doi: 10.1161/CIRCULATIONAHA.109.928481. [DOI] [PubMed] [Google Scholar]
- 11.Haeffele Christiane, Lui George K. Dextro-Transposition of the Great Arteries: Long-term Sequelae of Atrial and Arterial Switch. Cardiol Clin. 2015 Nov;33 (4):543–58, viii. doi: 10.1016/j.ccl.2015.07.012. [DOI] [PubMed] [Google Scholar]
- 12.Gelatt M, Hamilton R M, McCrindle B W, Connelly M, Davis A, Harris L, Gow R M, Williams W G, Trusler G A, Freedom R M. Arrhythmia and mortality after the Mustard procedure: a 30-year single-center experience. J. Am. Coll. Cardiol. 1997 Jan;29 (1):194–201. doi: 10.1016/s0735-1097(96)00424-x. [DOI] [PubMed] [Google Scholar]
- 13.Gillette P C, el-Said G M, Sivarajan N, Mullins C E, Williams R L, McNamara D G. Electrophysiological abnormalities after Mustard's operation for transposition of the great arteries. Br Heart J. 1974 Feb;36 (2):186–91. doi: 10.1136/hrt.36.2.186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Chauvaud S M, Brancaccio G, Carpentier A F. Cardiac arrhythmia in patients undergoing surgical repair of Ebstein's anomaly. Ann. Thorac. Surg. 2001 May;71 (5):1547–52. doi: 10.1016/s0003-4975(01)02464-x. [DOI] [PubMed] [Google Scholar]
- 15.Peters N S, Somerville J. Arrhythmias after the Fontan procedure. Br Heart J. 1992 Aug;68 (2):199–204. doi: 10.1136/hrt.68.8.199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Fujita Shuhei, Takahashi Kazuhiro, Takeuchi Daiji, Manaka Tetsuyuki, Shoda Morio, Hagiwara Nobuhisa, Kurosawa Hiromi, Nakanishi Toshio. Management of late atrial tachyarrhythmia long after Fontan operation. J Cardiol. 2009 Jun;53 (3):410–6. doi: 10.1016/j.jjcc.2009.01.009. [DOI] [PubMed] [Google Scholar]
- 17.January Craig T, Wann L Samuel, Alpert Joseph S, Calkins Hugh, Cigarroa Joaquin E, Cleveland Joseph C, Conti Jamie B, Ellinor Patrick T, Ezekowitz Michael D, Field Michael E, Murray Katherine T, Sacco Ralph L, Stevenson William G, Tchou Patrick J, Tracy Cynthia M, Yancy Clyde W. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J. Am. Coll. Cardiol. 2014 Dec 02;64 (21):e1–76. doi: 10.1016/j.jacc.2014.03.022. [DOI] [PubMed] [Google Scholar]
- 18.Walsh Edward P, Cecchin Frank. Arrhythmias in adult patients with congenital heart disease. Circulation. 2007 Jan 30;115 (4):534–45. doi: 10.1161/CIRCULATIONAHA.105.592410. [DOI] [PubMed] [Google Scholar]
- 19.Dos L, Teruel L, Ferreira I J, Rodriguez-Larrea J, Miro L, Girona J, Albert D C, Gonçalves A, Murtra M, Casaldaliga J. Late outcome of Senning and Mustard procedures for correction of transposition of the great arteries. Heart. 2005 May;91 (5):652–6. doi: 10.1136/hrt.2003.029769. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Durongpisitkul K, Porter C J, Cetta F, Offord K P, Slezak J M, Puga F J, Schaff H V, Danielson G K, Driscoll D J. Predictors of early- and late-onset supraventricular tachyarrhythmias after Fontan operation. Circulation. 1998 Sep 15;98 (11):1099–107. doi: 10.1161/01.cir.98.11.1099. [DOI] [PubMed] [Google Scholar]
- 21.Shinagawa Kaori, Li Danshi, Leung Tack Ki, Nattel Stanley. Consequences of atrial tachycardia-induced remodeling depend on the preexisting atrial substrate. Circulation. 2002 Jan 15;105 (2):251–7. doi: 10.1161/hc0202.102014. [DOI] [PubMed] [Google Scholar]
- 22.Nattel Stanley. New ideas about atrial fibrillation 50 years on. Nature. 2002 Jan 10;415 (6868):219–26. doi: 10.1038/415219a. [DOI] [PubMed] [Google Scholar]
- 23.Gelatt M, Hamilton R M, McCrindle B W, Gow R M, Williams W G, Trusler G A, Freedom R M. Risk factors for atrial tachyarrhythmias after the Fontan operation. J. Am. Coll. Cardiol. 1994 Dec;24 (7):1735–41. doi: 10.1016/0735-1097(94)90181-3. [DOI] [PubMed] [Google Scholar]
- 24.Stambler B S, Gottlieb S S, Singh B N, Ramanathan K B, Ogilby J D, Ellenbogen K A. Hemodynamic effects of intravenous sematilide in patients with congestive heart failure: a class III antiarrhythmic agent without cardiodepressant effects. J. Am. Coll. Cardiol. 1995 Dec;26 (7):1679–84. doi: 10.1016/0735-1097(95)00376-2. [DOI] [PubMed] [Google Scholar]
- 25.Echt D S, Liebson P R, Mitchell L B, Peters R W, Obias-Manno D, Barker A H, Arensberg D, Baker A, Friedman L, Greene H L. Mortality and morbidity in patients receiving encainide, flecainide, or placebo. The Cardiac Arrhythmia Suppression Trial. N. Engl. J. Med. 1991 Mar 21;324 (12):781–8. doi: 10.1056/NEJM199103213241201. [DOI] [PubMed] [Google Scholar]
- 26.Dorian P, Fain E S, Davy J M, Winkle R A. Lidocaine causes a reversible, concentration-dependent increase in defibrillation energy requirements. J. Am. Coll. Cardiol. 1986 Aug;8 (2):327–32. doi: 10.1016/s0735-1097(86)80047-x. [DOI] [PubMed] [Google Scholar]
- 27.Fain E S, Dorian P, Davy J M, Kates R E, Winkle R A. Effects of encainide and its metabolites on energy requirements for defibrillation. Circulation. 1986 Jun;73 (6):1334–41. doi: 10.1161/01.cir.73.6.1334. [DOI] [PubMed] [Google Scholar]
- 28.Echt D S, Gremillion S T, Lee J T, Roden D M, Murray K T, Borganelli M, Crawford D M, Stewart J R, Hammon J W. Effects of procainamide and lidocaine on defibrillation energy requirements in patients receiving implantable cardioverter defibrillator devices. J. Cardiovasc. Electrophysiol. 1994 Sep;5 (9):752–60. doi: 10.1111/j.1540-8167.1994.tb01198.x. [DOI] [PubMed] [Google Scholar]
- 29.Saul J Philip, Scott William A, Brown Stephen, Marantz Pablo, Acevedo Valeria, Etheridge Susan P, Perry James C, Triedman John K, Burriss Susan W, Cargo Paul, Graepel Jay, Koskelo Eeva-Kaarina, Wang Rebecca. Intravenous amiodarone for incessant tachyarrhythmias in children: a randomized, double-blind, antiarrhythmic drug trial. Circulation. 2005 Nov 29;112 (22):3470–7. doi: 10.1161/CIRCULATIONAHA.105.534149. [DOI] [PubMed] [Google Scholar]
- 30.Labombarda Fabien, Ou Phalla, Stos Bertrand, de Blic Jacques, Villain Elisabeth, Sidi Daniel. Acute amiodarone-induced pulmonary toxicity: an association of risk factors in a child operated by arterial switch operation. Congenit Heart Dis. 2008 Oct 8;3 (5):365–7. doi: 10.1111/j.1747-0803.2008.00208.x. [DOI] [PubMed] [Google Scholar]
- 31.Haas Nikolaus A, Camphausen Christoph K. Impact of early and standardized treatment with amiodarone on therapeutic success and outcome in pediatric patients with postoperative tachyarrhythmia. J. Thorac. Cardiovasc. Surg. 2008 Nov;136 (5):1215–22. doi: 10.1016/j.jtcvs.2008.04.011. [DOI] [PubMed] [Google Scholar]
- 32.Thorne S A, Barnes I, Cullinan P, Somerville J. Amiodarone-associated thyroid dysfunction: risk factors in adults with congenital heart disease. Circulation. 1999 Jul 13;100 (2):149–54. doi: 10.1161/01.cir.100.2.149. [DOI] [PubMed] [Google Scholar]
- 33.Pratap R, Qayyum A, Ahmad N, Jani P. Surgical management of amiodarone-induced thyrotoxicosis in a patient with Eisenmenger's syndrome: literature review and case report. J Laryngol Otol. 2009 Nov;123 (11):1276–9. doi: 10.1017/S0022215108004167. [DOI] [PubMed] [Google Scholar]
- 34.Wells Ronald, Khairy Paul, Harris Louise, Anderson C Christian, Balaji Seshadri. Dofetilide for atrial arrhythmias in congenital heart disease: a multicenter study. Pacing Clin Electrophysiol. 2009 Oct;32 (10):1313–8. doi: 10.1111/j.1540-8159.2009.02479.x. [DOI] [PubMed] [Google Scholar]
- 35.Beaufort-Krol G C, Bink-Boelkens M T. Sotalol for atrial tachycardias after surgery for congenital heart disease. Pacing Clin Electrophysiol. 1997 Aug;20 (8 Pt 2):2125–9. doi: 10.1111/j.1540-8159.1997.tb03642.x. [DOI] [PubMed] [Google Scholar]
- 36.Miyazaki Aya, Ohuchi Hideo, Kurosaki Ken-ichi, Kamakura Shiro, Yagihara Toshikatsu, Yamada Osamu. Efficacy and safety of sotalol for refractory tachyarrhythmias in congenital heart disease. Circ. J. 2008 Dec;72 (12):1998–2003. doi: 10.1253/circj.cj-08-0194. [DOI] [PubMed] [Google Scholar]
- 37.Hoyer Andrew W, Balaji Seshadri. The safety and efficacy of ibutilide in children and in patients with congenital heart disease. Pacing Clin Electrophysiol. 2007 Aug;30 (8):1003–8. doi: 10.1111/j.1540-8159.2007.00799.x. [DOI] [PubMed] [Google Scholar]
- 38.Feltes T F, Friedman R A. Transesophageal echocardiographic detection of atrial thrombi in patients with nonfibrillation atrial tachyarrhythmias and congenital heart disease. J. Am. Coll. Cardiol. 1994 Nov 01;24 (5):1365–70. doi: 10.1016/0735-1097(94)90121-x. [DOI] [PubMed] [Google Scholar]
- 39.Oski J A, Canter C E, Spray T L, Kan J S, Cameron D E, Murphy A M. Embolic stroke after ligation of the pulmonary artery in patients with functional single ventricle. Am. Heart J. 1996 Oct;132 (4):836–40. doi: 10.1016/s0002-8703(96)90319-1. [DOI] [PubMed] [Google Scholar]
- 40.Amarapurkar Pooja D, Amarapurkar Deepak N. Management of coagulopathy in patients with decompensated liver cirrhosis. Int J Hepatol. 2011;2011 () doi: 10.4061/2011/695470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Philip Femi, Muhammad Kamran I, Agarwal Shikar, Natale Andrea, Krasuski Richard A. Pulmonary vein isolation for the treatment of drug-refractory atrial fibrillation in adults with congenital heart disease. Congenit Heart Dis. 2012 Apr 4;7 (4):392–9. doi: 10.1111/j.1747-0803.2012.00649.x. [DOI] [PubMed] [Google Scholar]
- 42.Stavropoulos S William, Pan John J, Clark Timothy W I, Soulen Michael C, Shlansky-Goldberg Richard D, Itkin Maxim, Trerotola Scott O. Percutaneous transhepatic venous access for hemodialysis. J Vasc Interv Radiol. 2003 Sep;14 (9 Pt 1):1187–90. doi: 10.1097/01.rvi.0000085770.63355.f2. [DOI] [PubMed] [Google Scholar]
- 43.Johnson J L, Fellows K E, Murphy J D. Transhepatic central venous access for cardiac catheterization and radiologic intervention. Cathet Cardiovasc Diagn. 1995 Jun;35 (2):168–71. doi: 10.1002/ccd.1810350219. [DOI] [PubMed] [Google Scholar]
- 44.Nguyen Duy Thai, Gupta Rajan, Kay Joseph, Fagan Thomas, Lowery Christopher, Collins Kathryn K, Sauer William H. Percutaneous transhepatic access for catheter ablation of cardiac arrhythmias. Europace. 2013 Apr;15 (4):494–500. doi: 10.1093/europace/eus315. [DOI] [PubMed] [Google Scholar]
- 45.Nehgme Rodrigo A, Carboni Michael P, Care Jennifer, Murphy John D. Transthoracic percutaneous access for electroanatomic mapping and catheter ablation of atrial tachycardia in patients with a lateral tunnel Fontan. Heart Rhythm. 2006 Jan;3 (1):37–43. doi: 10.1016/j.hrthm.2005.09.027. [DOI] [PubMed] [Google Scholar]
- 46.Aoki Hisaaki, Nakamura Yoshihide, Takeno Satoru, Takemura Tsukasa. A new procedure for a trans-conduit puncture by grasping the dilator tip with a snare catheter: an alternative access method during catheter ablation of supraventricular tachycardias after an extracardiac Fontan operation. Heart Rhythm. 2014 Aug;11 (8):1492–4. doi: 10.1016/j.hrthm.2013.10.036. [DOI] [PubMed] [Google Scholar]
- 47.Swale M, Mikell S, Gard J, Munger TM, Asirvatham SJ, Friedman PA. Epicardial access: patient selection, anatomy and a stepwise approach. J Innovations in Cardiac Rhythm Management. 2011;2:239–249. [Google Scholar]
- 48.Soejima Kyoko, Couper Gregory, Cooper Joshua M, Sapp John L, Epstein Laurence M, Stevenson William G. Subxiphoid surgical approach for epicardial catheter-based mapping and ablation in patients with prior cardiac surgery or difficult pericardial access. Circulation. 2004 Sep 07;110 (10):1197–201. doi: 10.1161/01.CIR.0000140725.42845.90. [DOI] [PubMed] [Google Scholar]
- 49.Mavroudis C, Backer C L, Deal B J, Johnsrude C L. Fontan conversion to cavopulmonary connection and arrhythmia circuit cryoblation. J. Thorac. Cardiovasc. Surg. 1998 Mar;115 (3):547–56. doi: 10.1016/s0022-5223(98)70316-2. [DOI] [PubMed] [Google Scholar]
- 50.Deal B J, Mavroudis C, Backer C L, Johnsrude C L, Rocchini A P. Impact of arrhythmia circuit cryoablation during Fontan conversion for refractory atrial tachycardia. Am. J. Cardiol. 1999 Feb 15;83 (4):563–8. doi: 10.1016/s0002-9149(98)00914-x. [DOI] [PubMed] [Google Scholar]
- 51.Mavroudis Constantine, Deal Barbara J., Backer Carl L., Johnsrude Christopher L.. The favorable impact of arrhythmia surgery on total cavopulmonary artery Fontan conversion. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 1999;2 ():143–156. doi: 10.1016/s1092-9126(99)70013-x. [DOI] [PubMed] [Google Scholar]
- 52.Mavroudis C, Backer C L, Deal B J, Johnsrude C, Strasburger J. Total cavopulmonary conversion and maze procedure for patients with failure of the Fontan operation. J. Thorac. Cardiovasc. Surg. 2001 Nov;122 (5):863–71. doi: 10.1067/mtc.2001.117840. [DOI] [PubMed] [Google Scholar]
- 53.Van Hare G F, Lesh M D, Stanger P. Radiofrequency catheter ablation of supraventricular arrhythmias in patients with congenital heart disease: results and technical considerations. J. Am. Coll. Cardiol. 1993 Sep;22 (3):883–90. doi: 10.1016/0735-1097(93)90207-h. [DOI] [PubMed] [Google Scholar]
- 54.Kanter R J, Papagiannis J, Carboni M P, Ungerleider R M, Sanders W E, Wharton J M. Radiofrequency catheter ablation of supraventricular tachycardia substrates after mustard and senning operations for d-transposition of the great arteries. J. Am. Coll. Cardiol. 2000 Feb;35 (2):428–41. doi: 10.1016/s0735-1097(99)00557-4. [DOI] [PubMed] [Google Scholar]
- 55.Mavroudis Constantine, Deal Barbara J, Backer Carl L. Arrhythmia surgery in association with complex congenital heart repairs excluding patients with fontan conversion. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2003;6 ():33–50. doi: 10.1053/pcsu.2003.50019. [DOI] [PubMed] [Google Scholar]
- 56.Theodoro D A, Danielson G K, Porter C J, Warnes C A. Right-sided maze procedure for right atrial arrhythmias in congenital heart disease. Ann. Thorac. Surg. 1998 Jan;65 (1):149–53. doi: 10.1016/s0003-4975(97)01193-4. [DOI] [PubMed] [Google Scholar]
- 57.Collins Kathryn K, Rhee Edward K, Delucca Janet M, Alexander Mark E, Bevilacqua Laura M, Berul Charles I, Walsh Edward P, Mayer John E, Jonas Richard A, del Nido Pedro J, Triedman John K. Modification to the Fontan procedure for the prophylaxis of intra-atrial reentrant tachycardia: short-term results of a prospective randomized blinded trial. J. Thorac. Cardiovasc. Surg. 2004 Mar;127 (3):721–9. doi: 10.1016/s0022-5223(03)01055-9. [DOI] [PubMed] [Google Scholar]
- 58.Jadonath R L, Snow J S, Goldner B G, Cohen T J. Radiofrequency catheter ablation as primary therapy for symptomatic ventricular tachycardia. J Invasive Cardiol. 1994 Oct 5;6 (9):289–95. [PubMed] [Google Scholar]
- 59.Khairy Paul, Landzberg Michael J, Gatzoulis Michael A, Lucron Hugues, Lambert Jean, Marçon François, Alexander Mark E, Walsh Edward P. Value of programmed ventricular stimulation after tetralogy of fallot repair: a multicenter study. Circulation. 2004 Apr 27;109 (16):1994–2000. doi: 10.1161/01.CIR.0000126495.11040.BD. [DOI] [PubMed] [Google Scholar]
- 60.Rostock Thomas, Willems Stephan, Ventura Rodolfo, Weiss Christian, Risius Tim, Meinertz Thomas. Radiofrequency catheter ablation of a macroreentrant ventricular tachycardia late after surgical repair of tetralogy of Fallot using the electroanatomic mapping (CARTO). Pacing Clin Electrophysiol. 2004 Jun;27 (6 Pt 1):801–4. doi: 10.1111/j.1540-8159.2004.00531.x. [DOI] [PubMed] [Google Scholar]
- 61.Fontan F, Baudet E. Surgical repair of tricuspid atresia. Thorax. 1971 May;26 (3):240–8. doi: 10.1136/thx.26.3.240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Björk V O, Olin C L, Bjarke B B, Thorén C A. Right atrial-right ventricular anastomosis for correction of tricuspid atresia. J. Thorac. Cardiovasc. Surg. 1979 Mar;77 (3):452–8. [PubMed] [Google Scholar]
- 63.Marcelletti C, Corno A, Giannico S, Marino B. Inferior vena cava-pulmonary artery extracardiac conduit. A new form of right heart bypass. J. Thorac. Cardiovasc. Surg. 1990 Aug;100 (2):228–32. [PubMed] [Google Scholar]