

Abstract
Background
Little attention has focused on the integration of mobile health (mHealth) technology with self-management approaches to improve the detection and management of atrial fibrillation (AF) in clinical practice.
Objective
The objective of this study was to investigate the differences between mHealth and usual care over a 6-month follow-up period among patients with a known history of atrial fibrillation.
Methods
A pilot cohort from within the larger ongoing randomized trial, iPhone® Helping Evaluate Atrial fibrillation Rhythm through Technology (iHEART), was evaluated to determine differences in detection of AF and atrial flutter (AFL) recurrence rates (following treatment to restore normal rhythm) between patients undergoing daily smartphone ECG monitoring and age and gender matched control patients. SF-36v2TM QoL assessments were administered at baseline and 6 months to a subset of the patients undergoing daily ECG monitoring. Differences between groups were assessed by t-test, Fisher’s exact test, and Cox proportional hazard models.
Results
Among the 23 patients with smartphone ECG monitors (16 males and 7 females, mean age 55 ± 10), 14 (61%) had detection of recurrent AF/AFL versus 30% of controls. During the follow-up period, patients given smartphone ECG monitors were more than twice as likely to have an episode of recurrent AF/AFL detected (hazard ratio: 2.55; 95% CI: 1.06 – 6.11; p = 0.04). Among the 13 patients with baseline and 6 month QoL assessments, significant improvements were observed in the physical functioning (p = 0.009), role physical (p = 0.007), vitality (p = 0.03), and mental health domains (p = 0.02).
Conclusions
Cardiac mHealth self-monitoring is a feasible and effective mechanism for enhancing AF/AFL detection that improves quality of life.
Keywords: MHealth, ECG, Atrial Fibrillation, QoL
Introduction
Atrial fibrillation (AF) is the most common arrhythmia encountered in clinical practice and is a global epidemic with an estimated worldwide prevalence in 2010 of 20.9 million men and 12.9 million women.[1] The condition is expected to more than double over the next 35 years,[2] which further highlights the societal burden of AF and the need for innovative ways to improve its detection, treatment, and management. Individuals affected by AF may experience a variety of symptoms ranging from palpitations and fatigue to dyspnea and chest pain.[3] Many patients are asymptomatic[3] or experience very brief episodes associated with vague symptoms such as fatigue that could be related to other co-existing conditions such as heart failure or age-related changes. The lack of consistent follow-up further highlights the challenges encountered in documenting AF. Individuals with AF that goes unrecognized and untreated are at an increased risk for stroke and overall mortality.[3] Thus, it is critical to evaluate advances in mHealth monitoring to determine how advances in technology can be utilized to improve AF detection and treatment.
The affordability of smartphones has enabled mHealth technology to be integrated rapidly into day-to-day living. For example, 2 billion people, equal to approximately 28% of the global population, currently use smartphone technology.[4] Additionally, there are over 100 million active iPhones® in the United States alone[5] (https://9to5mac.com/2015/11/19/apple-100-million-active-iphones-us/), making mHealth technology a logical avenue for widespread integration into healthcare. Since most individuals report having their cell phones with them at all times, it is feasible to consider mHealth as an effective mechanism not only to transmit real-time ECG data to a healthcare provider and receive immediate feedback, but also to improve patient engagement and self-management. The purpose of this study was to determine if an FDA approved wireless electrocardiogram (ECG) monitor designed for use with smartphones (AliveCor™ ECG) could be utilized to detect and manage recurrent AF or other atrial arrhythmias better than usual medical care (without mHealth ECG monitoring). The primary outcome of this study was the detection of recurrent AF or other atrial arrhythmias over a 6-month period of time, using the AliveCor™ ECG monitor as compared to usual cardiac care without mHealth daily monitoring.
Methods
Recruitment and the Informed Consent Process
This investigation was approved by the Columbia University Medical Center Institutional Review Board (IRB) prior to subject enrollment (IRB-AAAJ7801). Subjects were recruited for this pilot study from the departments of cardiac electrophysiology and cardiac ambulatory care at Columbia University Medical Center in New York, NY, USA. These individuals were identified as potential study subjects by their healthcare providers during routine care visits within these departments. The healthcare provider obtained verbal approvals from the patients before the study team approached them. If the participants agreed to be approached, the study team discussed the study with them, allowed them to read the informed consent, and answered all questions. If the patients agreed to participate, they were asked to sign the informed consent which was available in both English and Spanish (participant’s preference). All participants were given a copy of their signed consent form for their personal records.
Study Subjects and Sample Size
Twenty-three subjects participated in the ECG monitoring pilot study. All subjects were 21 years or older, with a documented history of AF and were scheduled to undergo a cardioversion, ablation, and/or medical management aimed at maintaining a normal sinus rhythm. Patients who successfully had normal sinus rhythm restored were given a heart monitor (AliveCor™) compatible with iPhone® or Android™ (ECG monitoring group). The control group consisted of 23 age (within 5 years) and gender matched patients with a documented history of AF receiving usual cardiac medical care (no daily ECG self-monitoring) as part of their usual clinical management. In addition, baseline and 6 month SF-36v2TM Quality of Life assessments were administered to 13 patients in the ECG monitoring group in order to evaluate perceptions of their physical and mental health. These 13 patients also filled out a questionnaire at 6 months which queried their attitudes toward ECG monitoring.
Device Training
After collecting baseline information, patients in the ECG monitoring group were provided with a heart monitoring device for compatible smartphones. The AliveCor™ ECG device attaches to a smartphone with the one-time adhesive [Figure 1]. A member of the study team downloaded the "AliveECG” application to the patient’s smartphone [Figure 1a]. Subjects were then trained on how to use the heart monitor and capture an ECG. A test ECG recording and transmission was performed during baseline enrollment to ensure the quality of the ECG data being collected and that the participant was comfortable and could independently perform the ECG capture. This training session took from 15-30 minutes, depending on the user’s familiarity with technology.
Figure 1. AliveCor™ ECG device attaches to smartphone with one-time adhesive.

Figure 1A. AliveCor Kardia application.
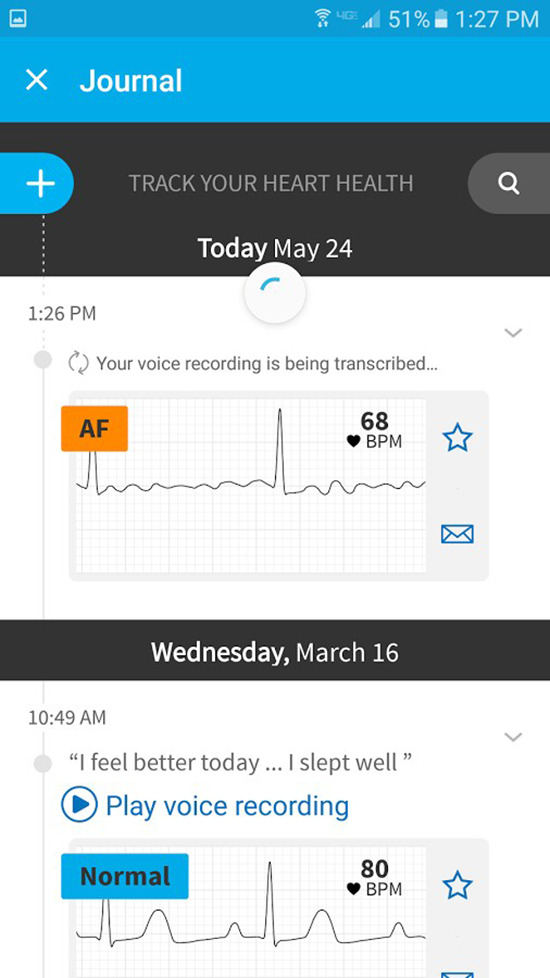
Patients in the ECG monitoring group were asked to use the wireless ECG device at least daily (and when symptomatic) to record ECG readings for a period of 6 months; transmission time took less than 5 minutes per day. All ECGs were reviewed daily for AF and other rhythm disturbances and the results were sent to the patient’s primary care physician. The patient’s physician/healthcare team performed the treatment and management of any recorded AF or other cardiac arrhythmias. No members of the research team were involved in direct clinical care.
Quality of Life
Quality of Life was assessed using the SF-36v2TM multi-item scale that measures eight health concepts (four physical and four mental health domains) rated on a 3- to 6-point Likert scale.[6] Responses to the questionnaire were transformed into norm-based physical and mental scores.The four physical domains (physical functioning, role-physical, bodily pain, general health) and four mental health domains (vitality, social functioning, role-emotional and mental health) were determined along with the physical component summary (PCS) and mental component summary (MCS) scores. These measures were scaled to have a mean of 50 and a standard deviation of 10 in the general population.
Statistical Analyses
All demographic and clinical data with the exception of age are reported as frequencies and percentages; age is reported as mean and standard deviation. Means and standard deviations were also used to characterize the SF-36v2TM domain and summary scores in the ECG monitoring group at baseline and 6 months. Fisher’s exact test were used to assess differences in clinical characteristics, medications, and AF procedures between those in the ECG monitoring group and the control group. Kaplan-Meier curves were created for AF/AFL detection rates for the ECG monitoring and control groups over the 6 month follow-up period. Differences in AF/AFL detection rates betweenof the study team downloaded groups were assessed using Cox proportional hazards models. Paired t-tests were used for testing differences in QoL health domains and summary scores between baseline and 6 months among patients in the ECG monitoring group. Analyses were performed using SAS 9.4 (SAS Institute, Cary, NC). A critical p-value of 0.05 was used for significance in all analyses.
Results
The demographic and clinical characteristics of the patients in the ECG monitoring and control groups are listed in [Table 1]. The ECG monitoring group consisted of 16 males and 7 females (mean age 55 ± 10) with control subjects matched for age and gender. Within the ECG monitoring group, 16 (70%) had been previously treated with cardioversion while 10 (43%) had undergone cardiac ablation; these rates did not differ significantly in the control group. There were no significant differences between groups with respect to the prevalence of coronary artery disease, stroke/TIA, congestive heart failure, cardiovascular risk factors, or medication usage.
Table 1. Clinical Characteristics.
* 1 response missing
| Variable | ECG Monitoring Group (N = 23) | Control Group (N=23) | P Value |
| Age (mean + SD, years) | 55 + 10 | 55 + 9 | --- |
| # (%) | # (%) | ||
| Males | 15 (71%) | 15 (71%) | --- |
| Previous Cardioversion | 16 (70%) | 13 (57%) | 0.54 |
| Cardiac Ablation | 10 (43%) | 11 (48%) | 1.0 |
| Coronary Artery Disease | 3 (13%) | 3 (13%) | 1.0 |
| Stroke/TIA | 3 (13%) | 0 (0%) | 0.23 |
| Congestive Heart Failure | 6 (26%) | 3 (13%) | 0.46 |
| CHA2DS2-VASc > 1 | 5 (22%) | 3 (13%) | 0.70 |
| Diabetes | 1 (4%) | 3 (13%) | 0.61 |
| Hypertension | 11 (48%) | 13 (57%) | 0.77 |
| Obesity | 9 (39%) | 15 (65%) | 0.14 |
| History of Smoking | 9 (39%) | 3 (13%) | 0.09 |
| Medications | |||
| Anticoagulants | 22 (96%) | 20 (87%) | 0.61 |
| Beta Blockers | 15 (68%)* | 19 (83%) | 0.31 |
| Antiarrhythmics | 10 (43%) | 11 (48%) | 1.0 |
| Diuretics | 6 (26%) | 4 (17%) | 0.72 |
| Calcium Channel Blockers | 5 (22%) | 7 (30%) | 0.74 |
| ACE/ARB | 1 (4%) | 4 (17%) | 0.35 |
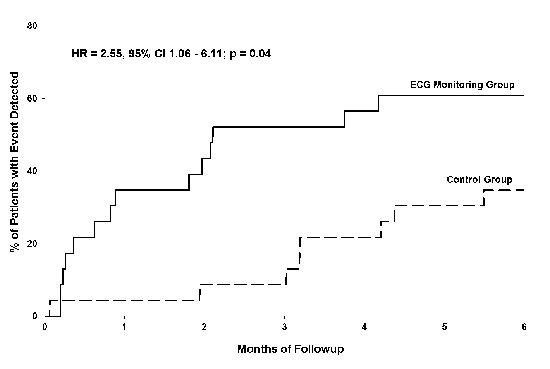
Kaplan-Meier curves depicting the AF/AFL detection rates for the ECG monitoring and control groups are shown in [Figure 2]. Over the six month follow-up period, 14 patients in the ECG monitoring group (61%) and 7 patients in the control group (30%) had episodes of AF/AFL detected. Cox proportional hazard model analysis yielded a hazard ratio of 2.55 with a 95% confidence interval of 1.06 to 6.11, p = 0.04.
Figure 2. Kaplan-Meier Curves for AF/AFI Detection.
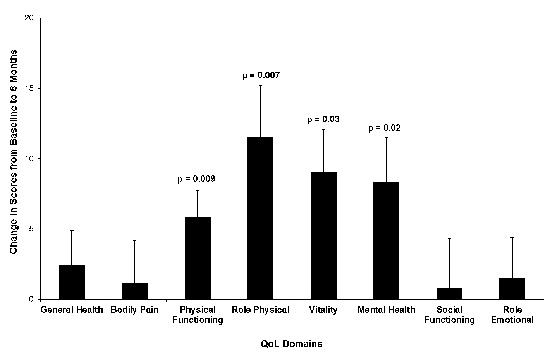
Among the 13 patients in ECG monitoring group who had QoL assessments at baseline and 6 months, PCS scores increased significantly from 50.3 ± 7.6 to 55.9 ± 5.3 (p = 0.02) while MCS scores did not change significantly from baseline to 6 months (47.5 ± 7.2 and 51.7 ± 9.6, respectively). The baseline and 6 month domain scores are listed in [Table 2]. [Figure 3] shows the change in domain scores from baseline to 6 months. Significant increases were observed for physical functioning, role physical, vitality, and mental health domain scores.
Table 2. Baseline and 6 Month SF-36 Quality of Life Domains.
| Domain | Baseline(mean + SD) | 6 Months(mean + SD) | ||||
| General Health | 52.0 + 9.0 | 54.4 + 4.1 | ||||
| Bodily Pain | 53.0 + 6.8 | 54.1 + 8.0 | ||||
| Physical Functioning | 49.9 + 7.7 | 55.7 + 2.5 | ||||
| Role Physical | 44.0 + 11.4 | 55.5 + 4.8 | ||||
| Vitality | 45.3 + 11.2 | 54.3 + 8.1 | ||||
| Mental Health | 42.6 + 7.2 | 50.9 + 8.5 | ||||
| Social Functioning | 53.1 + 6.8 | 53.9 + 7.9 | ||||
| Role Emotional | 52.2 + 6.2 | 53.7 + 7.5 | ||||
Figure 3. Change in SF-36 QoL Domain Scores.
At 6 months, none of the patients in the ECG monitoring group reported trouble using the device. In addition, 92% of respondents thought the device was beneficial and 58% said that they were more health conscious after participating in the study. Additionally, there was no difference in the rate of hospitalizations between the ECG monitoring group and the control group; no deaths occurred during follow-up.
Discussion
In this convenience sample of an ambulatory cardiac electrophysiology clinic population, use of mobile ECG technology resulted in higher rate of redetection of AF/AFL than monitoring through routine care in an age and gender-matched control group. Our study adds to the growing evidence regarding the use of smartphone-based ECG monitoring in other settings[7]-[12], including primary care and post-cardiac surgery, and is representative of the current “real world” shift in ECG monitoring and self-management in clinical practice.
Among patients in the Alivecor™ ECG group, significant increases in quality of life scores were observed between baseline and 6 months follow-up, spanning both physical and mental health domains. These differences are remarkable given the increased detection of AF/AFL that was noted with more intensive ECG monitoring. While speculative, it is possible that improvements in quality of life stem from the assurance of quicker treatment of arrhythmia episodes that would otherwise have gone undetected. Furthermore, mobile phone-based ECG monitoring offers greater access to investigate symptoms that may or may not be related to cardiac arrhythmia, which may reduce the patient’s level of uncertainty. Our participants had the ability to transmit anytime they were symptomatic from virtually anywhere and a trained healthcare provider was able to provide them immediate feedback on their rhythm status (i.e., AF/AFL, normal sinus rhythm, or some other rhythm such as frequent APCs/VPCs that may be associated with symptoms). Many subjects reported that knowing someone was vigilantly watching their heart rhythm was reassuring.
An important facet of new mHealth ECG technology is that multiple adhesive electrodes are not required as in Holter recording and event/patch-type ECG monitors, which can be cumbersome for patients to wear and reapply for extended periods of time leading to diminished ECG monitoring compliance. In addition, the time period is limited in which data is captured for a Holter or event/patch ECG device, ranging from 24 hours to 30 days, and requires the transmission and review of stored ECG data from the patient to a central monitoring site or service for validation and analysis.[13] Although Holter monitors have historically been the standard for clinical cardiac monitoring, their lower diagnostic yield, inconvenience, and higher costs have sparked a movement towards portable and user-friendly ECG devices.[14] The AliveCor™ device, for instance, captures a medical-grade ECG in 30-seconds, from virtually anywhere and has been validated and deemed effective in multiple studies.[15]-[17] An instant ECG analysis is provided using FDA-approved machine learning algorithms, which alert the patient (user) of a normal ECG reading or an indication of possible AF. Patients are also able to track their ECGs and associated symptoms using the AliveCor™ device/app and can relay this information rapidly to their doctor (via print or email as a PDF file) to inform a diagnosis/treatment plan.
Limitations of this study include the non-randomized ECG assignment and small homogenous group of subjects. We are currently conducting a larger prospective randomized study of mobile ECG technology for AF detection among 300 patients with a history of atrial fibrillation.[18] Of note, the protocol also incorporates text messaging to the mobile ECG group in order to provide education concerning risk factors associated with AF and potential alternatives for behavior modification. This messaging may result in subjects being more engaged in their self-management and reducing their AF burden. We will also examine the impact of ECG mHealth on QoL in this larger cohort.
Conclusions
Cardiac mHealth self-monitoring with the AliveCor™ ECG is a feasible and effective mechanism for improving AF/AFL detection in the real world. Individuals with AF who engaged in self-monitoring and knew their ECGs were vigilantly being reviewed reported a better self-reported QoL.
Conflict Of Interests
None.
Disclosures
This research is funded by a R01 from the National Institute of Nursing. NIH/NINR R01NR014853.
References
- 1.Barnett Adam S, Lewis William R, Field Michael E, Fonarow Gregg C, Gersh Bernard J, Page Richard L, Calkins Hugh, Steinberg Benjamin A, Peterson Eric D, Piccini Jonathan P. Quality of Evidence Underlying the American Heart Association/American College of Cardiology/Heart Rhythm Society Guidelines on the Management of Atrial Fibrillation. JAMA Cardiol. 2017 Mar 01;2 (3):319–323. doi: 10.1001/jamacardio.2016.4936. [DOI] [PubMed] [Google Scholar]
- 2.Munger Thomas M, Wu Li-Qun, Shen Win K. Atrial fibrillation. J Biomed Res. 2014 Jan;28 (1):1–17. doi: 10.7555/JBR.28.20130191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.January Craig T, Wann L Samuel, Alpert Joseph S, Calkins Hugh, Cigarroa Joaquin E, Cleveland Joseph C, Conti Jamie B, Ellinor Patrick T, Ezekowitz Michael D, Field Michael E, Murray Katherine T, Sacco Ralph L, Stevenson William G, Tchou Patrick J, Tracy Cynthia M, Yancy Clyde W. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation. 2014 Dec 02;130 (23):e199–267. doi: 10.1161/CIR.0000000000000041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Neubeck Lis, Lowres Nicole, Benjamin Emelia J, Freedman S Ben, Coorey Genevieve, Redfern Julie. The mobile revolution--using smartphone apps to prevent cardiovascular disease. Nat Rev Cardiol. 2015 Jun;12 (6):350–60. doi: 10.1038/nrcardio.2015.34. [DOI] [PubMed] [Google Scholar]
- 5.J Kahn. Report: Apple now at over 100 million iPhones in use in the US. . https://9to5mac.com/2015/11/19/apple-100-million-active-iphones-us. 0;0:0–0. [Google Scholar]
- 6.Newnham Elizabeth A, Harwood Kate E, Page Andrew C. Evaluating the clinical significance of responses by psychiatric inpatients to the mental health subscales of the SF-36. J Affect Disord. 2007 Feb;98 (1-2):91–7. doi: 10.1016/j.jad.2006.07.001. [DOI] [PubMed] [Google Scholar]
- 7.Hickey Kathleen T, Reiffel James, Sciacca Robert R, Whang William, Biviano Angelo, Baumeister Maurita, Castillo Carmen, Talathothi Jyothi, Garan Hasan. The Utility of Ambulatory Electrocardiographic Monitoring for Detecting Silent Arrhythmias and Clarifying Symptom Mechanism in an Urban Elderly Population with Heart Failure and Hypertension: Clinical Implications. J Atr Fibrillation. 2010 Jan 01;1 (12):663–674. doi: 10.4022/jafib.193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Orchard Jessica, Freedman Saul Benedict, Lowres Nicole, Peiris David, Neubeck Lis. iPhone ECG screening by practice nurses and receptionists for atrial fibrillation in general practice: the GP-SEARCH qualitative pilot study. Aust Fam Physician. 2014 May;43 (5):315–9. [PubMed] [Google Scholar]
- 9.Orchard Jessica, Lowres Nicole, Freedman S Ben, Ladak Laila, Lee William, Zwar Nicholas, Peiris David, Kamaladasa Yasith, Li Jialin, Neubeck Lis. Screening for atrial fibrillation during influenza vaccinations by primary care nurses using a smartphone electrocardiograph (iECG): A feasibility study. Eur J Prev Cardiol. 2016 Oct;23 (2 suppl):13–20. doi: 10.1177/2047487316670255. [DOI] [PubMed] [Google Scholar]
- 10.Lowres Nicole, Mulcahy Georgina, Gallagher Robyn, Ben Freedman Saul, Marshman David, Kirkness Ann, Orchard Jessica, Neubeck Lis. Self-monitoring for atrial fibrillation recurrence in the discharge period post-cardiac surgery using an iPhone electrocardiogram. Eur J Cardiothorac Surg. 2016 Jul;50 (1):44–51. doi: 10.1093/ejcts/ezv486. [DOI] [PubMed] [Google Scholar]
- 11.Haberman Zachary C, Jahn Ryan T, Bose Rupan, Tun Han, Shinbane Jerold S, Doshi Rahul N, Chang Philip M, Saxon Leslie A. Wireless Smartphone ECG Enables Large-Scale Screening in Diverse Populations. J. Cardiovasc. Electrophysiol. 2015 May;26 (5):520–6. doi: 10.1111/jce.12634. [DOI] [PubMed] [Google Scholar]
- 12.Tarakji Khaldoun G, Wazni Oussama M, Callahan Thomas, Kanj Mohamed, Hakim Ali H, Wolski Kathy, Wilkoff Bruce L, Saliba Walid, Lindsay Bruce D. Using a novel wireless system for monitoring patients after the atrial fibrillation ablation procedure: the iTransmit study. Heart Rhythm. 2015 Mar;12 (3):554–9. doi: 10.1016/j.hrthm.2014.11.015. [DOI] [PubMed] [Google Scholar]
- 13.Mittal Suneet, Movsowitz Colin, Steinberg Jonathan S. Ambulatory external electrocardiographic monitoring: focus on atrial fibrillation. J. Am. Coll. Cardiol. 2011 Oct 18;58 (17):1741–9. doi: 10.1016/j.jacc.2011.07.026. [DOI] [PubMed] [Google Scholar]
- 14.Lobodzinski S Suave. ECG patch monitors for assessment of cardiac rhythm abnormalities. Prog Cardiovasc Dis. 2013 Nov 13;56 (2):224–9. doi: 10.1016/j.pcad.2013.08.006. [DOI] [PubMed] [Google Scholar]
- 15.Olgun Kucuk Hilal, Kucuk Ugur, Yalcin Murat, Isilak Zafer. Time to use mobile health devices to diagnose paroxysmal atrial fibrillation. Int. J. Cardiol. 2016 Nov 01;222 () doi: 10.1016/j.ijcard.2015.10.159. [DOI] [PubMed] [Google Scholar]
- 16.Baquero Giselle A, Banchs Javier E, Ahmed Shameer, Naccarelli Gerald V, Luck Jerry C. Surface 12 lead electrocardiogram recordings using smart phone technology. J Electrocardiol. 2014 Oct 7;48 (1):1–7. doi: 10.1016/j.jelectrocard.2014.09.006. [DOI] [PubMed] [Google Scholar]
- 17.Chung Eugene H, Guise Kimberly D. QTC intervals can be assessed with the AliveCor heart monitor in patients on dofetilide for atrial fibrillation. J Electrocardiol. 2014 Dec 3;48 (1):8–9. doi: 10.1016/j.jelectrocard.2014.10.005. [DOI] [PubMed] [Google Scholar]
- 18.Hickey Kathleen T, Hauser Nicole R, Valente Laura E, Riga Teresa C, Frulla Ashton P, Masterson Creber Ruth, Whang William, Garan Hasan, Jia Haomiao, Sciacca Robert R, Wang Daniel Y. A single-center randomized, controlled trial investigating the efficacy of a mHealth ECG technology intervention to improve the detection of atrial fibrillation: the iHEART study protocol. BMC Cardiovasc Disord. 2016 Jul 16;16 () doi: 10.1186/s12872-016-0327-y. [DOI] [PMC free article] [PubMed] [Google Scholar]