

Abstract
Erectile dysfunction significantly affects quality of life in young men. Authors have evaluated erectile function in men with coronary artery disease (CAD) and the relationship between the degree of erectile dysfunction (ED) and the age of their first acute myocardial infarction (AMI). The incidence of erectile dysfunction in three groups of patients of AMI survivors was investigated: AMI survivors younger than 45 years, AMI survivors older than 65 years, and normal male population aged between 30 and 60 years. Erectile function was assessed by the International Index of Erectile Function (IIEF-5) questionnaire. In post-AMI male patients younger than 45 years (n = 76), mild ED occurred in 26% and severe in 7%. In the older AMI group, mild ED occurred in 52% and severe in 38%. In the control group age matched to younger survivors, 96% denied ED and only one control patient had a score of 20 on the IIEF-5. A paradoxical result was observed in patients using beta blockers (BB), who had better scores than the group without BB. Statin treatment had a positive influence on the score in questionnaires. Those on statins had an average score of 21.0 ± 4.9 vs. without statin 17.7 ± 5.7, p = .03. The current findings identified that the prevalence of ED is relatively high in young patients with CAD and is related to treatment of the CAD. The overall increase in ED presence suggests that the background of their coronary event is not due to destabilization of single focused atheroma but may reflect a generalized atherosclerotic process.
Keywords: erectile dysfunction, atherosclerosis, ischaemic heart disease, acute myocardial infarction
Erectile dysfunction (ED) is defined by the NIH Consensus Development Panel on Impotence (published in JAMA 1993 “NIH Consensus Conference. Impotence. NIH Consensus Development Panel on Impotence” 1993) as “the persistent inability to achieve and maintain an erection sufficient to permit satisfactory sexual intercourse.” The prevalence of ED depends on the studied population. In some studies, the abridged 5-item version of the International Index of Erectile Function (IIEF-5) (Rhoden, Teloken, Sogari, & Vargas Souto, 2002; Rosen, Cappelleri, Smith, Lipsky, & Pena, 1999) was used as a diagnostic tool. The IIEF addresses the relevant domains of male sexual function (i.e., erectile function, orgasmic function, sexual desire, intercourse satisfaction, and overall satisfaction); the questionnaire is self-administered in clinical settings (Rosen et al., 1999).
ED is often associated with chronic illnesses, such as arterial hypertension, diabetes mellitus, and coronary artery disease (CAD) (Montorsi et al., 2003). In a cohort of patients with CAD, ED rate differs according to coronary presentation and its severity is related to the extent of CAD (Montorsi et al., 2003).
Several studies reported an association between ED and CAD (Gandaglia et al., 2014; Otunctemur et al., 2015; Omland, Randby, Hrubos-Strom, Rosjo, & Einvik, 2016). According to some authors, ED and CAD should be regarded as “two different manifestations of the same systemic disorder.” ED usually precedes a CAD onset, and it might be considered an early marker of symptomatic CAD (Gandaglia et al., 2014). An association between treatment for erectile dysfunction and death of cardiovascular outcomes after myocardial infarction in a Swedish nationwide cohort study (in men younger than 80 years of age) was described by Andersson et al. (2017). Conversely, ED in post-AMI male patients younger than 45 years has not been precisely described.
Methods
Since 2010, male survivors of AMI in whom AMI occurred before the age of 45 (n = 78) and after the age of 65 (n = 21) were investigated and compared to healthy subjects aged between 30 and 60 years (n = 27). All patients participated on a voluntary basis and were invited to the study by an invitation letter or were directly asked to participate during their medical follow-up in the cardiovascular center. Five patients in our young patient population reported ED prior to having their AMI. All patients had a history of documented AMI according to the 2012 definition of the European Society of Cardiology (Thygesen et al., 2012). Most of the patients had either a history of coronary intervention for their AMI or a coronary lesion confirmed by coronary angiography. For ascertainment of the coronary disease extent, a significant arterial lesion was defined by a presence of at least one ≥50% stenosis downstream the major coronary artery.
The time span between AMI and the current clinical study examination was required to be <5 years. All participating subjects underwent a complex clinical examination—clinical history of risk factors was taken and patients underwent clinical and laboratory investigations. All subjects were invited to complete a sexual activity questionnaire (IIEF-5).
The study’s protocol conformed to all ethical guidelines of the 1975 Declaration of Helsinki and was approved by the respective institution’s Ethics Committee. All subjects participating in the study provided written informed consent, as was published earlier (Linhart et al., 2012).
As the diagnostic tool for ED, the International Index of Erectile Function (IIEF-5) questionnaire (Table 1) was used, originally published in Rosen et al. (1999).
Table 1.
The International Index of Erectile Function (IIEF-5) Questionnaire(http://www.hiv.va.gov/provider/manual-primary-care/urology-tool2.asp, originally published in Rosenet al. (1999).
| Over the past 6 months | |||||
|---|---|---|---|---|---|
| 1. How do you rate your confidence that you could get and keep an erection? | Very low 1 | Low 2 | Moderate 3 | High 4 | Very high 5 |
| 2. When you had erections with sexual stimulation, how often were your erections hard enough for penetration? | Almost never/never 1 | A few times (much less than half the time) 2 | Sometimes (about half the time) 3 | Most times (much more than half the time) 4 | Almost always/always 5 |
| 3. During sexual intercourse, how often were you able to maintain your erection after you had penetrated (entered) your partner? | Almost never/never 1 | A few times (much less than half the time) 2 | Sometimes (about half the time) 3 | Most times (much more than half the time)4 | Almost always/always 5 |
| 4. During sexual intercourse, how difficult was it to maintain your erection to completion of intercourse? | Extremely difficult 1 | Very difficult 2 | Difficult 3 | Slightly difficult 4 | Not difficult 5 |
| 5. When you attempted sexual intercourse, how often was it satisfactory for you? | Almost never/never 1 | A few times (much less than half the time) 2 | Sometimes (about half the time) 3 | Most times (much more than half the time) 4 | Almost always/always 5 |
IIEF-5 scoring:
The IIEF-5 score is the sum of the ordinal responses to the five items.
22–25: No erectile dysfunction.
17–21: Mild erectile dysfunction.
12–16: Mild to moderate erectile dysfunction.
8–11: Moderate erectile dysfunction.
5–7: Severe erectile dysfunction.
Statistical Analysis
Data were analyzed using the SAS JMP 6.0.3 statistical package. Results were expressed as mean ± standard deviations (SD) or as a percentage of subjects. Differences between the groups were assessed using ANOVA and unpaired t-tests for continuous variables with normal distribution or using the U-test analysis for variables with nonparametric distribution. χ2 test was applied for dichotomous variables. Statistical significance was defined as p < .05.
Results
Only patients with nonfatal AMI were included in the cohort of patients. All patients were interviewed by a cardiologist and a clinical examination was carried out, inclusive of echocardiography, carotid-intima measurement (as published earlier by Linhart et al., 2012), and questionnaires were filled out.
Almost all (97%, n = 76) of the younger patients and all (100%, n = 21) of patients from the older group denied being asked about ED in previous follow-up visits. The clinical and demographic characteristics of the patients are reported in Table 2.
Table 2.
The Clinical and Demographic Characteristic of the Patients.
| AMI young N = 78 |
AMI older N = 21 |
Controls N = 27 |
|
|---|---|---|---|
| Age (years) | 41 ± 8 | 72 ± 7 | 39 ± 9 |
| Height (cm) | 176 ± 19 | 175 ± 10 | 180 ± 7 |
| Weight (kg) | 90 ± 16 | 82 ± 16 | 82 ± 13 |
| BMI (kg/m2) | 28.7 ± 4.5 | 28.9 ± 3.7 | 25.0 ± 3.1 |
| Waist/hip ratio | 0.96 ± 0.97 | 0.98 ± 0.71 | 0.90 ± 0.07 |
| Systolic BP (mmHg) | 129 ± 17 | 133 ± 14 | 123 ± 15 |
| Diastolic BP (mmHg) | 79 ± 9 | 77 ± 10 | 75 ± 10 |
| Heart rate (min-1) | 68 ± 13 | 60 ± 8 | 66 ± 10 |
Smoking history was positive in 89% of young AMI survivors, 18% of them were ex-smokers. Dyslipidemia was diagnosed in 34%, arterial hypertension in 15%, and diabetes mellitus type 2 in 4% of the younger AMI patients.
Echocardiography examination results were within normal values in the control group. The cohort of younger AMI survivors had ejection fraction of the left ventricle (EF LV) during their acute hospitalization 57 ± 11%, 20 of them had EF LV under 45%, the lowest EF in this group of patients was 30%. During the study follow-up, the average EF LV was 61 ± 9%, and only 10% of patients had LV LF under 45%. The right ventricle function according to the TAPSE (tricuspid annular plane systolic excursion) parameter was predominantly within normal ranges −23.4 ± 3.1 mm, only 10% of patients had TAPSE under 20 mm (the lowest value was 17 mm). There were no patients with severe right ventricle dysfunction in the cohort. Left ventricle diastolic function was normal in 50% of the younger patients, impaired early left ventricle relaxation occurred in 38%, and 6% were detected to have pseudonormalization. In 6% (n = 5) of the patients, it was not possible to assess diastolic function. There were only two patients with mitral valve regurgitation worse than 2nd degree (1 small - 4 severe regurgitation).
During follow-up examination, 30% (n = 23) of patients complained of some dyspnoea during exercise (NYHA II), 6% (n = 5) of them were NYHA III. They were limited in daily living by shortness of breath. Sixty-four percent (n = 50) of patients did not suffer from shortness of breath, dyspnoea.
Only two patients among the young survivors of AMI did not fill out the questionnaires (one of them rejected because of his faith, one declared sexual abstinence). In total, 76 from the younger patients, 21 from the patients above 65 years of age, and all the healthy subjects (27) returned the completed questionnaires. There were no males with history of trauma to the pelvis or spinal cord, history of colorectal surgery, prostatectomy or orchidectomy, urinary incontinence, or severe depression, etc.
Results of each group of responders are reported in Tables 3 and 4. Table 3 is divided according to the scores of each question (questions 1–5), the lower the score, the higher is the prevalence of ED.
Table 3.
The International Index of Erectile Function (IIEF-5) Questionnaire and Its Average Scoring According to the Questions 1–5.
| Group of patients | N (number of patients) | Question 1 | Question 2 | Question 3 | Question 4 | Question 5 |
|---|---|---|---|---|---|---|
| Younger AIM | 76 | 3.58 | 4.23 | 4.29 | 4.12 | 4.17 |
| Older AIM | 21 | 2.21 | 2.31 | 2.63 | 2.47 | 3.15 |
| Healthy subjects | 27 | 4.42 | 4.8 | 4.96 | 4.53 | 4.76 |
Note. Results are reported as average scores; minimum 1, maximum 5 points in each question.
Table 4.
Prevalence of Mild and Severe ED in Different Cohorts.
| The IIEF-5 Score* | Young AIM | Older AIM | Healthy subjects |
|---|---|---|---|
| Score > 20 | 51 (67%) | 2 (10%) | 26 (96%) |
| Score 10-20 | 20 (26%) | 11 (52%) | 1 (4%) |
| Score < 10 | 5 (7%) | 8 (38%) | 0 (0%) |
Note. *The sum of the ordinal responses to the five items.
Table 5.
Prevalence of Mild and Severe ED in the Group of Patients Younger Than 45 Years Old, in Relation to the Number of Stenotic Coronary Arteries shows Table 5.
| The IIEF-5 Score* | 1 artery (single vessel disease) | 2 arteries | 3 arteries (multivessel disease) |
|---|---|---|---|
| Score >20 | 37 | 8 | 6 |
| Score 10–20 | 15 | 4 | 1 |
| Score <10 | 2 | 2 | 1 |
Note. *The sum of the ordinal responses to the five items. Data reported number of patients with single vessel disease; 2 = vessel disease or multivessel disease divided according to their IIEF-5 scores.
There are three groups of responders in Table 4 divided according to their scores in the IIEF-5 questionnaire. There is no erectile dysfunction in the groups with the score above 20. In young myocardial survivors, one third of patients (33%) complained of erectile dysfunction, 26% of mild, and 7% of severe. In the control group age matched to young AMI patients, 96% were without any ED, only one control subject scored with mild ED. In the group of patients above 65 years of age 90% complained of some type of ED, 38% of them with a severe grade of ED. Only 10% of patients above 65 years of age were free of ED.
Graph 1.
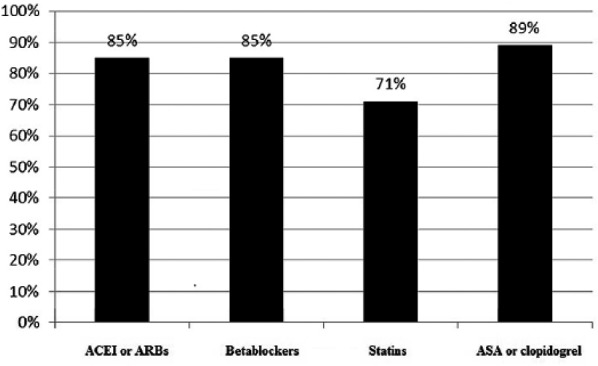
The concomitant medication in the group of young patients/like statins, beta blockers, ACEi/ARBs and antiplatelet therapy.
Symptoms of ED appeared, according to patient history, prior to AMI in five cases (6–24 months before AMI, median 12 months), the rest of the AMI group under 45 years of age denied ED. Except for four patients, ED began for all of them at the same time they suffered AMI and the treatment started. Four patients had no ED at the time of acute coronary syndrome and felt healthy at least 6 months after AMI. ED started after 6 to 12 months.
The concomitant medication such as statins, beta blockers, ACEi/ARBs, and antiplatelet therapy is reported in Graph 1. The compliance to the prescribed medication was high, more than 71% of young AMI survivors used statins, 85% of them were on ACE inhibitors or betablockers. Almost 90% of the younger group of AMI patients used clopidogrel or acetylic acid (48% of them were on dual antiplatelet therapy, three patients were on anticoagulant therapy). There were three patients without any medication, the treatment was stopped by themselves.
In the group of patients under 45 years of age, there was no influence of blood pressure values or LDL-cholesterol level or poly pharmacy (more than three different drugs in chronic medication) on the ED score. There was a beneficial effect on the score seen in the group of patients using statins. Patients treated with statins had a score of 21.0 ± 4.9 vs. 17.7 ± 5.7 in those not treated with statins, p = .03.
The patients on beta blockers (BB) reported surprisingly less ED than the group without BB (scoring on BB 20.9 ± 4.9 vs. 18.8 ± 6.0 without BB, p = .09).
Discussion
There are some limitations of the current study. The data do not represent a randomly selected population. The cohort of young AMI patients originated from survivors responding to investigators letters or phone calls, who were treated in the cardiology department in previous years. A sexual activity questionnaire was privately administered and completed during the interview at the office. It is therefore possible that these data might not represent health or disease levels of all young AMI survivors. Patients seeking medical help and responding positively to investigators calls or letters might be different from the whole population.
Important data arising from this research are that erectile dysfunction is not screened on a regular basis at cardiology departments in such a high-risk population. Patients with positive screening for ED were screened for the first time during the current study. In the younger cohort of AMI patients, only 2 out of 25 patients informed their cardiologists or GPs about their ED, and nobody diagnosed the older patients with ED.
Second, ED is a condition which is, according to reported data, highly prevalent in the group of young AMI survivors. The IIEF-5 questionnaire seems to be a very useful diagnostic tool in cardiology practice in order to not neglect such an important symptom.
There was no direct correlation between ED and type of coronary artery disease. Patients with single vessel disease do suffer from ED as well as those with multiple coronary disease as reported with the current study and by past authors (Borgquist, Gudmundsson, Winter, Nilsson, & Willenheimer, 2006; Byrne et al., 2016; Foroutan & Rajabi, 2007; Nascimento et al., 2013). The influence of beta blockers is controversial. Patients on BB reported surprisingly less ED than the group without BB. This could be biased by the previous withdrawing of BB in the latest group of patients just for their adverse influence on ED.
There was a beneficial effect on the score seen in the group of patients using statins. It could indirectly demonstrate that improvement of endothelial function could ameliorate erectile dysfunction.
Conclusions
In conclusion, the prevalence of ED was relatively high in young survivors of AMI. In these patients, the IEEF-5 questionnaire seems to be a very useful diagnostic tool in cardiology practice in order to avoid neglecting this important symptom. Furthermore, treatment of CAD can affect symptoms of ED in both positive and negative ways. Of note, ED can precede AMI on average by 12 months.
Footnotes
Author Contributions: All coauthors have read the final manuscript within their respective areas of expertise and participated in the study sufficiently to take responsibility for it and accept its conclusions.
Ethics: All procedures were in accord with the ethical standards of the regional ethics committee.
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Progres Q38/LF1.
References
- Andersson D. P., Trolle Lagerros Y., Grotta A., Bellocco R., Lehtihet M., Holzmann M. J. (2017). Association between treatment for erectile dysfunction and death or cardiovascular outcomes after myocardial infarction. Heart. doi: 10.1136/heartjnl-2016-310746 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Borgquist R., Gudmundsson P., Winter R., Nilsson P., Willenheimer R. (2006). Erectile dysfunction in healthy subjects predicts reduced coronary flow velocity reserve. International Journal of Cardiology, 112(2), 166–170. doi: 10.1016/j.ijcard.2005.08.035 [DOI] [PubMed] [Google Scholar]
- Byrne M., Doherty S., Fridlund B. G., Martensson J., Steinke E. E., Jaarsma T., Devane D. (2016). Sexual counselling for sexual problems in patients with cardiovascular disease. The Cochrane Database of Systematic Reviews, (2), CD010988. doi: 10.1002/14651858.CD010988.pub2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Foroutan S. K., Rajabi M. (2007). Erectile dysfunction in men with angiographically documented coronary artery disease. Urology Journal, 4(1), 28–32. [PubMed] [Google Scholar]
- Gandaglia G., Briganti A., Jackson G., Kloner R. A., Montorsi F., Montorsi P., Vlachopoulos C. (2014). A systematic review of the association between erectile dysfunction and cardiovascular disease. European Urology, 65(5), 968–978. doi: 10.1016/j.eururo.2013.08.023 [DOI] [PubMed] [Google Scholar]
- Linhart A., Dostalova G., Belohlavek J., Vitek L., Karetova D., Ingrischova M., . . .Cifkova R. (2012). Carotid intima-media thickness in young survivors of acute myocardial infarction. Experimental and Clinical Cardiology, 17(4), 215–220. [PMC free article] [PubMed] [Google Scholar]
- Montorsi F., Briganti A., Salonia A., Rigatti P., Margonato A., Macchi A., . . .Montorsi P. (2003). Erectile dysfunction prevalence, time of onset and association with risk factors in 300 consecutive patients with acute chest pain and angiographically documented coronary artery disease. European Urology, 44(3), 360– 364; discussion 364–365. [DOI] [PubMed] [Google Scholar]
- Nascimento E. R., Maia A. C., Pereira V., Soares-Filho G., Nardi A. E., Silva A. C. (2013). Sexual dysfunction and cardiovascular diseases: A systematic review of prevalence. Clinics (Sao Paulo), 68(11), 1462–1468. doi: 10.6061/clinics/2013(11)13 [DOI] [PMC free article] [PubMed] [Google Scholar]
- NIH Consensus Conference. NIH Consensus Development Panel on Impotence. (1993). Impotence. The Journal of the American Medical Association, 270(1), 83–90. [PubMed] [Google Scholar]
- Omland T., Randby A., Hrubos-Strom H., Rosjo H., Einvik G. (2016). Relation of erectile dysfunction to subclinical myocardial injury. The American Journal of Cardiology, 118(12), 1821–1825. doi: 10.1016/j.amjcard.2016.08.070 [DOI] [PubMed] [Google Scholar]
- Otunctemur A., Sahin S., Ozbek E., Cekmen M., Inal A., Tulubas F., . . .Koklu I. (2015). Lipoprotein-associated phospholipase A2 levels are associated with erectile dysfunction in patients without known coronary artery disease. Andrologia, 47(6), 706–710. doi: 10.1111/and.12322 [DOI] [PubMed] [Google Scholar]
- Rhoden E. L., Teloken C., Sogari P. R., Vargas Souto C. A. (2002). The use of the simplified International Index of Erectile Function (IIEF-5) as a diagnostic tool to study the prevalence of erectile dysfunction. International Journal of Impotence Research, 14(4), 245–250. doi: 10.1038/sj.ijir.3900859 [DOI] [PubMed] [Google Scholar]
- Rosen R. C., Cappelleri J. C., Smith M. D., Lipsky J., Pena B. M. (1999). Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction. International Journal of Impotence Research, 11(6), 319–326. [DOI] [PubMed] [Google Scholar]
- Thygesen K., Alpert J., Jaffe A., Simoons ML., Mendis S. (2012) Third Universal Definition o Myocardial Infarction Circulation. 2012;126:2020-2035 [DOI] [PubMed] [Google Scholar]