

Abstract
Objectives
This study aimed to assess the effect of surface treatment by bur and laser and application of universal adhesive on repair bond strength of composite resin.
Materials and Methods
A total of 120 composite blocks measuring 6×4×4 mm were fabricated of Filtek Z250 composite. All samples were subjected to 5,000 thermal cycles and divided into two groups for surface preparation by bur and by Er,Cr:YSGG laser (n = 60). The surfaces were then etched with orthophosphoric acid, rinsed with water and divided into three groups (silane, silane plus Single Bond and silane plus Single Bond Universal). Repair composite was then bonded to aged composite. Half of the samples in each group were stored in distilled water at 37°C for 24 hours and the other half underwent 5000 thermal cycles. All samples were then subjected to shear bond strength testing using a universal testing machine at a crosshead speed of 1 mm/minute. The data were analyzed using one-way ANOVA and Tukey's HSD test. Mode of failure was determined using a stereomicroscope.
Results
Bur preparation plus universal adhesive yielded the highest bond strength (30.16 µ 2.26 MPa). Laser plus silane yielded the lowest bond strength (5.63 µ 2.43 MPa). Bur preparation yielded significantly higher bond strength than laser (P < 0.001). Also, application of universal adhesive significantly improved bond strength compared to conventional adhesive and silane (P < 0.001). Bond strength after aging (5000 thermal cycles) had no significant difference with primary bond strength at 24 hours within each group (P = 0.182).
Conclusion
Surface preparation of aged composite by bur and application of universal adhesive can improve the repair bond strength of composite. Application of silane (without adhesive) in the process of repair cannot provide adequately high repair bond strength.
Keywords: Universal adhesive; Composite; Surface treatment; Er,Cr,YSGG Laser; Bur, Silane
Introduction
Composite resins are extensively used in operative dentistry due to high esthetics and conservative tooth preparation 1). Use of composite resins in dentistry has significantly increased due to advances in bonding and curing systems and physical and chemical modifications in their formulations. However, failure of composite restorations still occurs 2). In the past, complete replacement of restoration was the standard approach for eliminating small defects in restorations 3). However, complete removal of restoration weakens the tooth structure, results in unnecessary removal of tooth structure and irreversible injury to dental pulp in some cases. When secondary caries or discoloration does not exist at the tooth-restoration interface, repair is suggested instead of complete replacement of composite restoration because repair is a conservative approach that prevents unnecessary loss of tooth structure and possible injury to dental pulp 4). However, in the process of repair, it is difficult to obtain a suitable bond between the old and the new composite. When composite resin is polymerized in contact with air, a non-polymerized layer known as oxygen-inhibited layer forms on its outer surface. Due to having unreacted monomers, this layer enables adhesion between composite increments applied in the same session. Thus, bond strength in incremental build up of composite is similar to cohesive strength of composite material 5). However, as the composite restoration ages, oxygen-inhibited layer and free radicals on the surface are lost and water absorption occurs, which makes it difficult for the new composite to adequately bond to the old composite. Some measures need to be taken to enhance this bond. Thus, a combination of mechanical and chemical methods is often used to enhance the bond of new composite to aged composite 8). Mechanical preparation of composite surface is performed aiming to eliminate the superficial layer, provide a clean surface with high surface energy and increase the surface area for a suitable bond by creating porosities on the surface 9). In most clinical situations, removal of some parts of the old composite is the first step in the repair process, which is performed by bur 10). Use of laser has been recently suggested for creation of surface roughness and erbium lasers are often used for this purpose. Erbium laser irradiation is a method of surface preparation by ablation mechanism, which can be used in the process of repair 11). The next step after mechanical surface preparation is silanization and application of bonding gents in the process of repair to enhance a chemical bond 8, 12). Universal adhesives were recently introduced to enhance bond of tooth structure to ceramics, resins and metals 13). However, sufficient information is not available on the efficacy of universal adhesives in the process of composite repair. Also, studies on preparation of aged composite for a better bond are controversial. Considering the recent introduction of laser technique for surface preparation and universal adhesives, this study aimed to assess the effect of different surface preparation methods for old composite to obtain a suitable bond to new composite. The second objective was to assess the long-term stability of bond in addition to evaluating the initial repair bond strength.
Materials and Methods
Preparation of composite blocks
A total of 120 blocks of Z250 composite (A3 shade; 3M ESPE, St. Paul, MN, USA) measuring 4×4 mm with 6 mm height were fabricated using a plastic mold. The mold was fixed on a glass slab and composite was applied by a composite instrument to the mold as bulk. The composite block was then light cured from all directions for 40 seconds using a light curing unit (VALO; Ultradent Products, Inc., South Jordan, UT, USA) with a light intensity of 1000 mW/cm2 at 3 mm distance. After setting, composites were gently removed from the mold and thermocycled for 5000 cycles between 5–55°C with a dwell time of 20 seconds. After thermocycling, the samples were randomly divided into two groups (n = 60) for mechanical preparation.
Surface treatment
1. Surface preparation by bur:
One surface of each sample was roughened by diamond bur (835/008-teeskava, Iran) using a high speed handpiece under water and air spray. A new bur was used for preparation of every five composite blocks.
2. Surface treatment by laser:
One surface of each sample was irradiated by Er;Cr:YSGG laser (Waterlase, Biolase Technology, Sanclemente, CA, USA) which emits at 2780 nm. The parameters used were: 3W output power in pulsed mode, pulse duration 60 µsec, 20 Hz frequency. Laser was used with gentle sweeping motion at a working distance of 1 mm with a spot size of 800 µm (MZ-8 Ziptip, Biolase) and under air/water spray. The Fluence was 59.68 J/cm2 Next, the samples were etched with 37% phosphoric acid (Etch Royal, Pulpdent, Watertown, USA) for 15 seconds, rinsed for 10 seconds and air dried with air spray. Each group was divided into three subgroups (n = 20) for bonding procedure:
-
1.
Silane: The surface of samples in subgroup 1 (n = 20) was silanized (angelus, AMERGO Europe, Netherlands) for 10 seconds using a microbrush and dried for one minute with air spray.
-
2.
Silane plus Single Bond adhesive: Surface of samples in subgroup 2 (n = 20) was silanized for 10 seconds and dried with gentile air spray. One layer of Adper Single Bond II adhesive (3M ESPE, St. Paul, MN, USA) was rubbed on the surface for 10 seconds and cured for 20 seconds.
-
3.
Silane plus Single Bond Universal adhesive: Surface of all samples in subgroup 3 (n = 20) was silanized for 10 seconds, dried with air spray and one layer of Single Bond Universal adhesive (3M ESPE, St. Paul, MN, USA) was rubbed on the surface for 20 seconds, gently air dried for 5 seconds and cured for 10 seconds.
Repair procedure
To prepare the repair composite, a plastic cylindrical mold with 3 mm height and diameter was used. Repair composite, which was the same as the base composite (Filtek Z250; 3M ESPE, St. Paul, MN, USA) was applied to the mold and the mold was placed on prepared surfaces of samples and light-cured for 40 seconds. The mold was then removed. All samples were stored in distilled water for 24 hours. Half of the samples in each group were mounted in the metal mold of universal testing machine using acrylic resin and the other half were subjected to 5000 thermal cycles similar to initial aging protocol and were then mounted in acrylic resin.
Shear bond strength testing
Each mounted sample was fixed in universal testing machine (Zwick Roell, Ulm, Germany) such that the blade was at the interface and parallel to the longitudinal axis of samples. Load was applied to the interface at a crosshead speed of 1 mm/minute until failure. Data were then converted to megapascals (MPa) and analyzed using one-way ANOVA and Tukey's test.
Analysis of mode of failure
After shear bond strength testing, a blind observer evaluated the samples under a stereomicroscope (Nikon, Tokyo, Japan) at ×40 magnification to determine the mode of failure as:
-
1.
Adhesive: Failure at the interface
-
2.
Cohesive: Fracture of base or repair composite
-
3.
Mixed or combined failure
Results
Table 1 shows the shear bond strength in all groups. According to one-way ANOVA, the double and triple interaction effects among study variables were not significant (P > 0.066) and aging had no effect on shear bond strength (P = 0.182); but surface preparation by bur and laser had a significant effect on bond strength (P < 0.001). Also, chemical preparation (silanization, Single Bond, Single Bond Universal) had a significant effect on bond strength (P < 0.001). Pairwise comparison of groups by Tukey's HSD test revealed significant differences such that groups with Single Bond Universal adhesive had significantly higher bond strength than groups with Single Bond adhesive. Groups with Single Bond adhesive yielded significantly higher shear bond strength than silane groups (Fig. 1).
Table 1: The shear bond strength in all groups.
| preparation | Group No. | Minimum | Maximum | Mean | Std. Deviation | ||
|---|---|---|---|---|---|---|---|
| Bur | SB | immediate | G1 | 17.50 | 26.14 | 22.027 | 2.859 |
| aged | G2 | 14.73 | 29.60 | 20.547 | 4.140 | ||
| SBU | immediate | G3 | 27.14 | 34.00 | 30.162 | 2.263 | |
| aged | G4 | 21.96 | 34.66 | 28.298 | 4.355 | ||
| Silane | immediate | G5 | 8.11 | 19.87 | 14.335 | 3.698 | |
| aged | G6 | 11.46 | 18.91 | 13.852 | 2.502 | ||
| Laser | SB | immediate | G7 | 11.44 | 20.28 | 16.619 | 2.487 |
| aged | G8 | 13.52 | 19.27 | 16.059 | 2.139 | ||
| SBU | immediate | G9 | 19.15 | 29.79 | 23.976 | 4.216 | |
| aged | G10 | 19.58 | 31.31 | 24.612 | 3.510 | ||
| Silane | immediate | G11 | 2.26 | 9.02 | 5.635 | 2.437 | |
| aged | G12 | 2.96 | 7.96 | 4.750 | 1.730 |
Fig. 1:
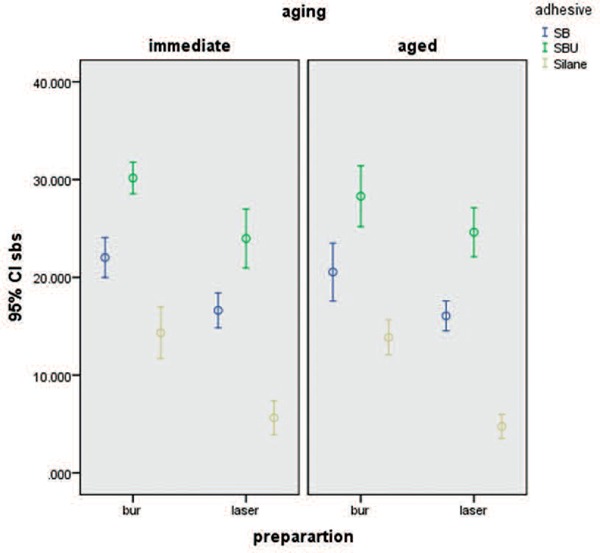
Error bar graph of mean repair bond strength values in the study groups
As seen in Fig. 1. Significant differences were noted between bur and laser groups in bond strength with 95% confidence interval.
Fig. 2 shows the frequency of modes of failure in the study groups.
Fig. 2:
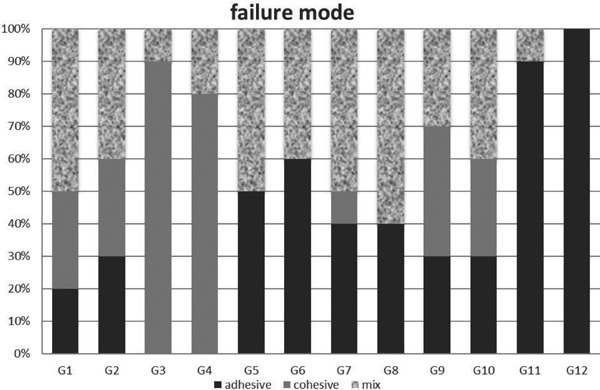
Frequency of modes of failure in the study groups
Discussion
Following aging, composites undergo structural changes due to water absorption, chemical degradation and leaching of some components as well as decreased activity of free radicals. This decreases the success rate of composite repair 1, 14, 15). Brosh et al. 16) stated that the bond between new and aged composite is achieved via three routes: Chemical bond with organic matrix, chemical bond with exposed filler particles and micromechanical bond via mechanical surface preparation. Routine method for repair of composite restorations is via the use of diamond bur and removal of part of old composite followed by the use of phosphoric acid and adhesive 17, 18). In fact, the outermost composite layer, which has been exposed to oral environment is removed. This creates irregularities on the surface and increases surface energy. This method is easy and effective for surface preparation and enhances the bond strength 19, 20). Following etching with phosphoric acid, surface morphology does not change significantly. In fact, this step aims to do a superficial cleaning following mechanical preparation 21). Mechanical preparation must be necessarily performed prior to etching, and etching alone would not be effective 21, 22). Silane is applied prior to adhesive in order to wet the surface. In fact, silane has two functional groups. Silanol bonds to silica in filler particles of composite and the organofunctional group is copolymerized with methacrylate present in adhesive, enabling a chemical bond in the process of repair 23). In our study, silane was only used without adhesive following mechanical treatment for bond in some groups in order to assess the efficacy of this step of repair process separately. Teixeira et al. 24) stated that repair bond strength must be in the range of 15 to 25 MPa. In our study, groups with silane alone (without adhesive) could not reach the minimum required repair bond strength. Laser groups obtained the mean bond strength of 4.75 and 5.63 MPa. Bur groups had slightly higher bond strength (13.85 and 14.33 MPa); however, application of bur with silane alone could not reach the minimum required repair bond strength of 15 MPa. This highlights the role of adhesive in the process of repair. Some other studies have also emphasized on the key role of adhesive in repair process and that silane alone cannot provide adequately high bond strength 25–28). In our study, all adhesive groups had adequately high repair bond strength; the mean bond strength was higher in Universal adhesive groups, which is probably attributed to the presence of functional monomers in universal adhesive. Functional monomers chemically bind to oxides via their hydrophilic phosphate terminal end and copolymerize with resin monomers via their hydrophobic methacrylate terminal end 13, 29). On the other hand, low viscosity of these adhesives enables their penetration into microscopical surface porosities and provides a better micromechanical retention 13). Pairwise comparison of groups revealed that mechanical preparation by bur provided higher bond strength than laser. Mechanical interlocking is a key factor in increasing the repair bond strength of composites. Following mechanical preparation, superficial layer of resin, which has been deteriorated due to environmental factors is removed 30) and surface roughness and free surface energy increase as such 31). Bur and laser can both cause surface roughness; however, higher efficacy of bur appears to be due to different patterns of surface roughness created following the use of bur and laser. Batista 32) stated that although laser roughens the surface, pattern of roughness is a more important factor in achieving micromechanical bond. The pattern of roughness created by laser is not suitable. Also, Tabatabaie et al. 33) stated that bur preparation creates both macro- and micro-retentive areas, which are suitable for bond while laser mainly creates macro-retentive areas; this was confirmed by our observations as well.
Evidence shows that laser parameters can significantly affect the bond strength. The higher the laser energy, the greater would be the destruction. Kimyai et al. 9) obtained results different from ours and showed that laser yielded higher bond strength than bur. However, they used 2 W laser while we used 3 W laser; difference in this parameter is probably responsible for the different results. Rossato et al. 17) and Batista et al. 32) also showed that higher power of laser would have greater destructive effects and can cause fissures in composite bulk that negatively affect adhesion. Factors other than laser parameters such as particle size and formulation of composite can also affect the volume and depth of ablation 36). It looks that the wavelength of 2780 nm is able to ablate composite resin and the ablation mechanisms might be explosive vaporization followed by a hydrodynamic ejection as Lizarelli 11) stated for Er. YAG laser which has close wavelength (2940 nm). The reason of the capacity of this wavelength(2780 nm) to ablate the composite resin is due to the strong absorption by two composite components (Silicon dioxide (SiO2) and PMMA) of the wavelengths emitting across the mid-IR with absorption bands in the 9 to 11 µm region and near 3 µm 37). Lizarelli 11) stated that hybrid composite compared to other types more easily undergoes ablation following laser irradiation. In our study, Z250 composite was used, which may explain why laser did not have a favorable effect on bond strength (since it is a hybrid composite). The initial shear bond strength had no significant difference with bond strength after aging in the groups. In fact, following aging, two phenomena occur at the bonding interface. The first one is degradation of interface due to hydrolytic degradation and the second one is post-curing. These two effects are opposite 38). In our study, it appears that these two effects were the same in terms of magnitude. However, further studies with different aging protocols such as higher thermal cycles to simulate longer clinical service or water storage for a couple of months are required to increase the chance of hydrolytic degradation. In our study, cohesive failure in groups significantly increased following the application of adhesive compared to groups with silane alone. This was especially prominent in universal adhesive groups, which confirms the significance of bonding agents in repair process to obtain chemical bonds. Universal adhesives had a higher efficacy for this purpose in our study. In groups with silane alone, especially those prepared with laser, failure modes were mostly adhesive, which indicates the significance of mechanical preparation along with the use of adhesives.
References
- 1: Bacchi A, Consani R, Sinoreti M, Feitosa V, Cavalcante L, Pfeifer C, Schneider L. (2013): Repair bond strength in aged methacrylate- and siloran-based composites. Journal of Adhesive Dentistry; 15(5):447-52 [DOI] [PubMed] [Google Scholar]
- 2: Tezvergil A., Lassila L.V.J., Vallittu P.K. (2003): Composite–composite repair bond strength: effect of different adhesion primers. Journal of Dentistry; 31(8): 521-525 [DOI] [PubMed] [Google Scholar]
- 3: Mjör IA, Moorhead JE, Dahl JE. (2000): Reasons for replacement of restorations in permanent teeth in general dental practice. International Dental Journal; 50:361-366. [DOI] [PubMed] [Google Scholar]
- 4: Mjör IA, Gordan VV. (2002): Failure, repair, refurbishing and longevity of restorations. Operative Dentistry; 27(5):528-534 [PubMed] [Google Scholar]
- 5: Boyer DB, Chan KC, Torney DL. (1978): The strength of multilayer and repaired composite resin. Journal Prosthetic Dentistry; 39:63-67 [DOI] [PubMed] [Google Scholar]
- 6: Padipatvuthikul P, Mair LH. (2007): Bonding of composite to water aged composite with surface treatments. Dental Material; 23(4)519-525 [DOI] [PubMed] [Google Scholar]
- 7: Vanckerckoven H, Lambrechts P, Van Beylen M, Davidson CL, Vanherle G. (1982): Unreacted methacrylate groups on the surfaces of composite resins. Journal of Dental Research; 61(6):791-795 [DOI] [PubMed] [Google Scholar]
- 8: Brosh T, Pilo R, Bichacho N, Blutstein R. (1997): Effect of combinations of surface treatments and bonding agents on the bond strength of repaired composites. Journal of Prosthetic Dentistry; 77(2):122-126. [DOI] [PubMed] [Google Scholar]
- 9: Kimyai S, Mohammadi N, Navimipour E, Rikhtegaran S. (2010): Comparison of the effect of three mechanical surface treatments on the repair bond strength of a laboratory composite. Journal Photomedicine and laser surgery; 28(2): S-25-S-30. [DOI] [PubMed] [Google Scholar]
- 10: Rathke A, Tymina Y, Haller B. (2009): Effect of different surface treatments on the composite-composite repair bond strength. Journal of Clinical Oral Investigation; 13(3): 317-323. [DOI] [PubMed] [Google Scholar]
- 11: Lizarelli R, Moriyama L, Pelino J, Bagnato V. (2005): Ablation rate and morphological aspects of composite resins exposed to Er:YAG laser. Journal of Oral laser applications; 5:151-160. [Google Scholar]
- 12: Papacchini F, Dall'oca S, Chieffi N, Goracci C, Sadek FT, Suh BI, Tay FR, Ferrari M. (2007): Composite to composite microtensile bond strength in the repair of a micro-filled hybrid resin: effect of surface treatment and oxygen inhibition. Journal of Adhesive Dentistry; 9(1):25-31. [PubMed] [Google Scholar]
- 13: Kim R, Woo J, Lee I, Yi Y, Hwang J, Seo D. (2015): Performance of universal adhesives on bonding to leucite-reinforced ceramic. J Kim et al. Biomaterials research; 22(19):11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14: Söderholm KJ. (1986) Flexure strength of repaired dental composites. Scandinavian Journal Dental Research; 94(4):364-9. [DOI] [PubMed] [Google Scholar]
- 15: Acharya GS, Manjunath M. (2012): The effect of surface treatments and bonding regimens on microtensile bond strengths of repaired composite: An in vitro study. Journal of Conservative Dentistry; 15(4):383-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16: Brosh T, Pilo R, Bichacho N, Blutstein R. (1997): Effect of combinations of surface treatments and bonding agents on the bond strength of repaired composites. Journal of Prosthetic Dentistry; 77(2):122-6. [DOI] [PubMed] [Google Scholar]
- 17: Rossato D. M., Bandécaa M. C., Saadea E. G., Lizarellib R. F. Z., Bagnatob V. S., Saada J. R. C. (2009): Influence of Er:YAG Laser on Surface Treatment of Aged Composite Resin to Repair Restoration. Journal of Laser Physics; 19(2):2144-2149. [Google Scholar]
- 18: Yesilyurt C, Kusgoz A, Bayram M, Ulker M. (2009): Initial repair bond strength of a nano-filled hybrid resin: effect of surface treatments and bonding agents. Journal of Esthetic Restorative Dentistry; 21(4):251-60. [DOI] [PubMed] [Google Scholar]
- 19: Hannig C, Sebastian L, Hahn P, Attin T. (2006): Shear bond strength of repaired adhesive filling materials using different repair procedures. Journal of Adhesive Dentistry; 8(1):35-40. [PubMed] [Google Scholar]
- 20: Rodrigues Junior SA, Ferracane JL, Della Bona A. (2009): Influence of surface treatments on the bond strength of repaired resin composite restorative materials. Dental Material; 25(4):442-451. [DOI] [PubMed] [Google Scholar]
- 21: Fawzy AS, El-Askary FS, Amer MA. (2008): Effect of surface treatments on the tensile bond strength of repaired water-aged anterior restorative micro-fine hybrid resin composite. Journal of Dentistry; 36(12):969-76. [DOI] [PubMed] [Google Scholar]
- 22: Melo MA, Moysés MR, Santos SG, Alcântara CE, Ribeiro JC. (2011): Effects of different surface treatments and accelerated artificial aging on the bond strength of composite resin repairs. Brazilian Oral Research; 25(6):485-91. [DOI] [PubMed] [Google Scholar]
- 23: El-Deeb H, Ghalab R, Akah M, Mobarak E. (2011): Repair bond strength of dual-cured resin composite core buildup materials. Journal of advanced research; 7(2):263-269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24: Teixeira EC, Bayne SC, Thompson JY, Ritter AV, Swift EJ. (2005): Shear bond strength of self-etching bonding systems in combination with various composites used for repairing aged composites. Journal of Adhesive Dentistry; 7:159-164. [PubMed] [Google Scholar]
- 25: Rathke A, Tymina Y, Haller B. (2009): Effect of different surface treatments on the composite-composite repair bond strength. Clinical Oral Investigation; 13(3):317-23. [DOI] [PubMed] [Google Scholar]
- 26: Staxrud F, Dahl JE. (2011): Role of bonding agents in the repair of composite resin restorations. European Journal of Oral Sciences; 119(4):316-22. [DOI] [PubMed] [Google Scholar]
- 27: Turner CW, Meiers JC. (1993): Repair of an aged, contaminated indirect composite resin with a direct, visible-light-cured composite resin. Operative Dentistry; 18(5):187-94. [PubMed] [Google Scholar]
- 28: Soderholm KJ, Roberts MJ. (1991): Variables influencing the repair strength of dental composites. Scandinavian Journal of Dental Research; 99(2):173-80. [DOI] [PubMed] [Google Scholar]
- 29: Yoshida K, Tsuo Y, Atsuta M. (2006): Bonding of dual-cured resin cement to zirconia ceramic using phosphate acid ester monomer and zirconate coupler. Journal of biomedical materials research. Part B, Applied biomaterials; 77(1):28-33. [DOI] [PubMed] [Google Scholar]
- 30: Kabeko M, Caldas RA, Feitosa VP, Consani RLX, Schneider LF, Bacchi A. (2015): Influence of surface treatments to repair recent fillings of silorane- and methacrylate-based composites. Journal of Conservative Dentistry; 18(3):242-246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31: Kusgoz A, Ülker M, Yesilyurt C, Yoldas OH, Ozil M, Tanriver M. (2011): Silorane-based composite: depth of cure, surface hardness, degree of conversion, and cervical microleakage in Class II cavities. Journal of Esthetic and Restorative Dentistry; 23(5):324-335. [DOI] [PubMed] [Google Scholar]
- 32: Batista G, Kamozaki M, Gutierrez N, Caneppele T, Torres C. (2015): Effects of different surface treatments on composite repairs. Journal of Adhesive dentistry; 17(5):421-426. [DOI] [PubMed] [Google Scholar]
- 33: Hasani Tabatabaei M, Alizade Y, Taalim S. (2004): Effect of various surface treatment on repair strength of composite resin. Journal of Dentistry (TUMS); 1:5-11. [Google Scholar]
- 34: Baktas O, Eren D, Siso S, Akin G. (2012): Effect of thermocycling on the bond strength of composite resin to bur and laser treated composite resin. Journal of Laser Medical Sciences; 27(4):723-728 [DOI] [PubMed] [Google Scholar]
- 35: Hatipo lu M, Barutcigil Ç. (2015): Effects of erbium–and chromium–doped yttrium scandium gallium garnet and diode lasers on the surfaces of restorative dental materials: A scanning electron microscope study. Nigerian Journal of Clinical Practice; 18(2):213-220 [DOI] [PubMed] [Google Scholar]
- 36: Lizarelli F.Z., Moriyama T., Bagnato V.S. (2003): Ablation of Composite Resins Using Er:YAG Laser-Comparison With Enamel and Dentin. Lasers in Surgery and Medicine; 33(2):132-139 [DOI] [PubMed] [Google Scholar]
- 37: Correa-Afonso AM, Palma-Dibb RG, Pécora JD. Composite filling removal with erbium:yttrium-aluminum-garnet laser: morphological analyses. Lasers Medical Sciences. 2010 Jan;25(1):1-7. [DOI] [PubMed] [Google Scholar]
- 38: Hamano N, Chiang Y, Nyamaa I, Yamaguchi H, Ino S, Hickel R, Kunzelmann K. (2012): Repair of siloran-based dental composites: influence of surface treatments. Journal of Dental materials; 28(8):894-902. [DOI] [PubMed] [Google Scholar]