

Abstract
Head and neck neoplasia can affect certain fundamental functions, including eating, drinking, speaking and respiration. One overriding factor in deciding on treatment policy is the tendency for head and neck malignancy to be limited to the primary site and regional lymph nodes with surgery and chemotherapy and radiotherapy. The aim of the study was to analyze the occurrence of Head and Neck tumours operated at ENT clinic Tuzla, University Clinical Center Tuzla, Bosnia and Herzegovina. Medical records of patients with histopathologically confirmed head and neck malignancies over a 5 year period (2003-2007) were analyzed. Eight hundred and eight one (881) cases, made up of 519 (58,8%) males and 362 (41,1%) females were found. The most common sites for head and neck malignancies were found to be in the larynx (26,1%), oral cavity (21,7%), the thyroid gland (14,64 %) and the neck (8,51%). A total of 230 patients were diagnosed with laryngeal carcinoma (M:173; E57), showing the increasing number of female patients. The histopathological tumour types found in this work were mostly squamous cell carcinoma (72,09%), papillary carcinoma (12,2%), while many other minor histopathological variants accounted for 13%. The most patients were presented with stage I and stage III of disease (27% and 28,3%), and 19,9% with stage IV. About 40% of patients did not have data about smoking habit and alcohol drinking. The incidence of head and neck tumours seems to be relatively high, but without significant increase during investigated period. More investigation concerning risk factors, diagnostic procedures, and management strategies should be done in future.
Keywords: head and neck tumours, epidemiology, sex, stage, distribution
INTRODUCTION
Head and neck neoplasia can affect certain fundamental functions including eating, drinking, speaking and respiration (1). Head and neck tumours (HNT) consist of a diverse group of tumours that ranges from cutaneous, lip, salivary glands, sinuses, oral cavity, pharynx and laryngs. Presently, HNT is six most prevalent neoplasms in the world, with approximately 900.000 cases diagnosed worldwide per year. Prognosis has improved little in the past 30 years (2). Males are approximately three times more likely to develop squamos cancers of the head and neck (oral cavity, pharynx and larynx) than females. Very few prospective studies have examined the association between cigarette smoking and cancer of the head and neck in women, even though the rates of smoking in women are increasing rapidly worldwide (3). In the U.S., public health efforts at tobacco control and education have successfully reduced the prevalence of cigarette smoking, resulting in a lower incidence of head and neck cancer (4). Cancer rate of the head and neck are traditionally linked to public health issues. Alcohol use appears to be an independent risk factor and acts synergistically with tobacco use in causing HNT (5). Chronic consumption of alcoholic beverages is an accepted social custom worldwide. In the upper aero digestive tract, local morphologic, metabolic and functional alterations are present due to alcohol consumption. A clinical link between the chronic consumption of alcohol and head and neck cancer has been observed for decades (6). Other risk factors include HPV, poor diet, certain occupations and occupational exposures, low education and socioeconomic status, immunodeficiency, poor oral hygiene, GERD, benign conditions, family history of cancer and other (5).
MATERIALS AND METHODS
Medical records of patients with hystopathologically confirmed head and neck malignancies over a 5 year period (2003-2007) were analyzed according to: sex, location of tumour, histopathological type and stage of tumour.
RESULTS
A total of 881 cases were recorded consisting 519 (58,8%) males and 362 (41,1%) females. The mean age of the patients was 50,7 years (Figure 1). The most common sites for head and neck malignancies were found to be in the larynx (26,1%), oral cavity (21,7%), the thyroid gland (14,64 %), skin (19,1%) and the neck (8,51%) (Figure 2). Total of 230 patients was diagnosed with laryngeal carcinoma M:173; F:57), (showing the increasing number of female patients (Figure 3).
FIGURE 1.
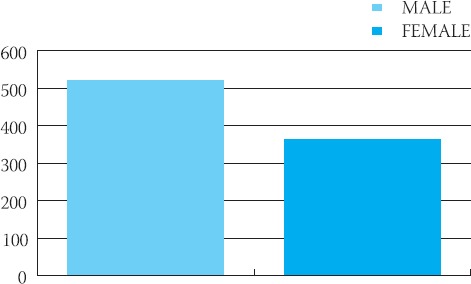
Sex distribution of patients with HNT
FIGURE 2.
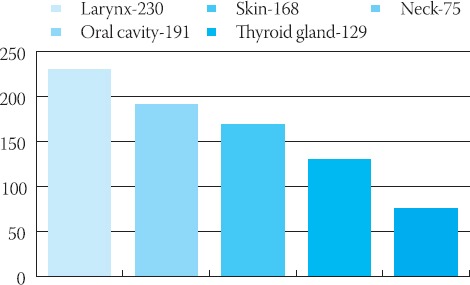
Localization of the HNT tumour
FIGURE 3.
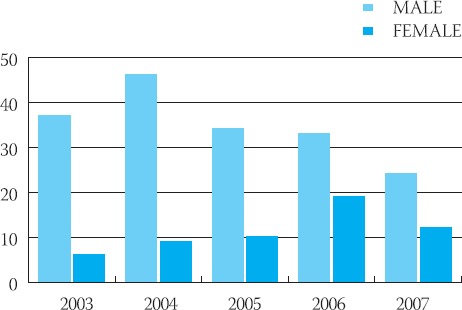
Increasing number of female patients with laryngeal cancer
A total of 43 patients in 2003 were recorded consisting of 37 males (86%) and 6 females (14%). In 2004 there were 46 (83,6%) males and 9 (16,4%) females of 55 operated patients. In 2005 there were 44 operated tumour of the larynx, with 34 (77,2%) males and 10 (22,8%) females. From 2005 to 2007 there were increasing number of female patients, in 2006 (52 patients were operated) there were 33 (63,4%) males and 19 (36,6%) females, and 2007 (36 patients were operated) there were 24 (66,6%) males and 12 (33,4%) females. Thyroid gland tumours were presented at 14,64% of the all operated tumours with notable female predominance (Figure 4).
FIGURE 4.
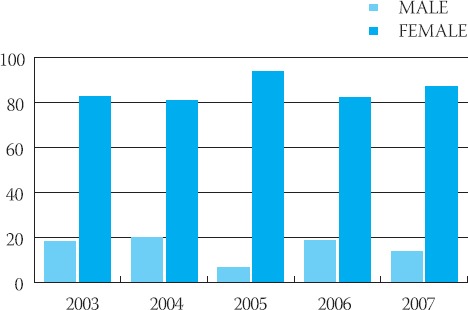
Sex distribution of thyroid gland tumours
The histopatological malignant tumour type found in this work were squamous cell carcinoma (72,1%), papillary carcinoma (12,2%), basocellular carcinoma (8,7%), while many other minor histopathological variants accounted for 7 % (Figure 5).
FIGURE 5.
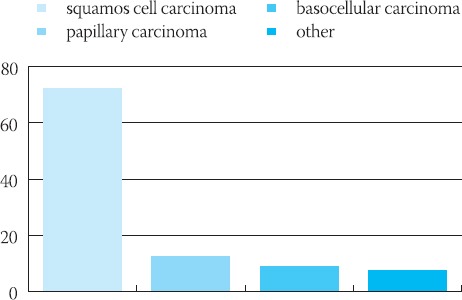
Histopatological type of HNT tumors
Squamous cell carcinomas were the most common malignancy. Sarcomas and lymphomas were typically rare. Squamos cell carcinomas continue to dominate head and neck cancer with notable male prevalence (7). Malignant neoplasm’s were 40,4 % and benign neoplasm’s were 59,6% of all operated head and neck tumours. The most patients were presented with stage I (27%). With stage II there were 24,78%, stage III 28,31% and stage IV 19,91% (Figure 6). Thyroid neoplasm’s were mostly papillary carcinoma at 89,3% or 28,2% of all operated thyroid tumours. Benign tumours, polyps were the most frequent (22,3%).
FIGURE 6.
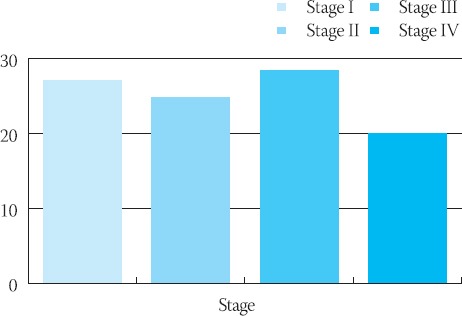
Stage of malignant neoplasms
DISCUSSION
The geographical variations in incidence and mortality are indicative of differences in the prevalence of risk factors between countries. In the U.S. and France, public health efforts at tobacco control and education have successfully reduce the prevalence of smoking, resulting in a lower incidence of laryngeal carcinoma (4, 8). Compared with study of Davis (9) we have increasing incidence of the laryngeal carcinoma, and decreasing incidence of thyroid tumours. Although, the prevalence of laryngeal carcinoma is increasing among females than at males. Very few prospective studies have examined the association between cigarette smoking and laryngeal cancer in females, even though the rates of smoking in women are increasing rapidly worldwide. Comparing the analysis of Tumino (10) and our study, laryngeal carcinoma showed significant increasing trend among females, trend is stable among males. Compared with patients in the Yemen (11), our patients were typically female (41,1% vs. 36,1%), no significant old at disease presentation (mean 50,7 vs. 50 years), had mainly tumour of the larynx (26,1 % vs. 8%), and had less tumours of oral cavity (21,7% vs. 47%). There was no statistically significant difference at incidence of thyroid tumours between our study and study of Thapa and al. (12). Although, our patients had mainly papillary carcinoma. Our study confirms that squamous cell carcinomas continue to dominate, and most common stages are stage I and stage III (13, 14, 15, 16).
CONCLUSION
The analysis of 230 laryngeal carcinomas in period 2003-2007 shows diverging trend between sexes, in fact rates decrease significantly among males and increase among females. Increasing number of women with laryngeal carcinoma correlate with their increasing use of cigarettes. Many head and neck tumours have changing incidence and mortality rates contrary to expected changes given trends in public health issues. Further investigation of risk factors, diagnostic practices, and management strategies is warranted. The prognosis in head and neck tumour patients depends on clinical stage at the time of diagnosis, therefore, identification of high-risk population, precancerous lesions and early diagnosis decrease mortality. Nevertheless, the major effort must be on primary prevention.
REFERENCES
- 1.Dhillon RS, East CA. 2nd edition. Vol. 88. Churchill, Livingstone; 2005. Ear, nose and throat and head and neck surgery; p. 89. [Google Scholar]
- 2.Chin D, Boyle GM, Porceddu S, Theile DR, Parsons PG, Coman WB. Head and neck cancers: past, present and future. Expert Rev Anticancer Ther. 2006;6(7):1111–1118. doi: 10.1586/14737140.6.7.1111. [DOI] [PubMed] [Google Scholar]
- 3.Freedman ND, Abnet CC, Leitzmann MF, Hollenbeck AR, Schatzkin A. Prospective investigation of the cigarette smoking-head and neck cancer association by sex. Cancer. 2007;110(7):1593–1601. doi: 10.1002/cncr.22957. [DOI] [PubMed] [Google Scholar]
- 4.Sturgi EM, Cinciripini PM. Trends in head and neck cancer incidence in relation to smoking prevalence: an emerging epidemic of HPV-associated cancers? Cancer. 2007;110(7):1429–1435. doi: 10.1002/cncr.22963. [DOI] [PubMed] [Google Scholar]
- 5.Water RW, Staecker H. Otolaryngology basic science and clinical rewiew. 2006;(chapter 10A):138–139. [Google Scholar]
- 6.Riedel F, Goessler UR, Hormann K. Alcohol-related diseases of the mouth and throat. Dig. Dis. 2005;23(3-4):195–203. doi: 10.1159/000090166. [DOI] [PubMed] [Google Scholar]
- 7.Wake M. ENT cancer in West Midlands region of England. J. Laryngol Otol. 1993;107(4):313–315. doi: 10.1017/s002221510012290x. [DOI] [PubMed] [Google Scholar]
- 8.Moriniere S. Epidemiology of head and neck cancer. Rev. Prat. 2006;56(15):1637–1541. [PubMed] [Google Scholar]
- 9.Davies L, Welch HG. Epidemiology of head and neck cancer in United States. Otolaryng. Head Neck Surgery. 2006;135(3):451–457. doi: 10.1016/j.otohns.2006.01.029. [DOI] [PubMed] [Google Scholar]
- 10.Tumino R, Vicario G. Head and neck cancers: oral cavity, pharynx and larynx. Epidemio Rev. 2004;28(2 Suppl):28–33. [PubMed] [Google Scholar]
- 11.Nasr AH, Khatri ML. Head and neck squamos cell carcinoma in Hajjah, Yemen. Saudi Med. J. 2000;21(6):565–568. [PubMed] [Google Scholar]
- 12.Thapa N, Jha AK, Rijal JP, Shah A. Study on head and neck tumors presented in ENT OPD of Nepal Medical College Teaching Hospital. Nepal Med. Coll. J. 2003;5(2):79–81. [PubMed] [Google Scholar]
- 13.Esteller More E, Quer M, Fabra JM, Garcia P, Leon X, Viladot J, Burgues J. Nasopharyngeal carcinoma. An epidemiological and clinical study. Anal. Otorrinolaringol. Ibero Am. 1990;17(5):473–494. [PubMed] [Google Scholar]
- 14.Quer M, Leon X, Orus C, Recher K, Gras JR. Analysis of 2500 squamos cell carcinoma of the head and neck. Acta Otorrinolaringol. Esp. 2001;52(3):201–205. doi: 10.1016/s0001-6519(01)78198-8. [DOI] [PubMed] [Google Scholar]
- 15.Onyango JF, Awange DO, Njiru A, Maharia IM. Pattern of occurrence of head and neck cancer presenting at Kenyatta National Hospital, Nairobi. East Africa J. Med. 2006;83(5):288–291. doi: 10.4314/eamj.v83i5.9435. [DOI] [PubMed] [Google Scholar]
- 16.Wake M. ENT cancer in the West Midlands region of England. J. Laryngol Otol. 1993;107(4):313–315. doi: 10.1017/s002221510012290x. [DOI] [PubMed] [Google Scholar]