

Rickettsial retinitis is increasingly being reported from the Indian subcontinent.[1,2] Rickettsia has to be considered in the standard list of differential diagnosis for cases of postfever retinitis/epidemic retinitis. It is definitely controversial whether a case of epidemic retinitis is because of direct microbial invasion or an immune-mediated phenomenon. The authors of “Rickettsial retinitis: Direct bacterial infection or an immune-mediated response?” have presented a single case report of rickettsial retinitis and reported improvement after the use of oral doxycycline. The authors have also reported initial worsening with steroids and antivirals.
We report a case of a 54-year-old woman who presented with diminution of vision in her right eye for 10 days. She reported a fever about 3 weeks before her visual complaints. The visual acuity in the right eye was 3/60 N18, and left eye was 6/6 N6 (+2.5D add). On examination, the anterior segment was unremarkable in both eyes. In the right eye, she had vitritis grade 1+ and yellowish-white retinitis patches in the superotemporal quadrant along the arcade with macular edema [Fig. 1a]. The spectral domain optical coherence tomography (RTVue, Optovue) showed subfoveal serous detachment along with cystoid spaces in the right eye [Fig. 2a]. Left eye was within normal limits. Hypertension and diabetes were ruled out. Initial workup for tuberculosis (Mantoux, chest X-ray, Quantiferon Gold), HIV, dengue (ELISA), chikungunya (ELISA), and West Nile virus (ELISA) was negative. She was empirically started on oral acyclovir 400 mg 12 hourly. At 1-week follow-up, she reported worsening of symptoms, vision dropped to 1/60 in the right eye. The fundus picture revealed increase in vitritis and the number of retinitis patches [Fig. 1b]. A fundus fluorescein angiography (TRC-50 Dx, Topcon) at this juncture revealed hypofluorescence corresponding to the areas of retinitis [Fig. 2c] that gradually showed hyperfluorescence at the edge of the retinitis lesions, especially in the area superotemporal to disc [Fig. 2d]. Oral steroids were now begun (1 mg/kg/day) and in a week's time, there was further worsening of symptoms. The vision deteriorated to counting finger at ½ m with further increase in vitritis and retinitis [Fig. 1c]. The fovea had flattened, but there was increased reflectivity in the nasal retina corresponding to the retinitis patches [Fig. 2b]. A Weil–Felix test was admittedly done only at this point, which revealed raised titers of OX2 (1:160 Progen, Tulip Diagnostics, Bengaluru, Karnataka, India). Oral steroids were stopped and oral doxycycline was started at 100 mg 12 hourly. The patient had dramatic resolution of symptoms with reduction in vitritis and retinitis at 1-week follow-up [Fig. 1d]. Doxycycline was given for 2 weeks in this patient.
Figure 1.
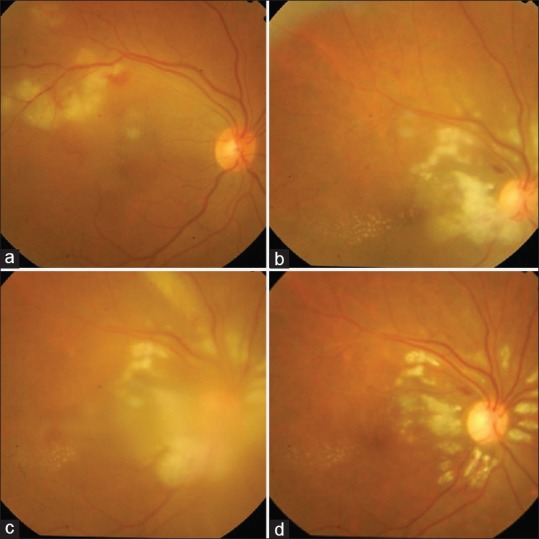
A photo collage demonstrating worsening of the fundus picture in the right eye with oral antiviral agents and steroids, followed by resolution with oral doxycycline. (a) Cotton wool spots suggestive of retinitis patches in the superotemporal quadrant along the vessel distribution. (b) Increase in the retinitis patches after a course of oral acyclovir, this time in a peripapillary distribution. Hard exudates in the macular area owing to resolution of the macular edema. Superficial hemorrhage superotemporal to disc. (c) Further increase in the retinitis patches along the vessels radiating superior to disc and increase in vitritis (after a week of oral steroids). Steroids were discontinued at this point. (d) Dramatic resolution with reduction in the retinitis patches and vitritis after 1 week of oral doxycycline therapy
Figure 2.
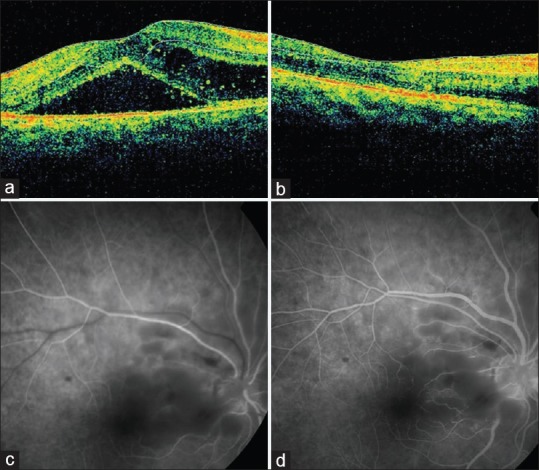
Spectral domain optical coherence tomography and fundus fluorescein angiography. (a) Spectral domain optical coherence tomography showing subfoveal fluid and cystoid spaces. (b) Spectral domain optical coherence tomography after 1 week of oral doxycycline. Resolution of macular edema, but nasal fovea shows hyperreflective inner layers corresponding to retinitis patches. (c) Fundus fluorescein angiography corresponding to Fig. 1b – hypofluorescence corresponding to retinitis patches (Early frames). Small blotches of blocked fluorescence owing to superficial hemorrhages. (d) Late frames of fundus fluorescein angiography showing mild capillary leakage at the edge of the hypofluorescent patches and mild vessel wall staining at the disc margin, inferiorly
Rickettsiosis is known to have a preferential vascular dissemination to endothelium of neural tissues.[3] The increased vascular permeability in retinal tissue mediated by natural killer (NK) cells and cytotoxic T-lymphocytes may explain the microvascular leakage leading to subfoveal and intraretinal fluid seen in retinitis. Although immune-mediated endothelial injury is one hypothesis, Heinzen has described rickettsial intracellular mobility and intercellular spread demonstrating direct bacterial invasion.[4]
Although not sensitive/specific, Weil–Felix test is a simple, inexpensive test for rickettsiosis. Either 4-fold rise in agglutinin titer in paired sera or single titer of more than 1:80 is considered diagnostic.[5] Rise in titers is difficult to demonstrate in retinitis patients because of the interval of 2–4 weeks between the fever and ocular presentation and inability of a retina specialist to do this test at the time of fever. Serum ELISA, particularly immunoglobulin M (IgM), is the most sensitive test available for rickettsial diagnosis and the presence of IgM antibodies indicates recent infection with rickettsial disease.[6] Immunofluorescent assay (IFA) is considered the gold standard for rickettsial infection;[7] but due to its limited availability and lack of technical expertise, it is not accessible to most physicians in India. Polymerase chain reaction (PCR) is a rapid and specific test for diagnosis of rickettsia. It can be used to detect rickettsial DNA in blood and tissue samples.[8] Aqueous/vitreous testing by PCR for rickettsia maybe a closer test to know if rickettsial retinitis is due to direct invasion or immune mediated.
Kawali et al. have evaluated 19 eyes of 11 patients with rickettsial retinitis and have employed oral steroids, oral doxycycline, and posterior subtenon injection of steroids variably. They found better results with a steroid only regimen and reported a final mean visual acuity of 20/30 in their series.[1] A favorable response to doxycycline like in our case and worsening with steroids might lead us to believe the retinitis is due to direct invasion of the microorganism. It is, however, interesting to note that doxycycline also has immunomodulatory properties. It is known to regulate cytokines, especially interleukin 6 (IL-6), IL-1 β, and tumor necrosis factor-α.[9] Hence, in a case of rickettsial retinitis, whether doxycycline ameliorates the immune response to the rickettsial organism or acts directly against the organism cannot be determined.
In conclusion, rickettsial retinitis must be suspected in all cases of postfever retinitis negative for dengue, chikungunya, or West Nile. The diagnosis of rickettsial retinitis must be based on specific tests such as ELISA and IFA. Weil–Felix test is definitely a screening tool, is inexpensive and freely available, but lacks specificity. Randomized trials are needed to analyze whether steroids, antibiotics, or steroid-antibiotic combination regimens are effective for these cases of retinitis. At present, evidence in part for direct bacterial invasion is only based on anecdotal reports such as ours and partial understanding of the pathogenic mechanisms of rickettsial retinitis.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Kawali A, Mahendradas P, Srinivasan P, Yadav NK, Avadhani K, Gupta K, et al. Rickettsial retinitis-an Indian perspective. J Ophthalmic Inflamm Infect. 2015;5:37. doi: 10.1186/s12348-015-0066-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kamath Y, Gonsalves S, Vivekanada U, Bhat SS, Rajurkar K. Bilateral presumed macular retinitis secondary to Rickettsial infection in South India. Trop Doct. 2017;47:186–8. doi: 10.1177/0049475516660466. [DOI] [PubMed] [Google Scholar]
- 3.Walker DH, Valbuena GA, Olano JP. Pathogenic mechanisms of diseases caused by Rickettsia. Ann N Y Acad Sci. 2003;990:1–11. doi: 10.1111/j.1749-6632.2003.tb07331.x. [DOI] [PubMed] [Google Scholar]
- 4.Heinzen RA. Rickettsial actin-based motility: Behavior and involvement of cytoskeletal regulators. Ann N Y Acad Sci. 2003;990:535–47. doi: 10.1111/j.1749-6632.2003.tb07424.x. [DOI] [PubMed] [Google Scholar]
- 5.Ajantha GS, Patil SS, Chitharagi VB, Kulkarni RD. Rickettsiosis: A cause of acute febrile illness and value of Weil-Felix test. Indian J Public Health. 2013;57:182–3. doi: 10.4103/0019-557X.119817. [DOI] [PubMed] [Google Scholar]
- 6.Rathi N, Rathi A. Rickettsial infections: Indian perspective. Indian Pediatr. 2010;47:157–64. doi: 10.1007/s13312-010-0024-3. [DOI] [PubMed] [Google Scholar]
- 7.Rahi M, Gupte MD, Bhargava A, Varghese GM, Arora R. DHR-ICMR Guidelines for diagnosis & management of Rickettsial diseases in India. Indian J Med Res. 2015;141:417–22. doi: 10.4103/0971-5916.159279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Renvoisé A, Rolain JM, Socolovschi C, Raoult D. Widespread use of real-time PCR for rickettsial diagnosis. FEMS Immunol Med Microbiol. 2012;64:126–9. doi: 10.1111/j.1574-695X.2011.00899.x. [DOI] [PubMed] [Google Scholar]
- 9.Castro J, Fredeking T. Doxycycline modify the cytokine storm in patients with dengue and dengue hemorrhagic fever. Int J Infect Dis. 2010;14:e44. [Google Scholar]