

The propagation of the electrical wave fronts in the atrial myocardium is complex and depends on discontinuities at multiple size scales, from the ionic dimension to the macroscopic structure. In some regions of the human atria, the myocardial fibers organize in well demarcated structures where fiber orientation favors a highly anisotropic condition forcing the electrical impulse to propagate mostly along the long axis of the muscle bundles. The latter organize in fascicles of variable thickness and number, which contributes to fast electrical propagation and enables efficient electromechanical coupling of both atria during each normal sinus beat.1 Bachmann’s bundle and the septo-pulmonary bundle are two mayor examples of bundles that sustain fast and laminar fluxes of electrical waves moving away from the sinus node. However, while Bachmann’s bundle extends mostly subepicardially across the interatrial groove, the septo-pulmonary bundle occupies a deeper level,1 which implies that even during sinus rhythm the propagation of waves is not uniform across the atrial wall. In fact, a certain degree of dissociation exists between the epicardium and the endocardium even for well-structured myocardial layers. Moreover, in some areas of the atrial wall, the uniform distribution of myocardial fibers is disrupted by multiple intricate crossings of fibers (Figure),2 which underlie the non-uniform anisotropic propagation that characterizes, for example, the crista terminalis and the antrum of the pulmonary veins (PVs). Altogether, such an intricate architecture is responsible for the efficient but highly non-linear propagation of sinus waves, but has also been demonstrated to underlie the initiation and maintenance of cardiac arrhythmias.3,4
Figure.
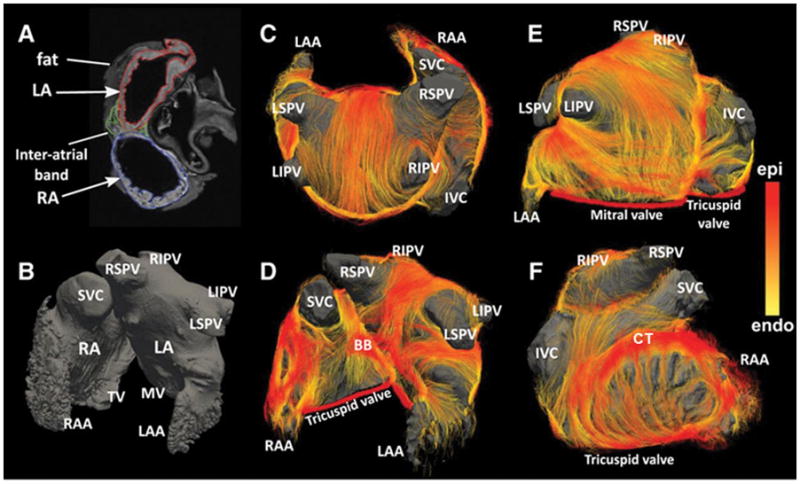
Acquired geometry and fiber visualization results in human atria specimens. Left, Atrial geometry. A, Short-axis view of a nondiffusion-weighted image (b0) with superimposed segmentation of left atrium (LA; red), right atrium (RA; blue), and interatrial bundles (green). Fat tissue surrounding the atria is excluded from the segmentation. B, Anterior view of left and right atria created from T1-weighted images; the dark grey volume represents lumen. Right, Fiber visualization using tractography. C, Posterior view of atrial roof. D, Anterior view. E, Inferior and left lateral views. F, View of right atrium. Color encodes the local distance to the endocardial shell: yellow is the endocardial layer, and red is the epicardial layer. BB indicates Bachman bundle; CT, crista terminalis, IVC, inferior vena cava; LAA, left atrial appendage; LIPV, left inferior pulmonary vein; LSPV, left superior pulmonary vein; MV, mitral valve; RAA, right atrial appendage; RIPV, right inferior pulmonary vein; RSPV, right superior pulmonary vein; SVC, superior vena cava; and TV, tricuspid valve. Modified from Pashakhanloo F et al. Circ Arrhythm Electrophysiol. 2016;9:e004133, by permission.
A number of studies have analyzed the patterns of sinus wave propagation in the human atria, but most of the data published to date have displayed sequences of activation recorded only on the endocardium.5 Evidence was lacking on propagation confined to the epicardium, and to our knowledge, no simultaneous endo-epicardial mapping studies had been conducted during sinus rhythm in the human heart. Experimental studies in dogs did show that epicardial and endocardial activation could be discordant at specific locations of the normal atria and that discordance increased when activation was premature.6 The latter opened the door for the study of transmural conduction from the subendocardium to the subepicardium, which also allowed for the demonstration of endo-epicardial asynchrony of propagation during atrial fibrillation (AF) in the human heart.7 In this issue of Circulation Arrhythmia & Electrophysiology, Mouws and colleges demonstrate that epicardial breakthrough waves (EBW) are recorded during sinus rhythm in the diseased atria of patients undergoing cardiac surgery.8 The unipolar electrograms recorded at EBW locations mostly consisted of clear R waves initiating the recordings, which was a solid and reliable piece of evidence to suggest that EBW represented propagation of electrical wave fronts from deeper layers. EBW were observed in a minority of cases on Bachmann’s bundle but they were widespread along different regions of both atria including the pulmonary vein (PV) antra. The latter agrees with the concept of preferential laminar fluxes in well demarked atrial fascicles versus much more complex patterns of propagation in areas of non-uniform anisotropy, either in the normal or the diseased myocardium. Altogether, the findings of Mouws et al, contribute to a better understanding of the complex patterns of propagation of sinus waves in the human atria and pave the way for individualized analyses that depend on precise characterization of the pathophysiologic substrate affecting propagation in each patient.
Mouws et al have made the intriguing observation that ischemic cardiomyopathy seems to be the pathophysiologic substrate with the highest incidence of EBW. There is increasing evidence suggesting that chronic ischemia and scar secondary to ischemic necrosis play major roles in electrophysiological remodeling and the mechanism supporting atrial arrhythmias in humans.9,10 Postoperative AF is more frequent in patients undergoing coronary bypass grafting when chronic occlusion of the main arteries irrigating the atria is demonstrated,11 also in cases of severe disease of the right coronary artery (main origin of atrial arteries in comparison with other vascular territories).12 Thus there may be a robust link between chronic ischemic lesions and atrial arrhythmias, which might also promote abnormal patterns of electrical propagation during sinus rhythm. The variably scarred tissue in the atria of patients with ischemic cardiomyopathy might increase non-uniform anisotropy leading to abnormal patterns of transmural propagation from endocardium to epicardium, which may explain the results obtained by Mouws and colleagues.8 Similar to scar-related non-uniform anisotropy, lines of endocardial block after radiofrequency-based ablation have been elegantly related to epicardial-to-endocardial breakthrough sites, which suggest the presence of an alternative pathway on the opposite side of the atrial wall. Moreover, persistent epicardial conduction leading to endocardial breakthrough sites after the endocardial ablation line, may also be critical in maintaining a macro-reentrant circuit.13
The data of Mouws and colleagues might have several potential clinical implications. For example, endocardial-epicardial dissociation may be a reasonable way to explain variable patterns of activation during focal atrial tachycardia, and the frequent failure to accurately predict the tachycardia origin from the p-wave morphology (analogous to the QRS ventricular tachycardia in patients with extensive myocardial infarction). It is also possible that epicardial-to-endocardial dissociation is a mechanism of AF maintenance. In this regard, the often invoked observation that EBW are frequent in persistent and long-term persistent AF14,15 would suggest that patients with frequent EBW during sinus rhythm would be more prone to develop AF. Surprisingly, such a hypothesis is untenable in light of the work by Mouws et al, who showed that ≈70% of the patients developing postoperative AF had no EBW.8 Instead their data suggest that EBW seen in sinus rhythm have no relationship with mechanisms supporting postoperative AF. Alternatively, confounding factors such as heart injury leading to inflammation, might have mitigated the ability of EBW to predict postoperative AF. Therefore, whether that or any other mechanism contributed to establish the appropriate conditions needed to sustain AF cannot be predicted from the study of Mouws et al.8 Another clinical question relates to the fact that valve surgery, in particular mitral valve surgery, is recognized as a powerful risk factor for postoperative AF in comparison with other surgical procedures including coronary bypass grafting.16 However, Mouws and colleges8 found that the distribution of EBW is significantly narrower in patients with valve disease than patients with ischemic cardiomyopathy, which is inconsistent with EBW playing a significant role in the pathophysiology of postoperative AF.
What else can we learn about AF mechanisms from mapping during sinus rhythm? Other authors have previously analyzed conditions during sinus rhythm and atrial pacing that might explain AF initiation and maintenance.17 Abnormal areas of conduction delay and lines of conduction block are formed in the posterior wall of the left atrium in patients with atrial enlargement and structural heart disease, which may initiate reentry around the PVs.4 Some animal models have also demonstrated rate dependency of the safety of propagation through the atrial architecture, leading the normal conduction during sinus rhythm to turn into conduction delay, block and wavebreak formation when the firing from a PV exceeds a critical rate.3 Considering such rate dependency, one may ask, are EBW observed during sinus rhythm functionally active during AF? It is hard to make predictions, and confirmation would be even more difficult in the light of the highly non-linear dynamics governing AF. Another question is, if sinus rhythm EBW predominate in ischemic cardiomyopathy patients, what is the relationship of EBW with the myocardial scar? Extensive scar tissue is a predictor of AF recurrence after PV isolation while additional ablation at the periphery of the scar seems to increase the probability to achieve freedom from AF during follow-up.18 Some studies suggest that reentrant activity at the periphery of the scar tissue can sustain AF,19 which may be formed in the setting of non-uniform anisotropy, and may also provide conditions for transmural conduction during sinus rhythm. The latter might help understand the hierarchical organization of wave propagation during human AF,20 which is otherwise difficult to explain by widespread, randomly distributed endo-epicardial dissociation.14 The article by Mouws and colleges8 provides novel and important clues to understand the complex propagation dynamics of sinus waves in the human atria, and convincingly realizes that the laminar electrical fluxes that were usually believed to occur during sinus rhythm may in fact abruptly become turbulent. However, even after accounting for their clinical correlations, the possible role of sinus rhythm EBW in the mechanism of human AF maintenance remains elusive at best. Clinically relevant animal model studies that integrate high-resolution electrode mapping with the underlying 3-dimensional structural substrate (e.g., scar and myocardial fiber distribution) may provide a unique opportunity to establish whether EBW are relevant to AF initiation and/or maintenance.
Supplementary Material
Acknowledgments
Sources of Funding: Supported in part by the National Heart, Lung, and Blood Institute (R01 Grant HL122352) to JJ and Fondos FEDER, Madrid, Spain to JJ and DF. The CNIC is supported by the Ministry of Economy, Industry and Competitiveness (MINECO) and the Pro-CNIC Foundation, and is a Severo Ochoa Center of Excellence (MINECO award SEV-2015-0505.
Footnotes
Disclosures: JJ is a consultant for Abbott EP and receives research funding from Medtronic, Inc.
References
- 1.Ho SY, Anderson RH, Sánchez-Quintana D. Atrial structure and fibres: morphologic bases of atrial conduction. Cardiovasc Res. 2002;54:325–336. doi: 10.1016/s0008-6363(02)00226-2. [DOI] [PubMed] [Google Scholar]
- 2.Pashakhanloo F, Herzka DA, Ashikaga H, Mori S, Gai N, Bluemke DA, Trayanova NA, McVeigh ER. Myofiber Architecture of the Human Atria as Revealed by Submillimeter Diffusion Tensor Imaging. Circ Arrhythm Electrophysiol. 2016;9:e004133. doi: 10.1161/CIRCEP.116.004133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Klos M, Calvo D, Yamazaki M, Zlochiver S, Mironov S, Cabrera J-A, Sanchez-Quintana D, Jalife J, Berenfeld O, Kalifa J. Atrial septopulmonary bundle of the posterior left atrium provides a substrate for atrial fibrillation initiation in a model of vagally mediated pulmonary vein tachycardia of the structurally normal heart. Circ Arrhythm Electrophysiol. 2008;1:175–183. doi: 10.1161/CIRCEP.107.760447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Roberts-Thomson KC, Stevenson IH, Kistler PM, Haqqani HM, Goldblatt JC, Sanders P, Kalman JM. Anatomically determined functional conduction delay in the posterior left atrium relationship to structural heart disease. J Am Coll Cardiol. 2008;51:856–862. doi: 10.1016/j.jacc.2007.11.037. [DOI] [PubMed] [Google Scholar]
- 5.Lemery R, Soucie L, Martin B, Tang ASL, Green M, Healey J. Human study of biatrial electrical coupling: determinants of endocardial septal activation and conduction over interatrial connections. Circulation. 2004;110:2083–2089. doi: 10.1161/01.CIR.0000144461.83835.A1. [DOI] [PubMed] [Google Scholar]
- 6.Schuessler RB, Kawamoto T, Hand DE, Mitsuno M, Bromberg BI, Cox JL, Boineau JP. Simultaneous epicardial and endocardial activation sequence mapping in the isolated canine right atrium. Circulation. 1993;88:250–263. doi: 10.1161/01.cir.88.1.250. [DOI] [PubMed] [Google Scholar]
- 7.de Groot N, van der Does L, Yaksh A, Lanters E, Teuwen C, Knops P, van de Woestijne P, Bekkers J, Kik C, Bogers A, Allessie M. Direct Proof of Endo-Epicardial Asynchrony of the Atrial Wall During Atrial Fibrillation in Humans. Circ Arrhythm Electrophysiol. 2016;9:e003648. doi: 10.1161/CIRCEP.115.003648. [DOI] [PubMed] [Google Scholar]
- 8.Mouws EMJP, Lanters EAH, Teuwen CP, van der Does LJME, Kik C, Knops P, Bekkers JA, Bogers AJJC, de Groot NMS. Epicardial Breakthrough Waves during Sinus Rhythm: Depiction of the Arrhythmogenic Substrate? Circ Arrhythm Electrophysiol. 2017;10:e005145. doi: 10.1161/CIRCEP.117.005145. [DOI] [PubMed] [Google Scholar]
- 9.Nishida K, Qi XY, Wakili R, Comtois P, Chartier D, Harada M, Iwasaki Y, Romeo P, Maguy A, Dobrev D, Michael G, Talajic M, Nattel S. Mechanisms of atrial tachyarrhythmias associated with coronary artery occlusion in a chronic canine model. Circulation. 2011;123:137–146. doi: 10.1161/CIRCULATIONAHA.110.972778. [DOI] [PubMed] [Google Scholar]
- 10.Alasady M, Shipp NJ, Brooks AG, Lim HS, Lau DH, Barlow D, Kuklik P, Worthley MI, Roberts-Thomson KC, Saint DA, Abhayaratna W, Sanders P. Myocardial infarction and atrial fibrillation: importance of atrial ischemia. Circ Arrhythm Electrophysiol. 2013;6:738–745. doi: 10.1161/CIRCEP.113.000163. [DOI] [PubMed] [Google Scholar]
- 11.Kolvekar S, D’Souza A, Akhtar P, Reek C, Garratt C, Spyt T, Akhatar P. Role of atrial ischaemia in development of atrial fibrillation following coronary artery bypass surgery. Eur J Cardiothorac Surg. 1997;11:70–75. doi: 10.1016/s1010-7940(96)01095-0. [DOI] [PubMed] [Google Scholar]
- 12.Pehkonen E, Honkonen E, Mäkynen P, Kataja M, Tarkka M. Stenosis of the right coronary artery and retrograde cardioplegia predispose patients to atrial fibrillation after coronary artery bypass grafting. Thorac Cardiovasc Surg. 1998;46:115–120. doi: 10.1055/s-2007-1010206. [DOI] [PubMed] [Google Scholar]
- 13.Pathik B, Lee G, Sacher F, Haïssaguerre M, Jaïs P, Massoullié G, Derval N, Sanders P, Kistler P, Kalman JM. Epicardial-endocardial breakthrough during stable atrial macroreentry: Evidence from ultra-high-resolution 3-dimensional mapping. Heart Rhythm. 2017;14:1200–1207. doi: 10.1016/j.hrthm.2017.04.043. [DOI] [PubMed] [Google Scholar]
- 14.Allessie MA, de Groot NMS, Houben RPM, Schotten U, Boersma E, Smeets JL, Crijns HJ. Electropathological substrate of long-standing persistent atrial fibrillation in patients with structural heart disease: longitudinal dissociation. Circ Arrhythm Electrophysiol. 2010;3:606–615. doi: 10.1161/CIRCEP.109.910125. [DOI] [PubMed] [Google Scholar]
- 15.de Groot NMS, Houben RPM, Smeets JL, Boersma E, Schotten U, Schalij MJ, Crijns H, Allessie MA. Electropathological substrate of longstanding persistent atrial fibrillation in patients with structural heart disease: epicardial breakthrough. Circulation. 2010;122:1674–1682. doi: 10.1161/CIRCULATIONAHA.109.910901. [DOI] [PubMed] [Google Scholar]
- 16.Melby SJ, George JF, Picone DJ, Wallace JP, Davies JE, George DJ, Kirklin JK. A time-related parametric risk factor analysis for postoperative atrial fibrillation after heart surgery. J Thorac Cardiovasc Surg. 2015;149:886–892. doi: 10.1016/j.jtcvs.2014.11.032. [DOI] [PubMed] [Google Scholar]
- 17.Walters TE, Lee G, Spence S, Larobina M, Atkinson V, Antippa P, Goldblatt J, O’Keefe M, Sanders P, Kistler PM, Kalman JM. Acute atrial stretch results in conduction slowing and complex signals at the pulmonary vein to left atrial junction: insights into the mechanism of pulmonary vein arrhythmogenesis. Circ Arrhythm Electrophysiol. 2014;7:1189–1197. doi: 10.1161/CIRCEP.114.001894. [DOI] [PubMed] [Google Scholar]
- 18.Rolf S, Kircher S, Arya A, Eitel C, Sommer P, Richter S, Gaspar T, Bollmann A, Altmann D, Piedra C, Hindricks G, Piorkowski C. Tailored atrial substrate modification based on low-voltage areas in catheter ablation of atrial fibrillation. Circ Arrhythm Electrophysiol. 2014;7:825–833. doi: 10.1161/CIRCEP.113.001251. [DOI] [PubMed] [Google Scholar]
- 19.Jadidi AS, Lehrmann H, Keyl C, Sorrel J, Markstein V, Minners J, Park C-I, Denis A, Jaïs P, Hocini M, Potocnik C, Allgeier J, Hochholzer W, Herrera-Sidloky C, Kim S, Omri YE, Neumann F-J, Weber R, Haïssaguerre M, Arentz T. Ablation of Persistent Atrial Fibrillation Targeting Low-Voltage Areas With Selective Activation Characteristics. Circ Arrhythm Electrophysiol. 2016;9:e002962. doi: 10.1161/CIRCEP.115.002962. [DOI] [PubMed] [Google Scholar]
- 20.Jalife J, Berenfeld O, Mansour M. Mother rotors and fibrillatory conduction: a mechanism of atrial fibrillation. Cardiovasc Res. 2002;54:204–216. doi: 10.1016/s0008-6363(02)00223-7. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.