

Abstract
Supplemental Digital Content is available in the text.
BACKGROUND
The standard procedure for the management of skeletal class III malocclusion is maxillary advancement with mandibular setback. Many Asian people have a preexisting dentoalveolar protrusion and a flat facial profile with a prominent mandibular angle compared with Western people. Maxillary advancement and mandible setback procedures may aggravate this preexisting dentoalveolar protrusion. Thus, in our practice, we use maxillary posterior impaction without maxillary advancement and mandibular setback to treat our Asian class III patients.1,2
METHODS
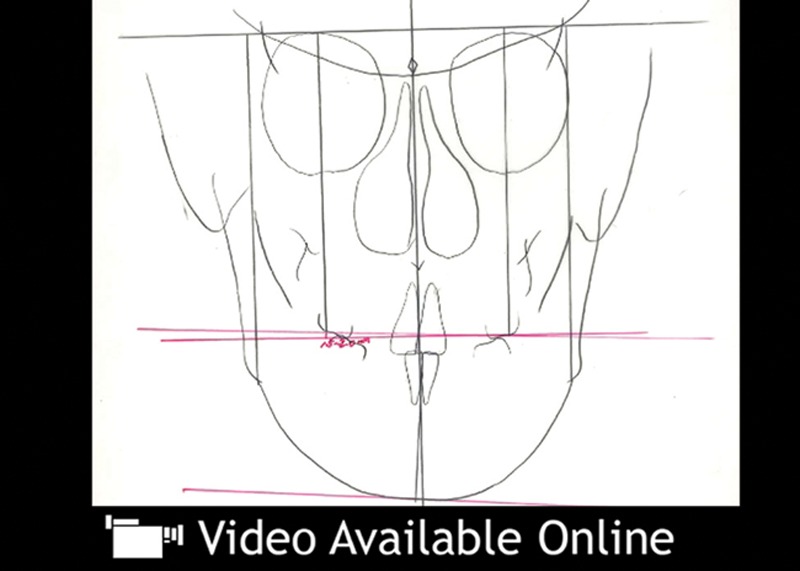
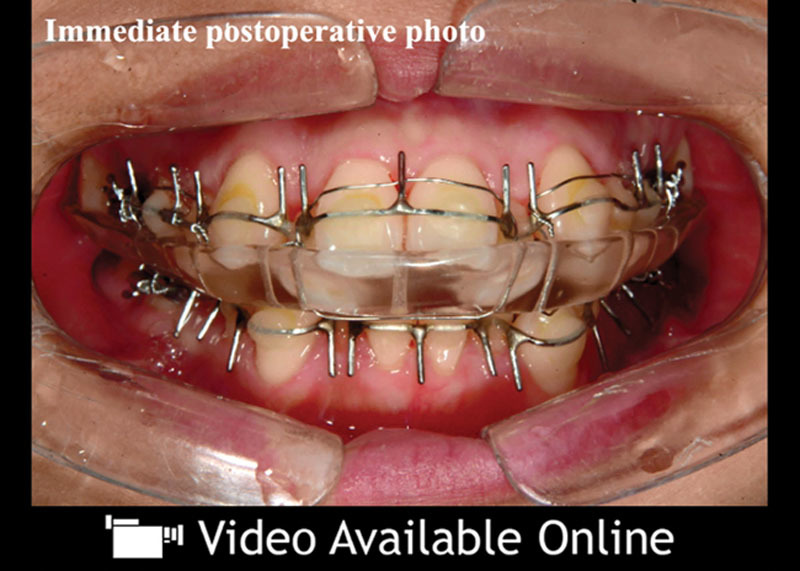
A 22-year-old patient presented with a typical skeletal class III dentofacial deformity (see video, Supplemental Digital Content 1, which displays the preoperative analysis. This video is available in the “Related Videos” section of the Full-Text article on PRSGlobalOpen.com or available at http://links.lww.com/PRSGO/A588). For aesthetic reasons, we chose to treat this patient using maxillary posterior impaction without maxillary advancement and mandibular setback based on the surgery-first orthognathic approach without presurgical orthodontic treatment.3,4 The patient was followed up for a period of 60 months. The preoperative surgical treatment objective (STO) was different from that of the conventional Western STO. As the triangle that consists of the anterior nasal spine, posterior nasal spine, and pogonion could have an effect on facial aesthetics even in the same occlusion, clockwise rotation of the maxillomandibular complex accompanied by occlusal restoration in class III dentofacial deformity was thought to be a solution for this patient. Although the surgical technique is similar with the exception of the direction of maxillary movement and the amount of mandibular setback, the aesthetics and functional occlusion are very different. Herein, we present the whole process of the clockwise rotational orthognathic surgery optimized for the Asian class III dentofacial deformity, based on the surgery-first orthognathic approach (see video, Supplemental Digital Content 2, which displays the intraoperative video from incision to maxillary fixation. This video is available in the “Related Videos” section of the Full-Text article on PRSGlobalOpen.com or available at http://links.lww.com/PRSGO/A589; see video, Supplemental Digital Content 3, which displays the intraoperative video from mandible fixation to mucosal closure. This video is available in the “Related Videos” section of the Full-Text article on PRSGlobalOpen.com or available at http://links.lww.com/PRSGO/A590).
Video Graphic 1.
See video, Supplemental Digital Content 1, which displays the preoperative analysis. This video is available in the “Related Videos” section of the Full-Text article on PRSGlobalOpen.com or available at http://links.lww.com/PRSGO/A588.
Video Graphic 2.

See video, Supplemental Digital Content 2, which displays the intraoperative video from incision to maxillary fixation. This video is available in the “Related Videos” section of the Full-Text article on PRSGlobalOpen.com or available at http://links.lww.com/PRSGO/A589.
Video Graphic 3.

See video, Supplemental Digital Content 3, which displays the intraoperative video from mandible fixation to mucosal closure. This video is available in the “Related Videos” section of the Full-Text article on PRSGlobalOpen.com or available at http://links.lww.com/PRSGO/A590.
RESULTS
Analysis using 2D cephalometry revealed that the average palatal plane angle of the study patient was more flat than that of average Asian skeletal class III patients. Images taken with a 3D camera revealed that the change in soft-tissue landmarks in the frontal view and the outcome in facial aesthetics in this procedure were remarkably more acceptable in Asian skeletal class III patients compared with the standard procedures.5 Moreover, despite the large amount of maxillary posterior impactions, there was no postoperative functional change in the airway. The occlusal plane based on the Frankfort horizontal line changed from 80 to 70 degrees. Although the sella–nasion–A point angle was maintained, the sella–nasion–B point angle decreased from 85 to 75 degrees. The class III malocclusion with dental crowding was corrected, resulting in a normal occlusion with normal arch coordination (see video, Supplemental Digital Content 4, which displays the postoperative results. This video is available in the “Related Videos” section of the Full-Text article on PRSGlobalOpen.com or available at http://links.lww.com/PRSGO/A591).
Video Graphic 4.
See video, Supplemental Digital Content 4, which displays the postoperative results. This video is available in the “Related Videos” section of the Full-Text article on PRSGlobalOpen.com or available at http://links.lww.com/PRSGO/A591.
CONCLUSIONS
Maxillary posterior impaction without maxillary advancement and mandibular setback based on the surgery-first orthognathic approach seems to be a suitable treatment for Asian skeletal class III patients in that it minimized the aggravation of the dentoalveolar protrusion and postoperative alar widening as well as the total treatment time. The STO should be planned according to the individual patients. Maxillary posterior impaction without advancement may yield better results than maxillary advancement, especially in terms of aesthetic outcomes of Asian class III patients, as was revealed in this case.
Supplementary Material
Footnotes
Disclosure: The authors have no financial interest to declare in relation to the content of this article. The Article Processing Charge was paid for by the authors.
Supplemental digital content is available for this article. Clickable URL citations appear in the text.
REFERENCES
- 1.Choi JW, Lee JY, Yang SJ, et al. The reliability of a surgery-first orthognathic approach without presurgical orthodontic treatment for skeletal class III dentofacial deformity. Ann Plast Surg. 2015;74:333–341.. [DOI] [PubMed] [Google Scholar]
- 2.Choi JW, Park YJ, Lee CY. Posterior pharyngeal airway in clockwise rotation of maxillomandibular complex using surgery-first orthognathic approach. Plast Reconstr Surg Glob Open. 2015;3:e485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Jeong WS, Choi JW, Kim DY, et al. Can a surgery-first orthognathic approach reduce the total treatment time? Int J Oral Maxillofac Surg 2017;4:473–482.. [DOI] [PubMed] [Google Scholar]
- 4.Choi SH, Yoo HJ, Lee JY, et al. Stability of pre-orthodontic orthognathic surgery depending on mandibular surgical techniques: SSRO vs IVRO. J Craniomaxillofac Surg. 2016;44:1209–1215.. [DOI] [PubMed] [Google Scholar]
- 5.Choi JW, Lee JY, Oh TS, et al. Frontal soft tissue analysis using a 3 dimensional camera following two-jaw rotational orthognathic surgery in skeletal class III patients. J Craniomaxillofac Surg. 2014;42:220–226.. [DOI] [PubMed] [Google Scholar]