

Abstract
The assessment of cognitive function is a challenging yet an integral component of psychological, psychiatric, and neurological evaluation. Cognitive assessment tools either can be administered quickly for screening for neurocognitive disorders or can be comprehensive and detailed to identify cognitive deficits for the purpose of localization, diagnosis, and rehabilitation. This article is a comprehensive review of published research that discusses the current challenges for cognitive testing in India, available tools used for the assessment of cognitive function in India, and future directions for cognitive testing in India.
Keywords: Cognition, cognitive testing, India, neuropsychology
INTRODUCTION
Assessment of cognitive function is a challenging yet an integral component of psychological, psychiatric, and neurological evaluation. Cognitive assessment is used for screening for the presence of any cognitive impairment and differential diagnosis, determining the severity of the disorder, monitoring disease progression, and determining treatment efficacy.
It is mandatory to use relevant normative data to understand the cognitive status of an individual and derive empirical conclusions that are strongly based on well-understood theoretical rationales of psychometrics and neuroscience. Ever since, it was understood that populations differing in their demographic characters show difference in test performance; population-based normative studies have become the need of the hour. Unfortunately, even seemingly homogenous populations exhibit within-group differences, and thus, the task of developing and using theoretically and ecologically valid instruments for the empirical assessment of cognitive function in a known heterogeneous population as in India is proving to be an enormous challenge for researchers and clinicians. The Indian demographics does not just differ by language and religion but also by a myriad of cultural and socioeconomic confounding factors, some of which have not yet even been identified as possible confounders.
In India, the cognitive assessment in human clinical populations is mainly carried out by professionals with Masters', M. Phil., or Doctoral-level training in psychology and its allied fields such as school psychology, clinical psychology, or counseling psychology and doctors with MD-level training in general medicine and psychiatry or DM-level training in neurology. Due to the lack of proper licensing procedures, dearth of good assessment tools and protocols, lack of uniform training practices, increasing need for cognitive testing, and shortage of trained professionals, the empirical assessment of cognition is often replaced by brief nonstandardized screening by clinicians whose observation-based subjective opinions take precedence over evidence-based objectively derived conclusions about a patient's cognitive status.
CHALLENGES
It is well known that education plays an important role in determining test performance of subjects on tests of cognition. The unavailability of quality educational opportunities to a significant proportion of the Indian population coupled with different categories of schools,[1] curricula,[1] and lack of uniform assessment of educational achievement makes it challenging to accurately determine the literacy, educational attainment, and cognitive ability of an individual. Further, added to this is the possibility of achieving passing grades and higher education in India using favors within the educational system. Many children with intellectual disabilities or neurodevelopmental disabilities go through formal education undetected due to the lack of systematic assessment and resources and tolerance for “poor learners” in the different Indian schooling systems.[1] Hence, this gives us a heterogeneous population even when the level of educational attainment is controlled, and so, education stratified normative data for cognitive tests may not be accurately available. The absence of any baseline data for estimating premorbid level of cognitive function and the inability to use the highest level of educational attainment as a reliable estimate make screening of cognitive dysfunction and diagnosis challenging.
When the classic Tower of Hanoi, a popular test of planning skills and executive function was administered to two groups of cognitively normal Indian elderly and those with early Alzheimer's disease, and it was found that the test had poor discriminative validity. In addition, it was found that the Indian cognitively normal elderly performed worse than age-matched scores in other studies though the Indian sample had more years of formal education.[2] Clinicians in India commonly observe this type of inferior test performance by individuals despite having high levels of educational attainment. This may be attributed to functional illiteracy in school-level educated elders whose reading, writing, drawing, and arithmetic skills acquired in school fall into disuse and become redundant due to their lifestyles or occupations.
There is a lack of exposure to take psychological tests, and often, the tests of cognition are treated akin to testing in schools and this leads to test anxiety which in turn affects test performance. Often, subjects who subjectively think they might perform very well on the tests are unwilling to try tasks that involve drawing, verbal recall, etc., with the best effort as there is an innate societal pressure of “scoring the highest” and “being the best.” The elderly Indian population and their families are defensive about their cognitive abilities and frequently are not motivated enough to complete the testing, often giving up during testing.[3] Thus, determining the best level of cognitive functioning is challenging even in cognitively normal people, and often, the poor test performance may be due to this lack of test sophistication and not cognitive dysfunction. It has been observed repeatedly by many clinicians that there is a need to repeat test instructions and give lengthy explanations to subjects and verbatim test instructions alone are not sufficient in many cases.[3,4] This affects the standardization of tests, and hence, test developers need to build sufficient flexibility into the test administration instructions. Further, it has been noted that instructions often need to be modified to suit colloquially used syntax and vocabulary. Elderly subjects have also been observed to require constant approval and urging from the tester to complete tasks.
India has no single national language, and at present, there are 22 official languages recognized in India. As per the Census of India of 2001, India has 122 major languages and 1599 other languages, many of which are dialects with no written script.[5] Although most trained professionals are multilingual or at the least bilingual, often they need to rely on translators to administer and interpret the tests. Many a times, professional translators for some languages are not available at hand easily and family members or friends of the patient's need to step in. This greatly affects the empirical, standardized nature of the testing process. In addition, frequently, tools are unavailable in the language that a patient is comfortable in. In these scenarios, the tester must translate an existing test while testing.[6] Apart from this, each language has its own variations in syntax and vocabulary based on the region of the country it is spoken in. Thus, the huge number of considerations and their implications that a test developer must take into account complicates the entire process of adaptation and development of assessment tools, which has resulted in very few cognitive tests available for use in India and no tests available for some communities within India.
Despite making rapid strides in raising awareness about dementia, an understanding of what is normal aging and what is not is found wanting even among the urban, educated population. Often, organic brain conditions are taken as anticipated normal aging.[7] The stigma, caregiver effort, and embarrassment attached to the behavioral symptoms of dementia cause these symptoms to be taken as deliberate misbehavior. Due to the lack of access to any organized medical care systems for a considerable proportion of population, even basic healthcare is overlooked. In cases of neurocognitive ailments, there is an even bigger gap between the medical requirements of this population, their diagnosis, and appropriate management.[7] When this population accesses healthcare for other physical comorbidities, the patient is often at advanced stages of the disease and cannot benefit from the current advances in the management of neurocognitive ailments. It is for this same population that the availability of normative data is scarce.
The caregiver report of the level of cognitive functioning of an individual is often ambiguous, especially when the patient is the head of the household and is a male.[7] This can be attributed to the traditional patriarchal structure of families in India and the culture of respect toward elders and spouses. Approximately, about 25% of the family members of a patient do not recognize any memory impairment.[3] This may be due to the high levels of support given to elders in the family and society to perform their social roles and activities of daily living.[7] Caregivers were found to be less likely to report any cognitive decline or social impairment even when there is objective memory impairment as seen on tests of cognitive function.[7] This may be due to the interpretation of early signs of dementia as decline in functioning due to normal aging. Thus, most often, even reversible dementias are neglected for appropriate medical management and the patients receive health-care attention only in the advanced stages of the established disease process. Patients are frequently lost to follow-up and consequently do not receive long-term treatment.[8]
There is a general lack of awareness of the benefits of cognitive testing, cognitive training, and rehabilitation, as well as the role of testing in early diagnosis. As a result of this, there is a devaluation of the testing which patients and caregivers often consider as long, time-consuming, unnecessary, and expensive without any immediate benefit of a medical cure.[3,6] The stigma surrounding the disease coupled with the lack of team-based approach to disease management and integrated health systems in India often leads to patients ignoring the recommendation to get themselves assessed. This emphasizes the need for brief but sensitive cognitive assessment tools.
There is a decreased priority for research in the field of cognitive assessment in India due to the scarcity of trained scientist-practitioners who are hard pressed for time, financial resources, infrastructure, and workforce required for carrying out and reporting quality work.[8] Often, these constraints on resources and lack of uniform training prevent the professionals from documenting, publishing, and sharing their work, which sometimes include cognitive tests that they have developed in their clinics for their target patient communities. Adequate training with updated curriculum and supervision should be made mandatory for improving the quality of clinical care and research output.
GLOBAL SCREENING MEASURES
Mini mental state examination[9]
The Mini mental state examination (MMSE)[9] is the most commonly used brief global cognitive screen by Indian clinicians in the outpatient department as well as at the bedside. The MMSE is a pencil-and-paper test that has a maximum score of 30, in which severe cognitive problems are indicated by lower scores. The cutoff score used for detecting cognitive dysfunction on the MMSE is 24. It was popularly used for research as well before the copyright enforcement by PAR curbed its use. It continues to be used for obtaining a standard index of cognitive dysfunction severity that is easily understood by clinicians across the spectrum of neurocognitive disorders' management though it has been proven to have low sensitivity and specificity,[10] especially when used in mild or early disease conditions, thus overestimating cognitive impairment.[11]
Hindi mental state examination[12]
The Hindi mental state examination (HMSE)[12] is the translation and adaptation of the MMSE for screening the Hindi-speaking illiterate rural elderly population. The maximum score if all items are answered correctly is 30 like the MMSE. It is freely available.
Montreal cognitive assessment (MoCA)[13]
The Montreal cognitive assessment (MoCA)[13] is a freely available, brief, simple to administer global cognitive screening tool, which is becoming increasingly popular due to its availability across multiple global languages including the Indian languages of Bengali, Kannada, Malayalam, Marathi, Tamil, Telugu, Hindi, and Urdu.[14] It has been validated for use in Malayalam-speaking Parkinson's disease patients.[15] The maximum score is 30 and it has provisions for correcting the score for low levels of education, visual impairments, and physical disability. It has good test-retest reliability for repeated assessments. The cutoff score used for distinguishing normal subjects from mild cognitive impairment is 26. The MoCA has shown better sensitivity and specificity when compared with the MMSE. The computerized version of the test is under development.[16]
Addenbrooke's cognitive examination-III[17]
The Addenbrooke's cognitive examination-III[17] is a 100-point simple, brief paper- and pencil-based measure of global cognitive function that can be used at the bedside. It is available in many global languages including Tamil, Hindi, Indian English, Kannada, Telugu, Urdu, and Marathi. This test is freely available with cutoff scores of 88 and 82 used, respectively, for clinical and research use.[18] Although the Addenbrooke's cognitive examination (ACE) was formerly available in some other Indian languages such as Bengali and Malayalam (known as M-ACE with established population-derived norms for an urban Malayalam-speaking population[19]), they are adaptations of the ACE-R which is no longer in use in clinical and research settings and have been removed from the NeuRA Research Institute's website.[18]
Community screening instrument for dementia[20]
The Community Screening Instrument for Dementia (CSI-D)[20] is a cognitive screening tool that forms a part of the 10/66 study batteries of tests as the measure of global cognitive function.[21] It is a 32-item cognitive test which is used to generate a global cognitive score. It also includes a 26-item informant interview about the patient's daily functioning and general health and combines this into a single predictive algorithm.[22] A brief, abbreviated version of the community screening instrument for dementia (CSI-D) has also been developed for use in primary care settings by nonspecialist health workers.[22]
Kolkata cognitive screening[23]
The Kolkata cognitive screening[23] is a global cognitive screening battery which has established normative data for the population of the city of Kolkata. The test language used is Bengali. The translated test battery is freely available in the public domain.
World health organization's Study on AGEing and adult health survey[24]
The World Health Organization's Study on AGEing and adult health survey[24] is a culture-sensitive screening tool that was developed as part of the World health organization's Study on AGEing and adult health (SAGE), a household health survey carried out in Ghana, India, and Tanzania. The pilot study includes the normative data from 469 Indian adults for the word list learning test, category fluency (animals), and digit span (forward and backward). The cognitive tests used in SAGE and data are freely available.
Cognistat-Indian adaptation[25]
Cognistat, formerly known as the neurobehavioral cognitive status examination, is a brief cognitive screening tool that has been adapted for use in the Indian population and has shown good validity for use in patients with traumatic brain injury.[25] Although it has shown good reliability and validity in a small size, population-derived normative data have not yet been established. It is unclear whether the Indian adaptation is available for purchase yet from the publishers of the test as their website does not list it as a purchase option.[26]
Multi-domain cognitive screening test[27]
The multi-domain cognitive screening test (MDCST)[27] is a sensitive and easy to administer global cognitive screening tool developed for detection of early MCI and has shown good psychometric properties for further use in demographic studies. It has been validated for use in the population of acclimatized lowlanders staying at altitudes higher than 4300 m.
Dementia assessment by rapid test[28]
The dementia assessment by rapid test (DART)[28] consists of four test items (repetition of three words, category fluency (vegetables), recall of words, and clock drawing) and is scored on range of scores from 0 to 4. It has been shown to have good sensitivity and concurrent validity but low specificity when compared to the MMSE. This quick screening test is available on public domain.
Hindi adaptation of Mattis dementia rating scale[29]
The Hindi adaptation of Mattis Dementia rating scale[29] consists of 36 tasks divided into five components, with a maximum score of 144. It has shown good reliability and validity for evaluation of dementia in Hindi-speaking Indian population.
Rowland universal dementia assessment scale[30]
The Rowland Universal dementia assessment tool was validated for use in the Malayalam-speaking population.[30] It has a maximum score of 30 and the cutoff score used was 23. Rowland universal dementia assessment scale (RUDAS) was found to have similar sensitivity but better specificity when compared to the Malayalam MMSE.
Picture-based memory impairment screen[31]
The Picture-based memory impairment screen[31] is a culture-fair, picture-based cognitive screen designed to be administered by nonspecialists. It is a quick and reliable screen that can be administered in 4 min. It has been developed to use in older adults aged 55 or older with little or no education and shows good reliability and validity. In this test, 12 digital photographs are sorted in three sets of four pictures each. Any one set of pictures is shown to the subject who must recall as many photographs as possible after an interference task. If the subject cannot retrieve by free recall, category cues are given and scored accordingly.
Domain-wise tests available with Indian norms [Table 1]
Table 1.
Tests available with Indian norms for testing specific cognitive domains
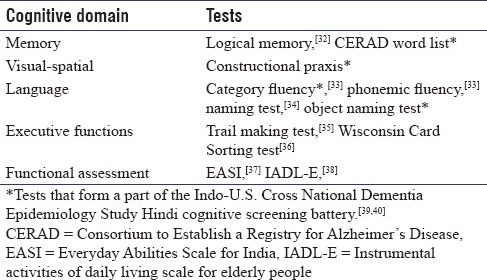
Speech and language pathologists often do the comprehensive assessment of language function in the clinical setting. Aphasia test batteries such as the Indian Aphasia Battery[41] and Western Aphasia Battery with Indian norms[42] are available for testing the Indian population. The Bilingual Aphasia Test battery has versions in Hindi, Kannada, Oriya, Tamil, and Urdu,[43] which can be used for assessing native speakers of those languages in India, but population-derived norms have not been established for the test battery in each of these languages.
Batteries developed and standardized for Indian population
PGI battery of brain dysfunction[44]
The PGI Battery of brain dysfunction[44] consists of five sub tests – PGI memory scale, Bhatia's Short Scale, Verbal adult intelligence scale, Nahor-Benson test of Perceptual Acuity, and Bender Visual Motor Gestalt Test. This test battery gives a global measure of cognitive dysfunction based on 19 test variables. It has established norms for the age group 20–59 years and was developed in 1990.
PGI memory scale[45]
The PGI memory scale[45] has 10 subtests assessing verbal and nonverbal memory, remote memory, recent memory, short-term memory, and long-term memory. The test was developed at Postgraduate Institute of Medical Education and Research, Chandigarh. It has been standardized with norms for adults between 20 and 45 years.
NIMHANS neuropsychological battery[46]
The NIMHANS neuropsychological battery[46] is the earliest neuropsychological test battery developed in India. It is a lobe function test battery based on Luria's principles of cerebral localization and lateralization of higher mental functions. It has about 20 tests with several adapted western tests and an indigenous delayed response test to assess working memory.[6]
NIMHANS neuropsychological battery for adults[47]
The NIMHANS Neuropsychological battery for adults[47] consists of 19 widely used western neuropsychological tests that have been adapted and standardized for the Indian population. It has population-derived norms for ages 16–65 years and has been validated for use in many neurocognitive disorders.
NIMHANS neuropsychological battery for children[48]
The NIMHANS neuropsychological battery for children[48] has norms for ages 5–15 years and has been validated for use in brain injured children.
NIMHANS neuropsychological battery for elderly[49]
The NIMHANS neuropsychological battery for elderly (NNB-E)[49] is a comprehensive test battery developed for use in the Indian elderly between the ages 55–80 years. It has shown to have good discriminant validity to identify older adults with Alzheimer's dementia.
All India Institute of Medical Sciences comprehensive neuropsychological battery in Hindi (adult form)[50]
The All India Institute of Medical Sciences comprehensive neuropsychological battery in Hindi (adult form)[50] is a comprehensive battery of tests which is normed for ages between 15–80 years. It is based on the Luria-Nebraska Neuropsychological Battery. It consists of 160 items divided into ten basic scales and four secondary scales. It is the only indigenously developed Indian test battery in Hindi.
10/66 Dementia Research Group cognitive test battery[51]
The 10/66 Dementia Research Group cognitive test battery[51] was used in the 10/66 Dementia Research Group studies comprising tests of general cognitive function, verbal fluency, and immediate and delayed verbal recall. It has been developed from the Community Screening Instrument for Dementia (CSI 'D') and the Consortium to Establish a Registry for Alzheimer's Disease. It has site-specific norms for ages 65–80 years. It is a useful battery for cross-cultural research as it has normed the same battery across seven countries (Cuba, Dominican Republic, Venezuela, Peru, Mexico, China, and India).
HIV cognitive test battery[52]
The HIV cognitive test battery[52] was developed to assess the cognitive domains that are known to be vulnerable to the effect of HIV. It consists of tests used in the United States that were modified for assessment in Tamil and Telugu. Population-derived norms have not been established for this battery.
Commercially available test batteries
Test batteries for assessment of general intellectual ability such as Wechsler Intelligence Scale for Children–Fourth Edition, India, and Wechsler Adult Intelligence Scale–Fourth Edition, India, which are used globally as gold standard assessments, are now available from publishers with Indian population specific adaptation, standardization, and norms. The Wechsler Memory Scale–Third Edition, India, which can assess verbal and nonverbal learning and memory, is also available from the publishers and is used across India. Recently, Wechsler Abbreviated Scale of Intelligence, Second Edition, India, has been available from the publisher as a brief and reliable measure of cognitive ability.[53] Some of the tests in the test batteries and their relevant norms can be used as standalone tests in clinical and research settings making them valuable for a comprehensive cognitive assessment; however, considering their cost of purchase, they are more commonly used only in bigger academic and medical institutions by clinical psychologists/neuropsychologists.
CNS Vital Signs is a comprehensive computerized neuropsychological test battery which is available in many global languages including the Indian languages of Bengali, Gujarati, Hindi, Kannada, Malayalam, Marathi, Punjabi, Tamil, Telugu, and Urdu. It consists of 10 tests that have been normed, but it is unclear whether any Indian population-derived norms are available.[54]
CONCLUSIONS AND FUTURE DIRECTIONS
Despite over 100 years of psychology, over 75 years of neurology, and over 40 years of neuropsychology in India, cognitive testing is still in its infancy. The priority for the advancement of cognitive testing lies in the development of novel assessment tools for our population, adapting appropriate tests that were developed for other populations and establishing population norms. Multicenter studies focusing on the development of tests in multiple languages which are tested for equivalence will solve the need for a pan Indian cognitive assessment tool. Capacity assessments with ecological validity and performance/symptom validity tests are in need. Although computer-assisted administration is not yet a feasible solution in India due to the lack of infrastructure and limited computing ability of the people (30.2% in urban areas and 8.8% in rural areas[55]), it holds promise for the development of equivalent cognitive assessment tools across the various local languages which can assess cognition with precision and reliability. The computer-aided administration will also promote better standardization of the tools and facilitate faster scoring and detailed analytics which will be necessary to address the needs of the growing Indian population despite the shortage of trained professionals. The development of a common assessment tool for the Indian population across languages has become a global need due to the increasing Indian diaspora across the world. Quality collaborative research coupled with an increase in sharing of resources and research findings will help in bridging the gap between the demand for brief, sensitive, and specific cognitive tests with strong psychometric properties and maintaining the empirical nature of cognitive testing for accurate diagnosis, management, and research.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Basu J. Present status and challenges of intellectual assessment in India. Int J School Educ Psychol. 2016;4:231–40. [Google Scholar]
- 2.Balachandar R, Tripathi R, Bharath S, Kumar K. Classic Tower of Hanoi, planning skills, and the Indian elderly. East Asian Arch Psychiatry. 2015;25:108–14. [PubMed] [Google Scholar]
- 3.Shah U. Neuropsychological assessment in the Indian elderly. Indian J Private Psychiatry. 2009;3:59–66. [Google Scholar]
- 4.Chandra V, Ganguli M, Ratcliff G, Pandav R, Sharma S, Belle S, et al. Practical issues in cognitive screening of elderly illiterate populations in developing countries. The Indo-US Cross National Dementia Epidemiology Study. Aging Clin Exp Res. 1998;10:349–57. doi: 10.1007/BF03339881. [DOI] [PubMed] [Google Scholar]
- 5.Census of India. [Last retrieved on 2016 Dec 15]. Available from: http://www.censusindia.gov.in/Census_Data_2001/Census_Data_Online/Language/gen_note.html .
- 6.Kumar JK, Sadasivan A. Neuropsychology in India. Clin Neuropsychol. 2016;30:1252–66. doi: 10.1080/13854046.2016.1197314. [DOI] [PubMed] [Google Scholar]
- 7.Prince MJ. The 10/66 dementia research group-10 years on. Indian J Psychiatry. 2009;51(Suppl 1):S8–15. [PMC free article] [PubMed] [Google Scholar]
- 8.Mathew R, Mathuranath PS. Issues in evaluation of cognition in the elderly in developing countries. Ann Indian Acad Neurol. 2008;11:82–8. doi: 10.4103/0972-2327.41874. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12:189–98. doi: 10.1016/0022-3956(75)90026-6. [DOI] [PubMed] [Google Scholar]
- 10.Creavin ST, Wisniewski S, Noel-Storr AH, Trevelyan CM, Hampton T, Rayment D, et al. Mini-Mental State Examination (MMSE) for the detection of dementia in clinically unevaluated people aged 65 and over in community and primary care populations. Cochrane Database Syst Rev. 2016:CD011145. doi: 10.1002/14651858.CD011145.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kuriakose J, Shaji S. Barriers to the cognitive assessment of dementia in India. Alzheimer's Dement. 2012;8:P227. [Google Scholar]
- 12.Ganguli M, Ratcliff G, Chandra V, Sharma S, Gilby J, Pandav R, et al. A Hindi version of the MMSE: The development of a cognitive screening instrument for a largely illiterate elderly population in India. Int J Geriatr Psychiatry. 1995;10:367–77. [Google Scholar]
- 13.Nasreddine ZS, Phillips NA, Bédirian V, Charbonneau S, Whitehead V, Collin I, et al. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53:695–9. doi: 10.1111/j.1532-5415.2005.53221.x. [DOI] [PubMed] [Google Scholar]
- 14. [Last retrieved on 2016 Dec 15]. Available from: http://www.mocatest.org/paper-tests/moca-test-full/
- 15.Krishnan S, Justus S, Meluveettil R, Menon RN, Sarma SP, Kishore A. Validity of Montreal Cognitive Assessment in non-english speaking patients with Parkinson's disease. Neurol India. 2015;63:63–7. doi: 10.4103/0028-3886.152637. [DOI] [PubMed] [Google Scholar]
- 16. [Last retrieved on 2017 Mar 05]. Available from: http://www.mocatest.org/normative-data/
- 17.Mathuranath PS, Nestor PJ, Berrios GE, Rakowicz W, Hodges JR. A brief cognitive test battery to differentiate Alzheimer's disease and frontotemporal dementia. Neurology. 2000;55:1613–20. doi: 10.1212/01.wnl.0000434309.85312.19. [DOI] [PubMed] [Google Scholar]
- 18. [Last retrieved on 2017 May 09]. Available from: https://www.neura.edu.au/
- 19.Mathuranath PS, Cherian JP, Mathew R, George A, Alexander A, Sarma SP. Mini mental state examination and the Addenbrooke's cognitive examination: Effect of education and norms for a multicultural population. Neurol India. 2007;55:106–10. doi: 10.4103/0028-3886.32779. [DOI] [PubMed] [Google Scholar]
- 20.Hall KS, Hendrie HC, Brittain HM, Norton JA, Jr, Rodgers DD, Prince CS, et al. The development of a dementia screening interview in two distinct languages. Int J Methods Psychiatr Res. 1993;3:1–28. [Google Scholar]
- 21.Sosa AL, Albanese E, Prince M, Acosta D, Ferri CP, Guerra M, et al. Population normative data for the 10/66 Dementia Research Group cognitive test battery from Latin America, India and China: A cross-sectional survey. BMC Neurol. 2009;9:48. doi: 10.1186/1471-2377-9-48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Prince M, Acosta D, Ferri CP, Guerra M, Huang Y, Jacob KS, et al. A brief dementia screener suitable for use by non-specialists in resource poor settings – the cross-cultural derivation and validation of the brief Community Screening Instrument for Dementia. Int J Geriatr Psychiatry. 2011;26:899–907. doi: 10.1002/gps.2622. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Das SK, Banerjee TK, Mukherjee CS, Bose P, Biswas A, Hazra A, et al. An urban community-based study of cognitive function among non-demented elderly population in India. Neurol Asia. 2006;11:37–48. [Google Scholar]
- 24.Carroll BA, Kowal P, Naidoo N, Chatterji S. Geneva: World Health Organization; 2012. [Last retrieved on 2017 Mar 12]. Measuring Cognitive Status In Older Age In Lower Income Countries: Results From a Pilot of the Study on Global AGEing and Adult Health (SAGE). SAGE Working Paper No. 3. Available from: http://www.who.int/entity/healthinfo/sage/SAGEWorkingPaper3_Pilot_cognition_Nov12.pdf . [Google Scholar]
- 25.Gupta A, Kumar NK. Indian adaptation of the Cognistat: Psychometric properties of a cognitive screening tool for patients of traumatic brain injury. Indian J Neurotrauma. 2009;6:123–32. [Google Scholar]
- 26. [Last retrieved on 2017 Mar 12]. Available from: http://www.cognistat.com/
- 27.Hota SK, Sharma VK, Hota K, Das S, Dhar P, Mahapatra BB, et al. Multi-domain cognitive screening test for neuropsychological assessment for cognitive decline in acclimatized lowlanders staying at high altitude. Indian J Med Res. 2012;136:411–20. [PMC free article] [PubMed] [Google Scholar]
- 28.Swati B, Sreenivas V, Manjari T, Nehra A. Dementia Assessment By Rapid Test (DART): An Indian screening tool for dementia. J Alzheimers Dis Parkinsonism. 2015;5:198. [Google Scholar]
- 29.Gopaljee S, Dwivedi CB, Pandey R. Psychometric evaluation of the Hindi adaptation of Mattis Dementia Rating Scale (HMDRS) Indian J Soc Sci Res. 2011;9:82–90. [Google Scholar]
- 30.Iype T, Ajitha BK, Antony P, Ajeeth NB, Job S, Shaji KS. Usefulness of the Rowland Universal Dementia Assessment scale in South India. J Neurol Neurosurg Psychiatry. 2006;77:513–4. doi: 10.1136/jnnp.2005.069005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Verghese J, Noone ML, Johnson B, Ambrose AF, Wang C, Buschke H, et al. Picture-based memory impairment screen for dementia. J Am Geriatr Soc. 2012;60:2116–20. doi: 10.1111/j.1532-5415.2012.04191.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Andrade C, Madhavan AP, Kishore ML. Testing logical memory using a complex passage: Development and standardization of a new test. Indian J Psychiatry. 2001;43:252–6. [PMC free article] [PubMed] [Google Scholar]
- 33.Mathuranath PS, George A, Cherian PJ, Alexander A, Sarma SG, Sarma PS. Effects of age, education and gender on verbal fluency. J Clin Exp Neuropsychol. 2003;25:1057–64. doi: 10.1076/jcen.25.8.1057.16736. [DOI] [PubMed] [Google Scholar]
- 34.George A, Mathuranath PS. Community-based naming agreement, familiarity, image agreement and visual complexity ratings among adult Indians. Ann Indian Acad Neurol. 2007;10:92–9. [Google Scholar]
- 35.Bhatia T, Shriharsh V, Adlakha S, Bisht V, Garg K, Deshpande SN. The trail making test in India. Indian J Psychiatry. 2007;49:113–6. doi: 10.4103/0019-5545.33258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Kohli A, Kaur M. Wisconsin card sorting test: Normative data and experience. Indian J Psychiatry. 2006;48:181–4. doi: 10.4103/0019-5545.31582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Fillenbaum GG, Chandra V, Ganguli M, Pandav R, Gilby JE, Seaberg EC, et al. Development of an activities of daily living scale to screen for dementia in an illiterate rural older population in India. Age Ageing. 1999;28:161–8. doi: 10.1093/ageing/28.2.161. [DOI] [PubMed] [Google Scholar]
- 38.Mathuranath PS, George A, Cherian PJ, Mathew R, Sarma PS. Instrumental activities of daily living scale for dementia screening in elderly people. Int Psychogeriatr. 2005;17:461–74. doi: 10.1017/s1041610205001547. [DOI] [PubMed] [Google Scholar]
- 39.Ganguli M, Chandra V, Gilby JE, Ratcliff G, Sharma SD, Pandav R, et al. Cognitive test performance in a community-based nondemented elderly sample in rural India: The Indo-U.S. Cross-National Dementia Epidemiology Study. Int Psychogeriatr. 1996;8:507–24. doi: 10.1017/s1041610296002852. [DOI] [PubMed] [Google Scholar]
- 40.Pandav R, Fillenbaum G, Ratcliff G, Dodge H, Ganguli M. Sensitivity and specificity of cognitive and functional screening instruments for dementia: The Indo-U.S. Dementia Epidemiology Study. J Am Geriatr Soc. 2002;50:554–61. doi: 10.1046/j.1532-5415.2002.50126.x. [DOI] [PubMed] [Google Scholar]
- 41.Nehra A, Pershad D, Sreenivas V. Indian Aphasia battery: Tool for specific diagnosis of language disorder post stroke. J Neurol Sci. 2013;333:e165. [Google Scholar]
- 42.Chengappa SK, Kumar R. Normative and clinical data on the Kannada version of Western aphasia battery (WAB-K) Lang India. 2008:8. ISSN 1930-2940;1-15. [Google Scholar]
- 43. [Last retrieved on 2017 Mar 12]. Available from: https://www.mcgill.ca/linguistics/research/bat#ebat .
- 44.Pershad D, Verma SK. Hand Book of PGI Battery of Brain Dysfunction (PGIBBD) Agra: National Psychological Corporation; 1990. [Google Scholar]
- 45.Pershad D, Wig NN. Reliability and validity of a new battery of memory tests. Indian J Psychiatry. 1978;20:76–80. [Google Scholar]
- 46.Mukundan CR, Murthy VN. Bangalore, India: Paper Presented at the Joint Conference of Neurology, Psychiatry, Clinical Psychology and Psychiatric Social Work Societies of India, NIMHANS; 1979. Lateralization and Localizing Cerebral Lesions by a Battery of Neuropsychological Tests. [Google Scholar]
- 47.Rao SL, Subbakrishna DK, Gopukumar K. NIMHANS Neuropsychological Battery Manual. Bangalore: NIMHANS Publications; 2004. [Google Scholar]
- 48.Kar BR, Rao SL, Chandramouli BA, Thennarasu K. Neuropsychological Battery for Children Manual. Bangalore: NIMHANS Publications; 2004. [Google Scholar]
- 49.Tripathi R, Kumar JK, Bharath S, Marimuthu P, Varghese M. Clinical validity of NIMHANS neuropsychological battery for elderly: A preliminary report. Indian J Psychiatry. 2013;55:279–82. doi: 10.4103/0019-5545.117149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Gupta S, Khandelwal SK, Tandon PN, Maheshwari MC, Mehta VS, Sundram KR, et al. The development and standardization of a comprehensive neuropsychological battery in Hindi-Adult form. J Pers Clin Stud. 2000;16:75–109. [Google Scholar]
- 51.Sosa AL, Albanese E, Prince M, Acosta D, Ferri CP, Guerra M, et al. Population normative data for the 10/66 Dementia Research Group cognitive test battery from Latin America, India and China: A cross-sectional survey. BMC Neurol. 2009;9:48. doi: 10.1186/1471-2377-9-48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Yepthomi T, Paul R, Vallabhaneni S, Kumarasamy N, Tate DF, Solomon S, et al. Neurocognitive consequences of HIV in Southern India: A preliminary study of clade C virus. J Int Neuropsychol Soc. 2006;12:424–30. doi: 10.1017/s1355617706060516. [DOI] [PubMed] [Google Scholar]
- 53.Pearson Clinical India-India Adapted and Standardized Assessments. [Last retrieved on 2016 Nov 18]. Available from: http://www.pearsonclinical.in/catindiaadaptedandstandardizedassessments/# .
- 54. [Last retrieved on 2017 Mar 15]. Available from: http://www.cnsvs.com/index.html .
- 55. [Last retrieved on 2017 Mar 15]. Available from: http://www.thehindu.com/data/on-computingability-rural-india-is-lost-in-the-woods/article17463258.ece .