

Sir,
Herpes zoster during pregnancy is rare. The incidence is seen in approximately 1/20,000 pregnancies.[1] The treatment modalities include antiepileptic drugs, antidepressants, and various surgical interventions.[2] Acyclovir during acute phase of herpetic eruptions reduces the risk of postherpetic neuralgia (PHN) but its use in nonlife-threatening infections or for suppressing therapy during pregnancy is not recommended by the Centers for Disease Control and Prevention (CDC). Local administration of botulinum toxin-A (BTX-A) is tried with variable success in PHN.[3] We administered fixed doses (500 units of Dysport) of BTX-A in two pregnant women with PHN.[4] The results were analyzed and found to be satisfactory.
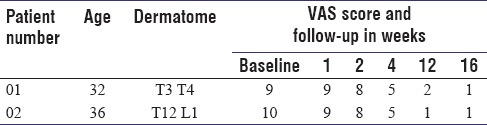
Two pregnant ladies aged 36 years and 38 years, respectively, developed Herpes zoster in 28 and 32 weeks of gestation, in T3 T4 and T12 L1 dermatomal distributions on the anterior side of the chest. Both the patients were treated symptomatically and acyclovir was not administered in either of the cases. In both the patients, pain persisted even after 4 weeks in spite of analgesic and antiepileptic treatment. BTX-A with written consent in fixed dose of 500 units Dysport was administered. The toxin was diluted with 5 mL of normal saline, making a concentration of 100 units/mL. With an insulin syringe it was injected in a checkerboard pattern subcutaneously along the course of skin eruptions. No untoward side effect was observed except mild erythema that subsided after 7 days. The effect of BTX-A on pain was measured on visual analogue scale (VAS) score after 1 week, 2 weeks, 4 weeks, 8 weeks, 12 weeks, and 16 weeks of administration, respectively. The score decreased to 2 to 3 in both the cases. Both the patients remained comfortable during the pregnancy period [Table 1]. Analysis was advised on si opus sit (SOS) basis. Both the patients are still under follow-up. Both the babies delivered were normal and are growing up normally. The patient's age, dermatographic distribution, VAS score at baseline, and follow-up visits (weeks) after BTX-A therapy are shown in the table as below.
Table 1.
Dermatomal distribution and VAS score
We, therefore, recommend its use during pregnancy for PHN to reduce the intensity of pain and avoid analgesic and antiepileptic drugs that may have a harmful effect on the fetus.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Weinberg JM. Herpes Zoster: Epidemiology, natural history and common complications. Jr Acad Dermatol. 2007;57:130–5. doi: 10.1016/j.jaad.2007.08.046. [DOI] [PubMed] [Google Scholar]
- 2.Kost RG, Streauss SE, Wood AJ. Post herpetic neuralgia pathogenesis, treatment, and prevention: A review article. N Engl J Med. 1996;4:32–40. doi: 10.1056/NEJM199607043350107. [DOI] [PubMed] [Google Scholar]
- 3.Bodkin CL, Maurer KB, Wszolek ZK. Botulinum toxin type A therapy during pregnancy. Mov Disord. 2005;20:1081–2. doi: 10.1002/mds.20549. [DOI] [PubMed] [Google Scholar]
- 4.Jain S, S Tamer K, Hiran S, Dwivedi MD. Cosmetic effect of Botulinum Toxin in focal hyperhydrosis. AIAN. 2005;8:45–7. [Google Scholar]