

Abstract
Crowding in emergency departments (EDs) is associated with long lengths of stay (LOS); however, it is not known whether the effect is equal across different chief complaints.
The aim of the study was to compare the effect of crowding on LOS in the 10 most common medical or surgical chief complaints in the ED.
All adult visits to a university hospital ED on weekdays between 8 am and 9 pm in 2012 (n = 19,200) were stratified based on chief complaint and triage priority. The ED bed occupancy rate was measured and crowding was defined as an occupancy rate over one. The impact of crowding on LOS was calculated for the different groups.
During crowding, LOS was longer among all chief complaints (P ≤.01) (except for high-acuity patients with wounds, where the study group was very small). During crowding, LOS increased the most among patients with extremity pain/swelling (145% among high-acuity patients, 125% among low-acuity patients) and flank pain (87% among high-acuity patients, 117% among low-acuity patients) and the least among patients with chest pain (32% among high-acuity patients, 45% among low-acuity patients) or arrhythmia (37% among high-acuity patients, 52% among low-acuity patients).
The effect of ED crowding on LOS is unequal across different chief complaints. These findings could be used to improve the processing of specific chief complaints in the ED.
Keywords: chief complaints, crowding, emergency department, length of stay
1. Introduction
The number of visits to the emergency department (ED) is increasing across the world, resulting in a growing workload and an increase in the occurrence of crowding.[1] Crowding in the ED has been associated with a number of negative consequences for both patient and organization, such as delayed administration of analgesics[2] and antibiotics[3] as well as longer subsequent in-hospital stays[4] and even increased mortality. The occurrence of crowding has also been associated with longer ED length of stay (LOS),[5] that is, the total amount of time a patient spends in the ED, even among patients with a high-acuity level.[6] However, it is not known whether the effect of crowding on LOS is equal across different chief complaints. Such investigations could provide important information regarding which groups are most at risk by the adverse effects of crowding, and enable interventions in the ED directed toward patients with those chief complaints. We therefore conducted a large cohort study, investigating the effect of crowding on LOS in the ten most common medical or surgical chief complaints in the ED.
2. Methods
2.1. Study design and settings
This cross-sectional cohort study included all adult visits to the medicine and surgery ED at Karolinska University Hospital Solna between 8 am and 9 pm on weekdays in 2012. The medical and surgical patients made up approximately half of the ED's annual 80,000 visits, and were handled by the same team, led by an emergency medicine physician. At arrival, triage was conducted according to the Rapid Emergency Triage and Treatment System (RETTS), and the patients were registered with a chief complaint and a priority between 1 (high) and 5 (low). Visits by patients under the age of 18 were excluded from the study, as well as visits by patients arriving during nighttime hours or weekends because staffing and allocation of bed-spaces differed during those settings. A total of 19,702 visits met the inclusion criteria and did not meet the exclusion criteria (Fig. 1). Out of those visits, another 350 were excluded because no priority had been registered, and 152 visits were excluded because the LOS was so short data were assumed to have been wrongly inputted. Hence 19,200 visits were included in the study, out of which 12,607 (66%) had been registered with 1 of the 10 most common chief complaints.
Figure 1.
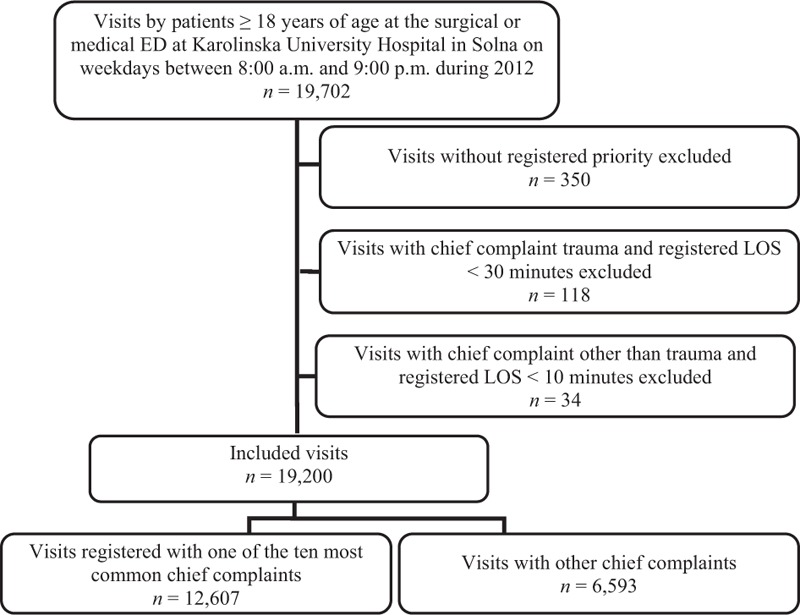
Flow chart of included and excluded visits. ED = emergency department. 1. Asplin BR. Measuring crowding: time for a paradigm shift. Academic emergency medicine: official journal of the Society for Academic Emergency Medicine. 2006;13(4):459-61.
The study was approved by the Regional Ethical Review Board in Stockholm, Sweden (Dnr 2013/796-31/3). This study is a database study on anonymous patient visits; therefore, no informed consent was given by patients.
2.2. Data collection and definitions
Crowding was measured using bed occupancy rate, that is, the ratio of patients to ED beds, and was defined as a bed occupancy rate over one. This measure was selected due to previous studies, feasibility, as well as the clinical relevance and simplicity in understanding the results of the study (1). All visits where the number of patients simultaneously being treated by the emergency physician's teams at some point exceeded the 19 available beds were considered to be exposed to crowding. Information regarding sex, age, chief complaint and acuity according to RETTS, time to evaluation by a physician, LOS, and destination after discharge was automatically collected for the included visits from the electronic patient record database Karda SQL Server 2005 using Qlikview software 11 (QlikTech International AB, Lund, Sweden). LOS was defined as the time between registration of the patient at the front desk, and the time when the patient was registered as having physically left the ED. Patients who during initial triage received priority 1 or 2, that is, were considered to have a potentially life-threatening condition in need of medical attention right away or within 15 minutes, were considered to be high-acuity patients. All other patients (triaged as priority 3, 4, or 5) were considered to be low-acuity patients. The data were stratified based on if crowding occurred at some point during the visit, and further subdivided based on the triage priority given at arrival, so that data for patients considered to be of high acuity could be analyzed separately from those considered to be of low acuity.
2.3. Statistical analysis
For each of the 10 most common chief complaints within the groups of high and low acuity, the median (25th–75th percentiles) LOS for visits that occurred with or without crowding was calculated. The difference in LOS between visits with and without crowding was presented both in minutes and as a percentage, and P values for the differences in LOS were calculated using Mann–Whitney U test. For reference, all 19,200 included visits, regardless of chief complaint, were stratified based on acuity and occurrence of crowding, and the same analyses were conducted on these groups. P < .05 was considered to be significant. All analyses were conducted using SPSS Statistics 23 (IBM, New York).
3. Results
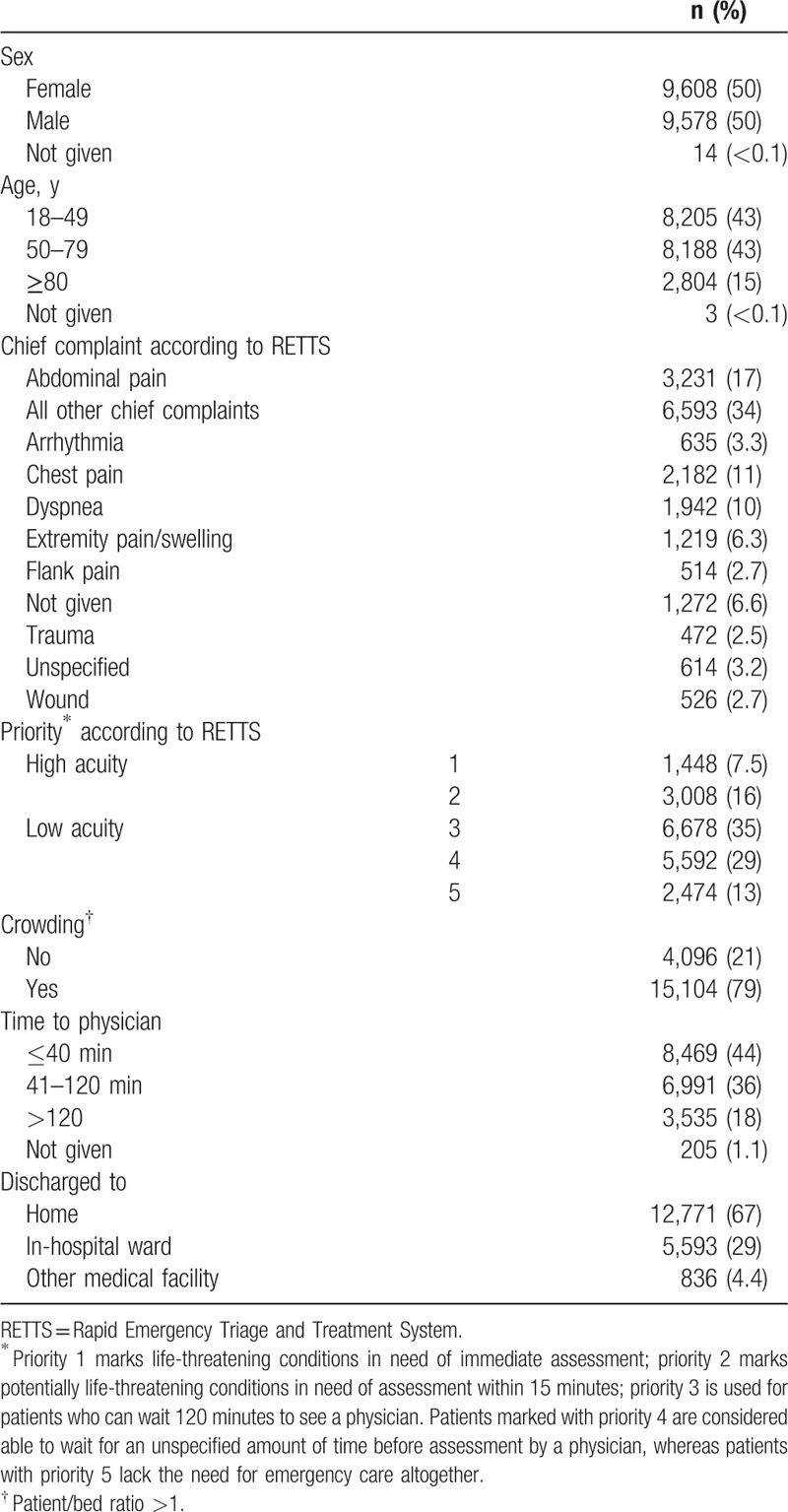
The total population had equal amount of men and women, approximately 15% were aged at least 80 years and crowding occurred in 79% of the visits (Table 1). The 10 most common chief complaints are presented in Table 1. Furthermore, nearly a quarter of all patients had high-acuity visits.
Table 1.
Patient and visit characteristic for the 19,200 included visits.
3.1. High-acuity patients
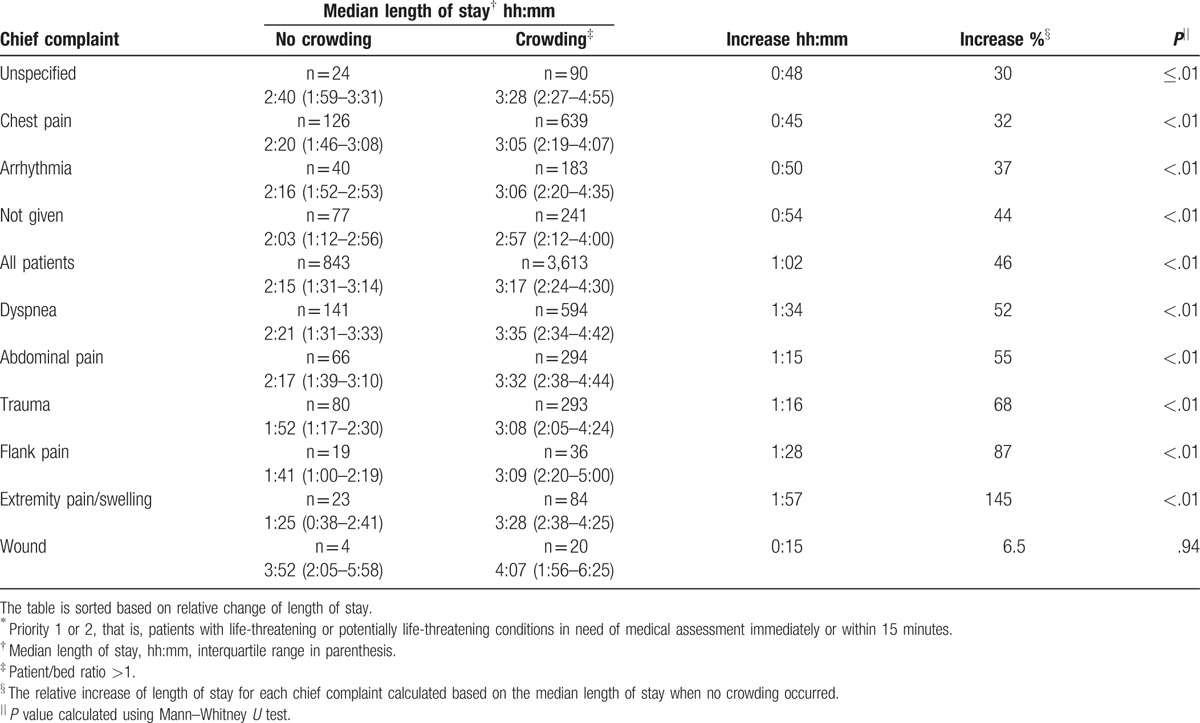
Among all visits by patients initially considered to have a medical condition of high acuity, LOS was 46% longer in the group subjected to crowding than in the group where no crowding occurred (135 vs 197 minutes) (Table 2). The increase in LOS was significant (P ≤ .01) for all studied chief complaints except wounds, where the population was very small. The largest change in LOS was seen among patients with extremity pain/swelling, where LOS increased by 145% (85 vs 208 minutes). Patients with flank pain had an increase in LOS with 87% (101 vs 189 minutes). The smallest increase in LOS was seen among patients with an unspecified chief complaint (30% increase, 160 vs 208 minutes), chest pain (32% increase, 140 vs 185 minutes), or arrhythmia (37% increase, 136 vs 186 minutes).
Table 2.
Length of stay among the 4456 high-acuity∗ patients.
3.2. Low-acuity patients
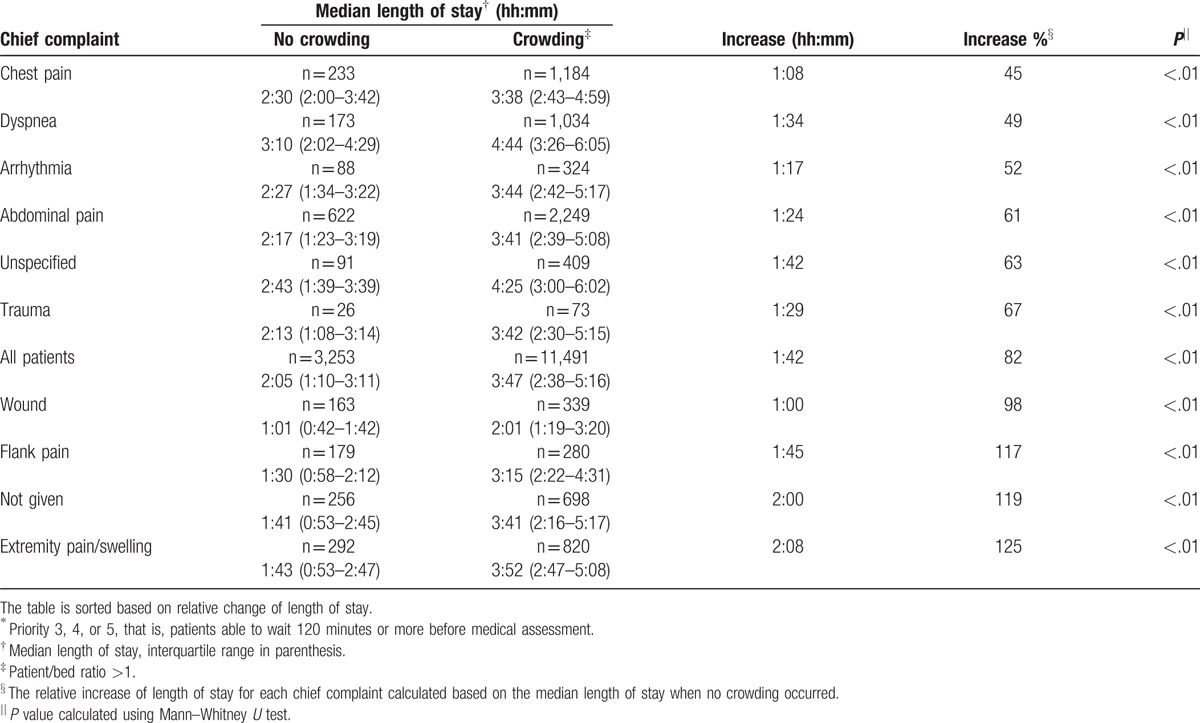
Among all visits by patients initially considered to have a medical condition of low acuity, LOS was 82% longer in the group subjected to crowding (125 vs 227 minutes), and the increase was significant for all of the 10 most common chief complaints (P < .01) (Table 3). The largest change was seen among patients with extremity pain/swelling, where LOS increased by 125% (103 vs 232 minutes). The increase was almost as large among patients with no given chief complaint (119% increase, 101 vs 221 minutes) and among those with flank pain (117% increase, 90 vs 195 minutes). The smallest increase in LOS was seen among patients with chest pain (45% increase, 150 vs 218 minutes), dyspnea (49% increase, 190 vs 284 minutes), or arrhythmia (52% increase, 147 vs 224 minutes).
Table 3.
Length of stay among the 14,744 low-acuity∗ patients.
4. Discussion
In this hospital-based cohort study, LOS for different chief complaints was affected differently by crowding in the ED. The biggest increase of LOS was seen among the low-acuity patients, but the increase was significant among the high-acuity patients as well. In general, chief complaints with a short LOS during periods without crowding had a larger increase of LOS as crowding occurred. This was true regardless of if the increase in LOS was given in minutes or as a percentage.
Previous studies have shown that the timeliness of care in time-sensitive conditions, such as myocardial infarction, is less sensitive to the adverse effects of crowding.[7,8] This has been explained by the use of standardized protocols to rapidly diagnose and treat these patients in the ED.[7] In our study, chest pain or arrhythmia was associated with a relatively small increase of LOS in both high- and low-acuity patients. We theorize that the standardized protocols used to rapidly identify and initiate treatment of the high-acuity patients with these chief complaints, as a secondary effect also accelerates the processing of the low-acuity patients with similar symptoms. A second contributor to the short LOS of these patients may be that they do not require medical imaging, such as computer tomography or ultrasonography, as frequently as some of the other chief complaints. The finding that low-acuity patients with extremity pain/swelling has the largest increase in LOS make sense because many of them need an ultrasound done by the radiology department to rule out a deep vein thrombosis. This finding could motivate the development of standardized protocols aiming at an early initiation of diagnostics in patients with chief complaints greatly affected by occurrence of crowding, such as extremity pain/swelling or flank pain.
Among the high-acuity patients in this study, 58% were discharged to an in-hospital ward, indicating that their LOS in the ED was affected by the availability of in-hospital beds. Still, the finding of a shorter LOS among them compared with low-acuity patients indicate that the staff have given them appropriate attentions as expected for a true high-acuity condition. Among the low-acuity patients this effect ought to have been much smaller, as only 20% in this group was discharged to an in-hospital ward. As the difficulty in finding in-hospital beds for patients in need of further treatment is a major cause of both crowding and prolonged LOS,[9] the smaller increase of LOS seen among the high-acuity patients is gladdening.
It is remarkable that 9.8% of the visits in this study had been registered with no chief complaint or with an unspecified chief complaint. The suspected heterogeneity within these groups makes it hard to evaluate the changes in LOS. However, previous studies have demonstrated that patients within these groups have an increased mortality[10] and are at a high risk of having their medical acuity underestimated at triage.[11] The need to further develop the triage tools to better evaluate and treat these patients is apparent.
4.1. Strengths and limitations
The generalizability of these findings is limited by the fact that this was a single-center study, with only daytime visits included. Future studies need to include patient visits 24/7 because visits occurring nighttime are likely to effect day visits. Also, although the usage of bed occupancy rate as an indicator of crowding is well established, it has its limitations. For an instance, it does not adjust for current staffing, actual bed availability, or the severity of the patients’ conditions. The occurrence of crowding may also vary during a visit, and more sensitive measures may have provided further information about the processes in the ED.
Some of the foremost strengths of this study are the long study period and the large study population. To our knowledge, this is the first study investigating the negative effect of crowding on such a large number of chief complaints, and the findings may help to better direct interventions of the ED.
5. Conclusions
This study shows that the effect of crowding on LOS is unequal across different chief complaints. Regardless of the acuity of the patients’ needs, those presenting with extremity pain/swelling or flank pain were the most affected by crowding, whereas patients with chest pain or arrhythmia were less affected. Further analysis based on this knowledge could be used to improve the processing of specific chief complaints in the ED.
Footnotes
Abbreviations: ED = emergency department, LOS = length of stay, RETTS = Rapid Emergency Triage and Treatment System.
The authors have no funding and conflicts of interest to disclose
References
- [1].Jayaprakash N, O'Sullivan R, Bey T, et al. Crowding and delivery of healthcare in emergency departments: the European perspective. West J Emerg Med 2009;10:233–9. [PMC free article] [PubMed] [Google Scholar]
- [2].Pines JM, Hollander JE. Emergency department crowding is associated with poor care for patients with severe pain. Ann Emerg Med 2008;51:1–5. [DOI] [PubMed] [Google Scholar]
- [3].Pines JM, Localio AR, Hollander JE, et al. The impact of emergency department crowding measures on time to antibiotics for patients with community-acquired pneumonia. Ann Emerg Med 2007;50:510–6. [DOI] [PubMed] [Google Scholar]
- [4].Derose SF, Gabayan GZ, Chiu VY, et al. Emergency department crowding predicts admission length-of-stay but not mortality in a large health system. Med Care 2014;52:602–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Perdahl T, Axelsson S, Svensson P, et al. Patient and organizational characteristics predict a long length of stay in the emergency department—a Swedish cohort study. Eur J Emerg Med 2015;24:284–9. [DOI] [PubMed] [Google Scholar]
- [6].McCarthy ML, Zeger SL, Ding R, et al. Crowding delays treatment and lengthens emergency department length of stay, even among high-acuity patients. Ann Emerg Med 2009;54:492–503. [DOI] [PubMed] [Google Scholar]
- [7].Harris B, Bai JC, Kulstad EB. Crowding does not adversely affect time to percutaneous coronary intervention for acute myocardial infarction in a community emergency department. Ann Emerg Med 2012;59:13–7. [DOI] [PubMed] [Google Scholar]
- [8].Ward MJ, Baker O, Schuur JD. Association of emergency department length of stay and crowding for patients with ST-elevation myocardial infarction. West J Emerg Med 2015;16:1067–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].White BA, Biddinger PD, Chang Y, et al. Boarding inpatients in the emergency department increases discharged patient length of stay. J Emerg Med 2013;44:230–5. [DOI] [PubMed] [Google Scholar]
- [10].Nemec M, Koller MT, Nickel CH, et al. Patients presenting to the emergency department with non-specific complaints: the Basel Non-specific Complaints (BANC) study. Acad Emerg Med 2010;17:284–92. [DOI] [PubMed] [Google Scholar]
- [11].Djärv T, Castrén M, Mårtenson L, et al. Decreased general condition in the emergency department: high in-hospital mortality and a broad range of discharge diagnoses. Eur J Emerg Med 2015;22:241–6. [DOI] [PubMed] [Google Scholar]