

Supplemental Digital Content is available in the text
Keywords: rehabilitation, spinal cord injury, spontaneous spinal epidural hematomas, treatment
Abstract
Rationale:
Spontaneous spinal epidural hematoma (SSEH) is a relatively rare but potentially disabling disease, and the classical presentation of it includes an acute onset of severe, sometimes radiating back or neck pain, followed by signs and symptoms of rapidly evolving nerve root or spinal cord compression.
Patient concerns:
Here, we report a 26-year-old female patient presented with weakness in bilateral lower extremities, progressing to intense paraplegia and anesthesia without recent medical history of trauma, infection, surgery, or drug use.
Diagnosis:
A magnetic resonance imaging (MRI) scan of spinal cord was planned and a posterior epidural hematoma of the thoracic spine was observed.
Interventions:
A posterior decompression and hematoma evacuation was performed after diagnosis immediately. Early rehabilitation program of the specific kind spinal cord injury was formulated and implemented.
Outcomes:
The patient finally can handle basic living activities, such as completing wheelchair locomotion, transferring from bed to wheelchair independently after 3 months of rehabilitation.
Lessons:
SSEH is a rarely occurring case in emergency. Acute chest pain and paraplegia could be the initial presentation of acute spinal epidural hemorrhage, but the diagnosis of patient without classical manifestations is still a challenge for doctors. Early diagnosis, prompt decompression, and individualized rehabilitation program can improve the prognosis and outcome.
1. Introduction
Spontaneous spinal epidural hematoma (SSEH) is a relatively rare occurring but potentially disabling disease. It was first described by Blauby in 1808.[1] The incidence is estimated at 0.1 per 100,000 individuals.[2,3] The classical presentation of it includes an acute onset of severe, sometimes radiating back or neck pain, followed by signs and symptoms of rapidly evolving nerve root or spinal cord compression. Although any part of the spine may be involved, at the lower cervical and thoracolumbar spinal levels are reported as the most common site of SSEH.[4,5] The true etiology of the SSEH is still unknown, but the associations with some predisposing conditions, such as coagulopathy, use of anticoagulants, arteriovenous malformation, have been reported.[1,5] The progressive neurological deficit requires urgent treatment, and emergency decompression of the spinal cord and the evacuation of the hematoma remain the standard management.[6,7] Early and individualized rehabilitation program after recovery of the operation is beneficial for SSEH patients.
This article presents a previously healthy young woman who was admitted to the emergency department with weakness of bilateral lower extremities caused by SSEH, in whom prompt surgical treatment and immediate rehabilitation proposal prevented definitive neurological sequelae.
2. Case report
A 26-year-old female patient presented to our emergency department with weakness in bilateral lower extremities of 3-hour duration without any pain in body part after waking up in the morning. Blood pressure was 120/60 mm Hg. There was no recent medical history of trauma, infection, surgery, or drug use. The initial laboratory tests of blood, such as blood routine test, liver function test, blood creatinine, electrolytes, the activated partial thromboplastin time, and the international normalized ratio, were within normal limits. The neurological examinations revealed loss of strength of both lower extremities and the muscle strength was grade 0/5. The loss of skin sensation was below the T4 vertebral level with saddle anesthesia. Babinski reflex of bilateral lower extremities was positive and the anal sphincter tone and bilateral tendon reflex were reduced. Magnetic resonance imaging (MRI) of the cervical and dorsal spines revealed a posterior epidural hematoma from T4 to T7 level with spinal cord compression. The mass had isointensity to the spinal cord on T1-weighted images and hyperintensity on T2-weighted images (Fig. 1). The patient was hospitalized in the orthopedic department after diagnosis of SSEH and an operation was planned. Posterior approach decompression laminectomy and hematoma evacuation was performed on the patient. A bilateral laminectomy from T4 to T7 was performed. Thick, clotted blood, and prominent epidural hematoma were seen, but no obvious vascular malformation was found during operation. The hematoma was evacuated, the cord adequately decompressed, and tissue was sent for histology. The pathologic report described a hematoma without neoplasm or vessel malformation.
Figure 1.
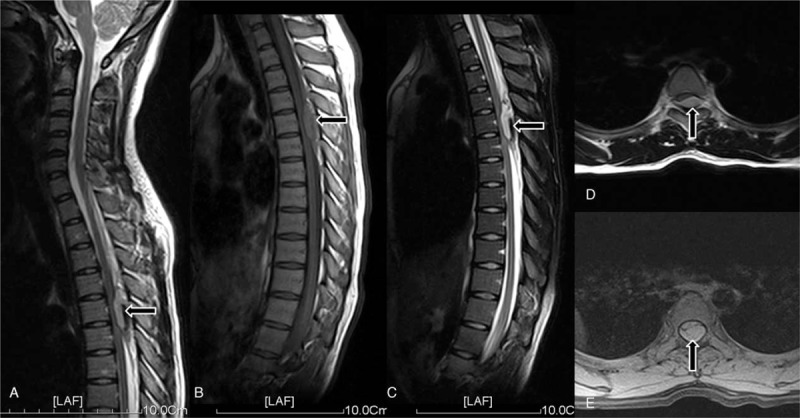
Spinal cord MRI of this case. (A) Shows the location of the hematoma which is a posterior epidural hematoma from T4-T7 level with spinal cord compression. (B) The mass had isointensity to the spinal cord on T1-weighted sagittal scanning images. (C) The mass had hyperintensity to the spinal cord on T2-weighted sagittal scanning images. (D) The mass had isointensity to the spinal cord on T1-weighted coronal scanning images. (E) The mass had hyperintensity to the spinal cord on T2-weighted coronal scanning images.
After the healing of the incision, the patient was transferred to the department of rehabilitation medicine. Preoperative spinal cord status assessment was AIS A scale. A detailed rehabilitation schedule was established for the early rehabilitation program, which included passive joint range of motion (ROM) training of lower limbs, active joint ROM training of upper limbs, muscle strength enhance training, pulmonary function training, and position change training. After gaining enough upper limbs strength, the next stage of training began, which included seat balancing training, tilting table training, transfer training (bed to wheelchair), and activities of daily living training (ADL training). The patient finally could handle basic living activities, complete wheelchair locomotion, and transfer from bed to wheelchair independently.
3. Discussion
SSEH is always defined as accumulation of blood in the vertebral epidural space which requires prompt diagnosis and treatment to prevent morbidity and mortality. Patients with classical clinical presentation always present with a sudden severe and acute back or neck pain around the affected vertebrae, followed by rapid progress to symptoms and pathological signs of spinal cord compression.[3,4,6,8] The pathogenesis of it is still unclear, though the cause of it has been discussed thoroughly in the previous literature. Whether the origin of the bleeding is arterial or venous still cannot be decided. The latest meta-analysis of SSEH showed that the main bleeding is assumed to be of venous region, because of the compression is probably limited.[3] The location of the hematomas are usually posterior to the spinal cord according to one large literature survey,[9] and this location has a consistency between the thoracic cavities and the valveless epidural venous plexus distribution in the spinal cord, while the valveless epidural venous plexus is particularly vulnerable to variations in pressure from the abdominal and thoracic cavities.[5] The hematoma in this case has the same location as reported in the prior literature, but what seems different is that there is no sudden pain or any symptoms of subjective feelings. The probable reasons for this asymptomatic case maybe that the origin of the hematoma is venous and the expansion velocity of the hemorrhage was not as fast as considered, which cannot induce the pain from compressed spinal neural structures.[7]
Early recognition of the symptoms and rapid diagnostic evaluation is essential to minimize delay in treatment of SSEH. Several studies have shown that MRI is the preferred diagnostic method of SSEH,[1,5,10,11] which may explain the increased report of the SSEH. Conventional MRI can estimate the bleeding occurrence, location, size, and severity of the spinal cord compression, based on the signal intensities of hematomas in T1 and T2-weighted images. Early MRI of SSEH reveals isointensity or hypointensity on T1-weighted images, and hyperintensity on T2-weighted images. As the MRI images showed previously, this case has the same radiological manifestations.
Surgical decompression of the neural structures and removal of the hematoma is the appropriate modality of treatment in the majority of patients with SSEH.[4,7] Urgent decompression of the spinal cord assumes to be the initial step for the recovery of the patient. The type and the degree of preoperative neurological deficit, and time interval to surgery are the most critical factors affecting functional recovery of patients.[1,6,8,10] The midthoracic area seems the most vulnerable for ischemic insult, not only because of the venous plexus described earlier but also because the epidural space is narrowest between T3 and T9.[6,12] The clinical outcomes in those patients should be significantly worse. Posterior decompression and hematoma evacuation was performed immediately after hospitalization on this patient in the hope of a better prognosis.
Unlike traumatic spinal epidural hematoma, SSEH does not damage adjacent structures such as bones or soft tissues (such as ligaments), and the spinal cord injury (SCI) is also unlikely to demonstrate signs of contusion. This kind of SCI could be treated as nontraumatic SCI, and SSEH seems to be one of the most frequent vascular causes of nontraumatic SCI.[13] A number of studies have found that early SCI rehabilitation is beneficial.[14–16] The main rehabilitation goals of the SSEH inpatients are to reduce the occurrence rate of disability through increasing patients’ independence in performing activities and to decrease the relevant limitations of impairments. On account of the primary stability of the spinal cord, early rehabilitation plan maybe particularly suitable for SSEH patients. One retrospective study of New PW et al[17] finally concluded that most nontraumatic SCI patients finally gained good mobility, better bladder function and bowel status, compared with traumatic ones with SCI in other studies, and the patients’ disability was usually remarkably reduced after comprehensive rehabilitation program. Physical therapy (PT), occupational therapy (OT), and sports therapy are main rehabilitation strategies which could make contributions to improve the physical performance and capacity in mobility and self-care of the patients with SCI.[18,19] Conversely, according to a retrospective comparison study of Cosar SN et al[20] reported that despite more impairment in patients with traumatic SCI according to the ASIA scale scores, there was no significant difference in functional gain between patients with traumatic and nontraumatic SCI. Strategies are needed to improve future research in comparison of traumatic and nontraumatic SCI to treat different SCI patients. As the mechanism of SCI caused by SSEH is so different from traumatic SCI,[21] whether an adapted rehabilitation program of the SSEH patients is needed or not is still unknown. One recent study of Vervoordeldonk JJ et al[13] called for different rehabilitation needs for nontraumatic SCI. Some new attempts, such as new functional recovery measures[22] and new international standards for neurological classification of SCI,[23] have emerged to deal with different cases through individualized ways. In this case, the patient was given specific PT, OT, and sports therapy according to the early rehabilitation schedule. The largest proportion of time was spent on treatment to improve muscle power and wheelchair propulsion, all of which are the basic function needs during early rehabilitation. The patient finally can handle basic living activities, such as completing wheelchair locomotion, transferring from bed to wheelchair independently after 3 months of rehabilitation.
4. Conclusion
In conclusion, SSEH is a rarely occurring case in emergency. Acute chest pain and paraplegia could be the initial presentation of acute spinal epidural hemorrhage. Early diagnosis, prompt decompression, and individualized rehabilitation program can improve the prognosis and outcome. The diagnosis of patients without classical manifestations is still a challenge for doctors. Early MRI test can help evaluate the condition of the hematoma and the spinal cord. Early rehabilitation of nontraumatic SCI patients focusing on basic function handling can benefit patients on the early stage. But we also highlight that much more research into the pathogenesis, prognostic factors, and effectiveness of inpatients’ rehabilitation is needed, especially for different nontraumatic ones.
Acknowledgment
The authors thank the patient for consenting to this report, as well as sharing and providing detailed documentation of her experience.
Supplementary Material
Footnotes
Abbreviations: ADL training = activities of daily living training, AIS = ASIA impairment score, MRI = magnetic resonance imaging, OT = occupational therapy, PT = physical therapy, ROM = range of motion, SCI = spinal cord injury, SSEH = spontaneous spinal epidural hematoma.
HX and LX collected the clinical material and retrieved literature, conceived of the study, and participated in its design and coordination and drafted the manuscript. CHL, WXW, and GDF formulated and implemented the rehabilitation program, and helped to evaluate the spinal cord status. JMH retrieved data, and participated in design and drafting of the manuscript. KJL and LL supervised design, coordination, and drafting of the manuscript, revised the final edition of the manuscript for important professional content. All authors read and approved the final manuscript.
The authors report no funding and conflicts of interest.
Supplemental Digital Content is available for this article.
References
- [1].Aycan A, Ozdemir S, Arslan H, et al. Idiopathic thoracic spontaneous spinal epidural hematoma. Case Rep Surg 2016;2016:15430708. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Holtås S, Heiling M, Lönntoft M. Spontaneous spinal epidural hematoma: findings at MR imaging and clinical correlation. Radiology 1996;199:409–13. [DOI] [PubMed] [Google Scholar]
- [3].Bakker NA, Veeger NJ, Vergeer RA, et al. Prognosis after spinal cord and cauda compression in spontaneous spinal epidural hematomas. Neurology 2015;84:1894–903. [DOI] [PubMed] [Google Scholar]
- [4].Hussenbocus SM, Wilby MJ, Cain C, et al. Spontaneous spinal epidural hematoma: a case report and literature review. J Emerg Med 2012;42:e31–4. [DOI] [PubMed] [Google Scholar]
- [5].Taniguchi LU, Pahl FH, Lúcio JE, et al. Complete motor recovery after acute paraparesis caused by spontaneous spinal epidural hematoma: case report. BMC Emerg Med 2011;11:10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Foo D. Operative treatment of spontaneous spinal epidural hematomas: a study of the factors determining postoperative outcome. Neurosurgery 1997;41:1218–20. [DOI] [PubMed] [Google Scholar]
- [7].Groen RJ. Non-operative treatment of spontaneous spinal epidural hematomas: a review of the literature and a comparison with operative cases. Acta Neurochir 2004;146:103–10. [DOI] [PubMed] [Google Scholar]
- [8].Estaitieh N, Alam S, Sawaya R. Atypical presentations of spontaneous spinal epidural hematomas. Clin Neurol Neurosurg 2014;122:135–6. [DOI] [PubMed] [Google Scholar]
- [9].Kunz U. Spinal hematoma: a literature survey with meta-analysis of 613 patients. Neurosurg Rev 2003;26:52. [DOI] [PubMed] [Google Scholar]
- [10].Fedor M, Kim ES, Ding K, et al. Spontaneous spinal epidural hematoma: a retrospective study on prognostic factors and review of the literature. Korean J Spine 2011;8:272–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Saritas A, Guneysu F, Guneysu S, et al. An unusual presentation of spontaneous spinal epidural hematoma. J Emerg Med 2014;47:689–91. [DOI] [PubMed] [Google Scholar]
- [12].Hsieh CT, Chang CF, Lin EY, et al. Spontaneous spinal epidural hematomas of cervical spine: report of 4 cases and literature review. Am J Emerg Med 2006;24:736–40. [DOI] [PubMed] [Google Scholar]
- [13].Vervoordeldonk JJ, Post MW, New P, et al. Rehabilitation of patients with nontraumatic spinal cord injury in the Netherlands: etiology, length of stay, and functional outcome. Top Spinal Cord Inj Rehabil 2013;19:195–201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Scivoletto G, Morganti B, Molinari M. Neurologic recovery of spinal cord injury patients in Italy. Arch Phys Med Rehabil 2004;85:485–9. [DOI] [PubMed] [Google Scholar]
- [15].Scivoletto G, Morganti B, Molinari M. Early versus delayed inpatient spinal cord injury rehabilitation: an Italian study. Arch Phys Med Rehabil 2005;86:512–6. [DOI] [PubMed] [Google Scholar]
- [16].van der Putten JJ, Stevenson VL, Playford ED, et al. Factors affecting functional outcome in patients with nontraumatic spinal cord lesions after inpatient rehabilitation. Neurorehabil Neural Repair 2001;15:99–104. [DOI] [PubMed] [Google Scholar]
- [17].New PW. Functional outcomes and disability after nontraumatic spinal cord injury rehabilitation: Results from a retrospective study. Arch Phys Med Rehabil 2005;86:250–61. [DOI] [PubMed] [Google Scholar]
- [18].Harvey LA, Lin CW, Glinsky JV, et al. The effectiveness of physical interventions for people with spinal cord injuries: a systematic review. Spinal Cord 2009;47:184–95. [DOI] [PubMed] [Google Scholar]
- [19].van Langeveld SA, Post MW, van Asbeck FW, et al. Feasibility of a classification system for physical therapy, occupational therapy, and sports therapy interventions for mobility and self-care in spinal cord injury rehabilitation. Arch Phys Med Rehabil 2008;89:1454–9. [DOI] [PubMed] [Google Scholar]
- [20].Cosar SN, Yemisci OU, Oztop P, et al. Demographic characteristics after traumatic and non-traumatic spinal cord injury: a retrospective comparison study. Spinal cord 2010;48:862–6. [DOI] [PubMed] [Google Scholar]
- [21].Rajz G, Cohen JE, Harnof S, et al. Spontaneous spinal epidural hematoma: the importance of preoperative neurological status and rapid intervention. J Clin Neurosci 2015;22:123–8. [DOI] [PubMed] [Google Scholar]
- [22].Anderson K, Aito S, Atkins M, et al. Functional recovery measures for spinal cord injury: an evidence-based review for clinical practice and research. J Spinal Cord Med 2008;31:133–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Kirshblum SC, Biering-Sorensen F, Betz R, et al. International Standards for Neurological Classification of Spinal Cord Injury: cases with classification challenges. J Spinal Cord Med 2014;37:120–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.