

Abstract
Early rehabilitation after surgery for patellar fracture is challenging. The purpose of this study was to evaluate the surgical outcome of titanium cable cerclage for patellar fracture in early functional activity.
We reviewed a series of 24 patients treated at our hospital with titanium cable. Functional exercises were started early. Patients were followed up for at least 12 months.
Fifteen were males and 9 were females. Fracture occurred in the right knee in 13 patients and in the left knee in 11 patients. The most common mode of injury involves a tumble. None of the patients presented with any postoperative complications. The management resulted in satisfactory outcomes.
Titanium cable cerclage offers a new strategy in treating patellar fracture.
Keywords: patellar fracture, tension band wiring, titanium cable cerclage
1. Introduction
Patellar fracture is a common skeletal fracture, which accounts for approximately 1% of all skeletal injuries.[1] Open reduction and internal fixation is recommended for displaced fractures or comminuted fractures to restore extensor continuity and articular congruity. The common technique consists of stainless steel wire placed through tension bands around Kirschner wires (K-wires). After operative treatment, immobilization, which refrains from redisplacement of the fracture in early stage, may cause arthrofibrosis and a stiff knee, and the steel wire fixation can break, cause painful irritation, and/or migrate.[2,3] To avoid knee stiffness and decreased range of motion, early mobilization is necessary. Therefore, the above-mentioned complications have prompted the use of alternative materials in place of stainless steel wire.
Titanium cable cerclage can provide stable fracture fixation of the patella to allow early mobilization without fracture displacement. In comminuted fractures, especially, the titanium cable allows anatomic reduction and stabilization of multiple fragments. To evaluate the effectiveness of this technique in the treatment of patellar fractures, we conducted this retrospective study to evaluate the postoperative outcomes of patients managed using this technique.
2. Materials and methods
The study protocol was approved by the Ethics Committee of the Second Affiliated Hospital, School of Medicine, Xi’an Jiaotong University. Written informed consent was obtained from all the patients included in this study.
2.1. Patients
From November 2012 to November 2015, 24 patients with patellar fracture were treated surgically with the titanium cables at our hospital. All patients presented the surgery indications advocated by Cramer and Moed.[4] The clinical data of the patients, including age, sex, history of past illness, surgical procedures, clinical presentation, neurologic status, and ancillary tests, were recorded and retrieved in this study.
2.2. Instruments
Titanium cables were purchased from Zhejiang Guangci Medical Device CO., Ltd (Cixi, China). The cable is equipped with specialized surgical instruments (Fig. 1), such as cannulated and a wire inducer (to pass the wire).
Figure 1.
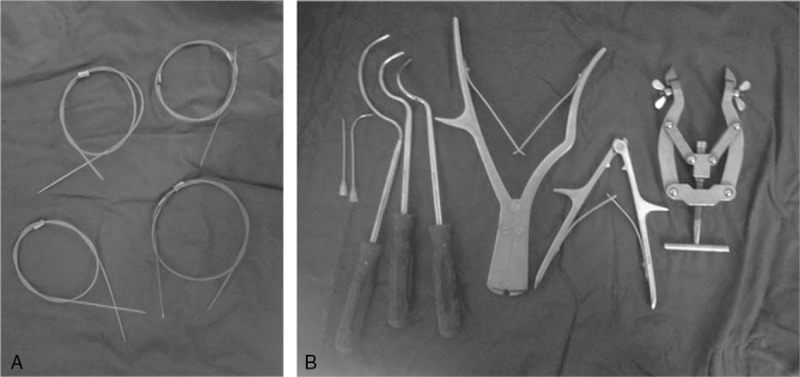
The titanium cable and specialized surgical instruments.
2.3. Procedure
Under general or spinal anesthesia, surgery was performed in supine position with the injured knee extended. The tourniquet was used. An incision was made along the inferior border of the patella. After incising the superficial fascia, the extensor apparatus was exposed, and then the patella was completely exposed. The fractured patella was thus presented. A hematoma might be present and should be debrided. The fracture was then reduced with reduction forceps, and two 2-mm K-wires were inserted into the fragments to hold the fracture. In some cases, more K-wires were demanded to penetrate the fracture line. The number of K-wires used in each patient depended on the type and extent of the fracture. The articular surface was checked by image intensifier. After the K-wires went across the fracture site, a titanium cable was placed in a ring-shaped pattern around the circumferential patella close to the bone. The cable ends were next to each other at the medial or lateral aspects of the patella. The cable was then tightened to prevent displacement of the fragments, during which congruity of the articular surface was checked again under the image intensifier. The cerclage was performed without difficulty. The stability of fixation was assessed by bending the knee. The proximal ends of K-wires were bent over towards the patella to prevent slipping of the wires. The distal tip of each wire was trimmed and cut to avoid irritation of the soft tissue. The ends of each wire were buried under the skin.
In most cases, K-wires were maintained after the fracture was adequately repositioned, since it was quite difficult to hold the fragments without the help of the wires. Only in 3 patients, the wires were removed after cerclage was performed.
2.4. Postoperation
Functional exercises with active quadriceps exercises were started as early as the first day after operation in these cases, and mobilization without weight bearing was allowed in an extended position. Four weeks after operation, full weight-bearing was allowed.
2.5. Follow-up
The patients were followed up at 2 weeks, 12 weeks, 6 months, and 1 year. The range of motion of the knee at time of 12 months postoperatively, and any complications were recorded. The function of the knee was evaluated by Böstman score[5] at 1-year follow-up. The implant was removed if a secondary operation was required.
3. Results
Among the 24 patients with patellar fracture, 15 were males and 9 were females, ranging from 21 to 85 years old, with an average of 54.67 ± 15.43 years. Eleven fractures were of the left patella and 13 were of the right. All the fractures were closed injuries; 20 were caused by tumble, 3 by fall, and 1 by motor vehicle accident (Table 1). One patient had undergone a nickel-titanium patellar concentrator fixation 40 days before this hospitalization.
Table 1.
Clinical features of the patients.
None of the patients received a blood transfusion. All the patients had an uneventful postoperative course. No postoperative complications, including infection, were encountered, and no early displacement occurred after the fixation.
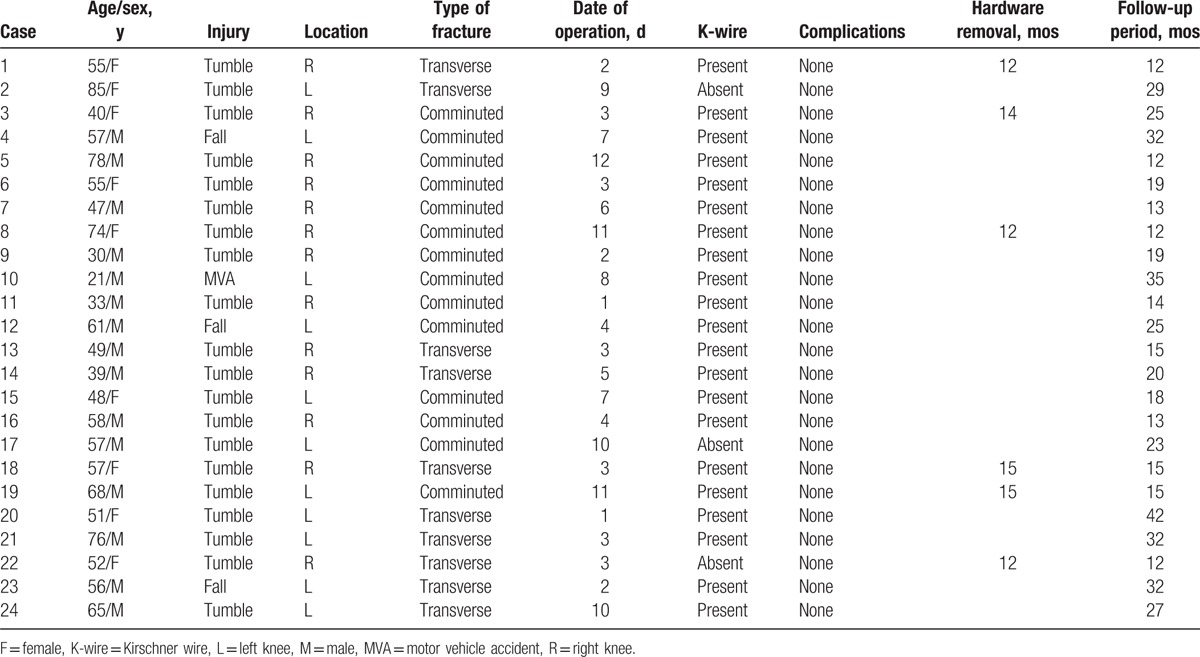
All patients were followed up. The mean follow-up period was 21.29 ± 8.75 (range 12–42) months. Twenty patients had excellent treatment results and 4 had good results. All the patients gained up to 90 degrees of active flexion at the end of week 4 after operation. At week 12, all the patients had full range of movement, and could walk and squat without any restrictions. All the fractures achieved union by the end of week 12. None of the patients developed postoperative knee stiffness. At 1-year follow-up, radiographs detected no broken cables and implant-related symptoms in any of the patients (Fig. 2). No postoperative complications, including local irritation, sinus tract formation, loss of reduction, or breakage, were encountered. Of the 3 patients with K-wires removed, only a 52-year-old female experienced migration of a titanium cable 4 weeks after surgery (Fig. 3), but this migration was related to the absence of K-wires. The displacement of the cable remained asymptomatic and the cable remained anteriorly around the knee joint. In this patient, the titanium cables were removed 1 year after operation. The patients were satisfied with the excellent knee function regained.
Figure 2.

Radiographs of patellar fracture. (A) Before surgery; (B) 2 weeks after surgery; (C) 1 year after surgery.
Figure 3.
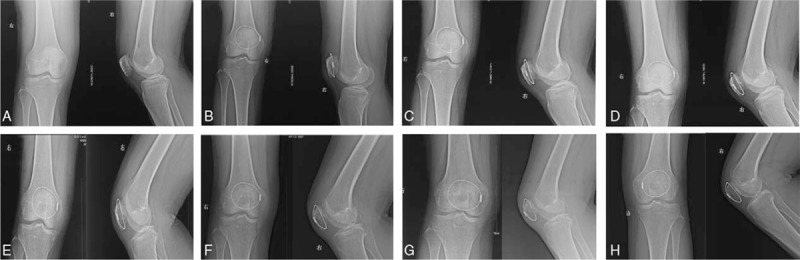
Titanium cable migration. (A) Before surgery; (B) 1 day after surgery; (C) 2 weeks after surgery; (D) 4 weeks after surgery; (E) 2 months after surgery; (F) 3 months after surgery; (G) 5 months after surgery; (H) 1 year after surgery.
Hardware removal was performed in 6 cases during the study period. Reasons for removal were migration in 1 case and patients’ request in 5 cases. The 5 patients who did not complain about symptomatic hardware were troubled for foreign materials. Hardware removal occurred at an average of 13.33 ± 1.51 (range 12–15) months.
4. Discussion
Fixation by using conventional figure-of-eight tension band requires immobilization of the knee after operation, which delays rehabilitation of the knee. Decreased range of motion is a common complication in patients with patellar fractures, and management of such fractures remains challenging because of the desire for early active knee motion. To facilitate rehabilitation in these patients, mobilization is recommended after stable fixation of the fractures. Our study shows that titanium cables can restore the joint surface and provide stable fixation for early mobilization. The cables offer an alternative strategy for treating patients with any fracture of patellar.
In our clinical experiences, indications for application of the titanium cables include either comminuted or transverse fractures, especially significant comminution. The cables may also be indicated in rare cases of failed internal fixation (Fig. 4). We claim that titanium cerclage cables are strong enough to allow early mobilization of the knee joint because the cables retain the shape of the patella. There is thus no need for knee immobilization postoperatively. A previous study on patients treated with tension band wiring reported that a fragment displacement of more than 2 mm occurred in 22% of the patients with early mobilization.[3] In contrast, our cases demonstrate that the titanium cable cerclage allows early functional exercise and gets satisfactory results. Although 1 patient experienced displacement of cable cerclage 4 weeks after surgery, the patient acquired full range of motion and bone union within 3 months during the course of recovery. Our follow-up records show a 100% union rate and no wire breakage during the follow-up period. Based on these results, we believe that the titanium cable provides adequate fixation in patellar fracture and allows early movement. The advantages of this technique include early mobilization and ease of use, particularly in comminuted fracture. However, a major disadvantage of this method is migration of the cable if K-wires are absent.
Figure 4.

Failure of nickel-titanium patellar concentrator fixation. (A) Before surgery; (B) 1 day after surgery; (C) 4 months after surgery.
Here we introduce our experience in using titanium cable cerclage to manage patellar fracture. Based on our cases, we would like to share 5 important points in applying this technique. First, K-wires are positioned to protect the titanium cable fixation, and the wires can prevent slipping of the cerclage in early rehabilitation. Second, the titanium cable should contact the K-wire closely at the superior and inferior edge of patella. This is critical to the success of the management because loose bone-to-cable interfaces would not endure displacement of fracture during knee joint motion. In our cases, the loosening did not occur secondary to soft tissue shifting or necrosis. Third, the titanium cable passing circumferentially around the patella should be closely along the cortical bone. Make sure the cable is next to the bone. Fourth, the knots should be buried in the lateral soft tissue to reduce symptoms caused by them. Fifth, titanium cable cerclage can be used, after other internal fixation failures.
This study had the following limitation: the series of patients involved was small. Larger studies are needed to fully evaluate its role in clinical practice.
5. Conclusions
We describe a novel surgical technique for patellar fractures. The titanium cable can be used for the majority of patella fractures. This technique may afford comparable stability of the fracture during early stage compared with steel wire techniques.
Footnotes
Abbreviation: K-wire = Kirschner wire.
The authors report no conflicts of interest.
References
- [1].Boström A. Fracture of the patella. A study of 422 patellar fractures. Acta Orthop Scand Suppl 1972;143:1–80. [DOI] [PubMed] [Google Scholar]
- [2].Weber MJ, Janecki CJ, McLeod P, et al. Efficacy of various forms of fixation of transverse fractures of the patella. J Bone Joint Surg Am 1980;62:215–20. [PubMed] [Google Scholar]
- [3].Smith ST, Cramer KE, Karges DE, et al. Early complications in the operative treatment of patella fractures. J Orthop Trauma 1997;11:183–7. [DOI] [PubMed] [Google Scholar]
- [4].Cramer KE, Moed BR. Patellar fractures: contemporary approach to treatment. J Am Acad Orthop Surg 1997;5:323–31. [DOI] [PubMed] [Google Scholar]
- [5].Böstman O, Kiviluoto O, Nirhamo J. Comminuted displaced fractures of the patella. Injury 1981;13:196–202. [DOI] [PubMed] [Google Scholar]