

Abstract
[Purpose] The present study aimed to conduct a comparative analysis of changes in mechanical characteristics of cervical muscles and cervical posture in patients with cervicogenic headache following exercise program intervention in order to present effective treatment methods for such patients. [Subjects and Methods] A total of 30 patients with cervicogenic headache were recruited and 15 patients were allocated to cervical stretching exercise group and 15 to cervical stretching exercise and cranio-cervical flexion exercise group. After 3 weeks of exercise intervention, craniovertebral angle and tone (Hz) and stiffness (N/m) of the suboccipital and upper trapezius muscles were measured. [Results] After the exercise program intervention, a greater amount of change in tone of suboccipital and upper trapezius muscles was found in the experimental group, as compared to the control group, but the difference was not statistically significant. Greater amount of change in muscle stiffness and craniovertebral angle was found in the experimental group, as compared to the control group. [Conclusion] Findings of the present study showed that cranio-cervical exercise was an effective form of exercise for changing muscle characteristics and posture in patients with cervicogenic headache. Such findings will be helpful in providing effective treatments for patients with cervicogenic headache.
Key words: Cervicogenic headache, Cranio-cervical flexion, Mechanical properties
INTRODUCTION
Cervicogenic headache refers to repetitive and persistent pain in the cervical and cranial areas that occurs secondarily from anomalies in the soft tissues in the cervical spine or cervical areas1). It is a syndrome that is characteristic of chronic pain mostly in one side of the head that is the same side where cervical musculoskeletal impairment appears2). The structures that cause pain in the cervical region include the suboccipital muscles, C1-2 nerve roots, C2-3 intervertebral discs, upper cervical ligaments, and synovial joints. Moreover, the suboccipital nerves may be the source of headache that occurs in the occipital region as they send nerve branches to the atlanto-occipital joint, while pain originating from cervical muscles can cause referred pain in the head and face3). Methods for treating cervicogenic headache include the foremost recommended method of joint mobilization, along with manipulation, soft tissue mobilization and stretching techniques, retraining of special postural muscle groups, and patient lifestyle training4). Hamilton et al.5) analyzed changes in pain threshold in the suboccipital muscles after separately applying muscle energy and manipulation techniques, while Dunning et al.6) observed changes in cervical impairment indices in patients with cervicogenic headache after applying manipulation to the upper cervical and upper thoracic spine regions. Vavrek et al.7) applied cervical massage to patients with cervicogenic headache and observed changes in their pain and functional impairment. Along with these, there are other on-going studies that have applied various physical therapy interventions to patients with cervicogenic headache for investigation of therapeutic effects. Cervical stabilization exercise strengthens deep muscles that play a dominant role in cervical postural control and stability in patients with cervical impairment, which induces maintenance of neutral cervical posture8). Jull et al.9) observed scalene and sternocleidomastoid muscle activity after applying 6 weeks of intervention consisting of different exercise therapies to patients with chronic cervical pain. The results showed that sternocleidomastoid and scalene muscle activity decreased to a greater degree in the cervical stabilization exercise group than in other groups. Zito et al.10) observed sternocleidomastoid muscle activity while applying deep cervical flexion exercise to patients with cervicogenic headache, patients with migraine, and healthy subjects. The results showed that sternocleidomastoid muscle activity was higher in patients with cervicogenic headache than the other groups. It was surmised that such results were due to patients with cervicogenic headache not being able to effectively use deep cervical flexion muscles, as compared to those in other groups.
As shown, stabilization exercise training has positive effects on patients with cervicogenic headache. However, most of the existing studies used electromyography (EMG) to measure and analyze muscle activity or subjectively measured muscle elasticity or stiffness by manual examination, while studies that analyzed postural changes after stabilization exercises in patients with cervicogenic headache are lacking. The present study divided patients with cervicogenic headache into the control group, in which cervical stretching exercise was applied, and the experimental group, in which both cervical stretching and cranio-cervical flexion exercises were applied. Exercise intervention was applied to both groups for 3 weeks, and comparative analysis was performed on changes in posture and characteristics of upper cervical muscles between the 2 groups. Our objective was to present an effective method for postural analysis and application of exercise therapy in patients with cervicogenic headache.
SUBJECTS AND METHODS
The present study was conducted from April 15 to May 12, 2017. A total of 30 patients with cervicogenic headache were recruited. Their age ranged from 20 to 42 years. Using random clinical sampling, patients were assigned to the experimental group (n=15), which participated in cervical stretching and stabilization exercise programs, or the control group (n=15), which participated in cervical stretching exercise program only. The subjects were those who had been diagnosed with cervicogenic headache based on International Headache Society diagnostic criteria, and their duration of disease ranged between 4 months and 2 years.
For cervical stretching exercise, lateral flexion was performed in the opposite direction of and rotation was performed in the same direction of the muscle that would stretch the neck in sitting position. The therapist stood behind the patient and used one hand to immobilize the thoracic skeleton and the other hand to immobilize the patient’s head. When the patient breathed, the thoracic skeleton was immobilized and relaxed, which was repeated 5–6 times. Moreover, the C2 spinous process was felt and this location was immobilized with the thumb as the patient nodded. The therapist induced the motion and instructed the patient to maintain it for about 10 s, and the stretching exercise was repeated 5–6 times. Cranio-cervical flexion exercise was performed while lying down with the knees bent. After placing a pressure sensor (Stabilizer, Chattanooga Group, TX, USA) underneath the subject’s neck, about 20 mmHg of air, which is enough to fill the space between the neck and floor, was used to fill. The subject was instructed to performed smooth nodding action to induce cranio-cervical flexion. Pressure in the sensor would increase up to 2–10 mmHg depending on the subject. Such state of increased pressure was maintained for 10 s and this was repeated 10 times11).
The mechanical characteristics of cervical muscles were measured using MytonPRO (Myoton AS, Tallinn, Estonia). Tone (Hz) and stiffness (N/m) in the left and right suboccipital muscle and upper trapezius muscles were measured and the mean values were analyzed. Tone (Hz) and stiffness (N/m) values were calculated as the mean value measured 5 times. The measurement method involved pressing the skin with a force of 0.18 N and subsequently applying instantaneous impulse of 0.4 N in 15-ms intervals to the skin. Afterwards, skin surface vibration caused by MytonPRO was measured to confirm the values of mechanical variables12). For measurement of cervical posture, photographs taken from the side were used for objective measurement of forward head posture. The patient was instructed to assume a standing posture, and then to relax. The camera was positioned at shoulder height, and after printing the photographs taken, the craniovertebral angle, which represented the angle of forward head posture, was measured. The craniovertebral angle was derived from the angle formed by the horizontal line that passed the 7th cervical vertebra and the line that connected the tragus of the ear and C7 spinous process (Fig. 1)13). The value of the craniovertebral angle were calculated as the mean value measured 5 times. To examine the mechanical characteristics of cervical muscles and changes in forward head posture between the experimental and control groups after different exercise therapy interventions, the present study performed an analysis of covariance. Statistical significance level was set to α=0.05, and SPSS 19.0 for Windows was used for statistical analysis. This study was approved by Bioethics Committee of Sehan University Center (IRB) (Approval number: 2017–02) on March 31, 2017.
Fig. 1.
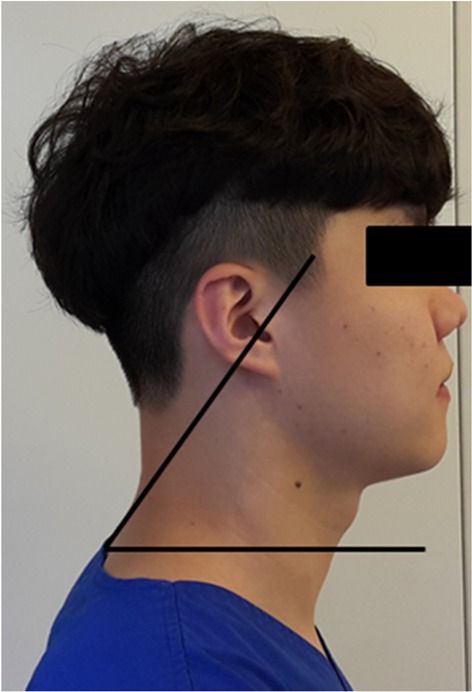
The craniovertebral angle: the angle between C7, the tragus, and the horizontal
RESULTS
The general characteristics of the subjects are shown in Table 1. When comparing suboccipital and upper trapezius muscle characteristics of the experimental and control groups before and after exercise program intervention, greater amount of change in tone was found in the experimental group, as compared to the control group, but the difference was not statistically significant. Greater amount of change in stiffness was found in the experimental group (p<0.05; Table 2). With respect to craniovertebral angle for analyzing forward head posture, greater amount of change was found in the experimental group (p<0.05; Table 3).
Table 1. General characteristics of the subjects.
| M ± SD | ||
|---|---|---|
| Control group | Experimental group | |
| Gender (male/female) | 5/10 | 4/11 |
| Age (years) | 32 ± 5.0 | 31 ± 6.5 |
| BMI (kg/m2) | 21.6 ± 2.0 | 21.89 ± 2.5 |
Values are shown as mean (M) ± standard deviation (SD)
Control group: cervical stretching exercise; Experimental group: cervical stretching exercise + deep cervical flexion exercise; BMI: body mass index
Table 2. Comparison of muscle mechanical properties between the groups.
| Control group | Experimental group | |||
|---|---|---|---|---|
| Pre | Post | Pre | Post | |
| SO Tone (Hz) | 16.1 ± 1.3 | 14.9 ± 1.3 | 15.6 ± 1.5 | 13.8 ± 1.3 |
| SO Stiffness (N/m) | 309.4 ± 19.3 | 285 ± 23.9 | 310.2 ± 19.4 | 275 ± 22.9* |
| UT Tone (Hz) | 18.8 ± 2.0 | 17.3 ± 1.6 | 19.3 ± 2.1 | 16.8 ± 1.4 |
| UT Stiffness (N/m) | 323.6 ± 29.0 | 304.1 ± 26.7 | 342.1 ± 34.6 | 313.1 ± 28.0* |
Values are shown as mean ± standard deviation.
*Significant difference between the two groups (p<0.05).
Control group: cervical stretching exercise; Experimental group: cervical stretching exercise + deep cervical flexion exercise; SO: suboccipital; UT: upper trapezius
Table 3. Comparison of craniovertebral angle between the groups.
| Control group | Experimental group | |||
|---|---|---|---|---|
| Pre | Post | Pre | Post | |
| FHP (degree) | 49.4 ± 1.7 | 51.2 ± 1.8 | 49 ± 1.8 | 52.5 ± 1.5* |
Values are shown as the mean ± SD.
* Significant difference between the two groups (p<0.05).
Control group: cervical stretching exercise; Experimental group: cervical stretching exercise + deep cervical flexion exercise; FHP: forward head posture
DISCUSSION
The present study recruited 30 patients with cervicogenic headache and assigned them to experimental (n=15) and control (n=15) groups by random clinical sampling. After applying different exercise therapy intervention for 3 weeks, tone and stiffness in the upper trapezius and suboccipital muscles were measured and craniovertebral angle was also measured for comparative analysis in order to identify if exercise intervention causes any changes.
Tone in the upper trapezius and suboccipital muscles decreased in both the experimental and control groups after exercise intervention. Although the control group showed a higher value, the difference was not statistically significant. Hamilton5) applied high velocity low amplitude manipulation and muscle energy technique stretching exercise to 65 subjects and found that there were changes in their suboccipital muscle pain threshold. When the value of tone is higher, it is said to represent increased degree of pain and exercise overload14). In the present study, both the experimental and control groups showed a decrease in tone, which is an indicator of pain sense. These results were similar to the findings in a study by Hamilton5), meaning cervical stretching and cranio-cervical exercise reduced pain by decreasing the tone of muscles around the cervical vertebrae.
Stiffness of upper trapezius and suboccipital muscles decreased after exercise intervention in both groups, and in particular, the experimental group, which had both stretching exercise and cervical stabilization exercise applied together, showed significantly lower stiffness values than the control group. Zito et al.10) recruited 25 healthy subjects and 27 patients with cervicogenic headache and observed their sternocleidomastoid muscle activity during cervical stabilization exercise. The results demonstrated that patients with cervicogenic headache had higher sternocleidomastoid muscle activity than the healthy subjects. Moreover, Jull et al.9) recruited 40 patients with chronic cervical pain and observed their sternocleidomastoid muscle activities after applying cervical stabilization exercise to only 20 patients and cervical muscle strengthening exercise to the other 20 patients. The results showed that the group that had cervical stabilization exercise applied had decreased sternocleidomastoid muscle activity, as compared to the group that had muscle strengthening exercise applied. Increase in sternocleidomastoid muscle activity reflects weakening of deep cervical flexion muscles, which can lead to difficulties in maintaining the neutral cervical posture. In the present study, stiffness value decreased in the group that received intervention by cranio-cervical flexion exercise, which is believed to be the result of stiffness in cervical muscles decreasing from neutral cervical posture being maintained by strengthening of the deep cervical flexion muscles.
In the present study, changes in forward head posture were measured for observation of postural changes after intervention with different exercise therapies. The results showed that forward head posture decreased more in the experimental group than in the control group, but the difference was not statistically significant. Chae & Lee13) applied 8 weeks of cervical stabilization exercise on 24 patients with tension type headache and performed comparative analysis on the changes in their forward head posture. The results showed that there was a significant increase in craniovertebral angle which reflects the forward head posture in both sitting and standing positions. Such results were similar to the findings in the present study, demonstrating that cranio-cervical flexion exercise improved forward head posture by increasing the craniovertebral angle.
The present study performed comparative analysis on the changes in mechanical characteristics of muscles and posture in patients with cervicogenic headache after applying intervention with different exercise programs. The results showed that the group that had cervical stretching and stabilization exercise applied had greater amount of changes in tone, stiffness, and cervical posture. If such points are taken into account when applying exercise therapy to patients with cervicogenic headache, the patients can be maintained more effectively.
Acknowledgments
This research was supported by research grant of Sehan Univercity in 2017.
REFERENCES
- 1.Jang JH, Sagong ES: Chiropractic manipulation treatment in cervicogenic headache. Kosin Med J, 2008, 23: 107–110. [Google Scholar]
- 2.Biondi DM: Cervicogenic headache: a review of diagnostic and treatment strategies. J Am Osteopath Assoc, 2005, 105: 16S–22S. [PubMed] [Google Scholar]
- 3.Choi BO, Kim JD, Joo MJ: A review of physical therapies approach for cervicogenic headache. J Korean Soc Phys Ther, 2003, 3: 212–221. [Google Scholar]
- 4.Lee JH, Kang DH, Kang JI: The effects of myofascial relaxation on blood flow velocity of the cranial artery and pain level in cervicogenic headache patients. J Korean Soc Phys Ther, 2010, 22: 49–57. [Google Scholar]
- 5.Hamilton L, Boswell C, Fryer G: The effects of high-velocity, low-amplitude manipulation and muscle energy technique on suboccipital tenderness. Int J Osteopath Med, 2007, 10: 42–49. [Google Scholar]
- 6.Dunning JR, Butts R, Mourad F, et al. : Upper cervical and upper thoracic manipulation versus mobilization and exercise in patients with cervicogenic headache: a multi-center randomized clinical trial. BMC Musculoskelet Disord, 2016, 17: 64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Vavrek D, Haas M, Peterson D: Physical examination and self-reported pain outcomes from a randomized trial on chronic cervicogenic headache. J Manipulative Physiol Ther, 2010, 33: 338–348. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Cho HY: Effects of cervical stabilization exercise type on muscle strength and endurance, cross sectional area of cervical in patients with chronic cervical pain. Doctoral dissertation, Korean Univercity, 2011.
- 9.Jull GA, Falla D, Vicenzino B, et al. : The effect of therapeutic exercise on activation of the deep cervical flexor muscles in people with chronic neck pain. Man Ther, 2009, 14: 696–701. [DOI] [PubMed] [Google Scholar]
- 10.Zito G, Jull G, Story I: Clinical tests of musculoskeletal dysfunction in the diagnosis of cervicogenic headache. Man Ther, 2006, 11: 118–129. [DOI] [PubMed] [Google Scholar]
- 11.Kisner C, Colby LA: Therapeutic exercise foundations and techniques. Philadelphia: FA Davis, 2007. [Google Scholar]
- 12.Bailey L, Samuel D, Warner M, et al. : Parameters representing muscle tone, elasticity and stiffness of biceps brachii in healthy older males. J Neurol Disord, 2013, 1: 116. [Google Scholar]
- 13.Chae YW, Lee HM: The effect of craniocervical exercise on tension-type headache. J Korean Soc Phys Ther, 2009, 21: 9–16. [Google Scholar]
- 14.Kim DH, Kim SK, Jung YJ, et al. : Measurement of low back muscle characteristic change using MyotonPRO in a long-term driving: pilot study. J Ergon Soc Korea, 2015, 4: 592–598. [Google Scholar]