

Abstract
Background: Flexor tendon ruptures in the wrist are uncommon. Flexor carpi radialis (FCR) tendon rupture can occur in rheumatoid patients, following cortisone injection for tenosynovitis, and following trauma. Following tendon rupture, tethering of the ruptured FCR tendon, or pseudotendon, can form which may or may not be symptomatic. Methods: A literature review was done reviewing treatment and outcomes of FCR tendon lesions. A case report of painful FCR pseudotendon following a fall is presented. The patient presented 4 months after injury with a tender lump 6 cm proximal to the wrist joint with pain and weakness aggravated with wrist motion and gripping. Results: The literature review reveals operative excision of a symptomatic FCR pseudotendon lesion results in great patient satisfaction with no morbidity. In this case report, in spite of conservative measures including cortisone injection and activity modification, the patient had persistent symptoms. The patient proceeded with surgery for complete excision of both the painful pseudotendon and retracted FCR tendon stump. Post-operatively, his wrist motion and grip strength returned to normal, and his Disabilities of the Arm, Shoulder, and Hand (DASH) score was significantly improved from 72 to 9. Conclusions: FCR pseudotendon is an uncommon condition and can be seen following trauma. Majority of FCR tendon ruptures resolve with non-operative treatment. Based on the excellent outcomes following complete FCR tendon harvest for thumb carpometacarpal (CMC) joint reconstruction, complete excision of a symptomatic pseudotendon results in excellent relief of symptoms with no long-term morbidity.
Keywords: flexor carpi radialis, rupture, pseudotendon, tethering, excision
Introduction
Flexor tendons ruptures are uncommon.1,3,8 Ruptures of the flexor carpi radialis (FCR) tendon are rare in nonrheumatoid patients.1 FCR tendon rupture can occur following a cortisone injection for tenosynovitis.5,7,8,13-15 Attritional FCR tendon ruptures are also seen with scaphotrapezial arthritis.3,4,7,8,13 In this article, we present a case report of a painful FCR pseudotendon following a fall. After failed nonoperative treatment, the painful pseudotendon was completely excised and the patient returned to work. The clinical presentation, pathology, treatment, and literature review of this rare entity are discussed.
Case Report
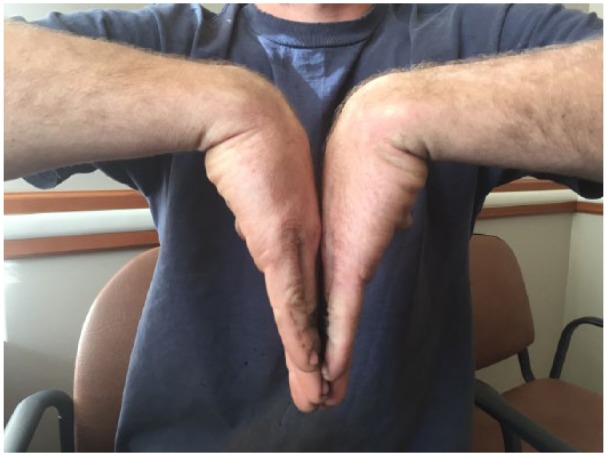
This 28-year-old right-handed male construction worker presented to our office 4 months following a fall on his outstretched right hand. He fell 5 feet from a platform and had immediate pain and swelling in his wrist and hand. When seen in our office, he complained of right wrist and forearm pain. At that time, he was tender and swollen along the FCR tendon (Figure 1). Approximately 6 cm proximal to the wrist joint, there was a painful lump. His pain was aggravated with wrist extension, flexion, and gripping. He also complained of dorsal wrist pain and was tender over the scapholunate interval. Watson’s maneuver was positive. Grip strength, determined with a JAMAR dynamometer, was 108% compared with the uninvolved hand. The Disabilities of the Arm, Shoulder, and Hand (DASH) score was 72. Plain radiographs of the wrist were normal. A 3T magnetic resonance imaging (MRI) scan/arthrogram was done to rule out a carpal ligament injury and showed an intrasubstance tear of the FCR tendon (Figure 2). The carpal ligaments were normal. The FCR sheath was injected with 0.5% Sensorcaine and Dexamethasone. The patient had 2 hours of pain relief following the cortisone injection. The swelling improved but his pain worsened.
Figure 1.
Physical exam showing thickened flexor carpi radialis tendon.
Figure 2.

3T GE magnetic resonance imaging/arthrogram.
Note. a, Axial T1-weighted image demonstrates thickening of distal flexor carpi radialis tendon or pseudotendon (arrow). b, Axial T2-weighted fat-saturated image demonstrates thickening of distal flexor carpi radialis tendon or pseudotendon (arrow). c, Sagittal T1-weighted image demonstrates thickening of flexor carpi radialis tendon or pseudotendon with a distal tear (arrow). d, Sagittal T2-weighted fat-saturated image demonstrates thickening of the flexor carpi radialis tendon or pseudotendon with a distal tear (arrow).
One month following the injection, there was no improvement in the symptoms, and he elected to have surgery. The tendon was exposed through a longitudinal incision. Dissection was done on the radial side of the tendon to avoid injury to the palmar cutaneous branch of the median nerve. The FCR tendon sheath was swollen and discolored. There was marked thickening of the distal third of FCR tendon and sheath (Figure 3). The entire tendon was excised and the proximal musculotendinous junction sutured beneath the deep forearm fascia (Figure 4). Examination of the excised tendon showed marked thickening of the distal third of the specimen. Sectioning of the tendon revealed fibrous tissue consistent with the tendon regeneration (Figure 5). Microscopic examination revealed fibrotendinous changes with inflammatory changes in the tendon structure (Figure 6).
Figure 3.
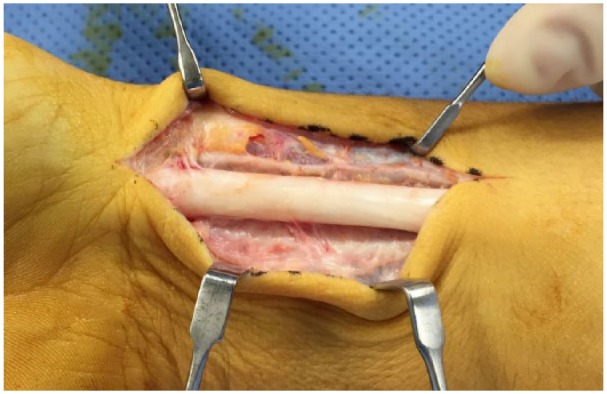
Intraoperative photo showing thickening of distal flexor carpi radialis tendon.
Figure 4.

Intraoperative photo following excision of flexor carpi radialis tendon.
Figure 5.
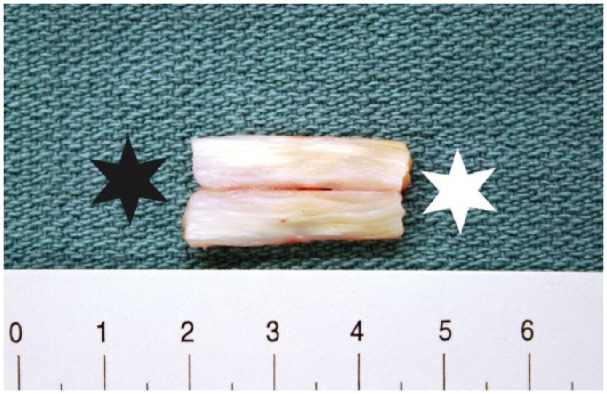
Flexor carpi radialis tendon section which is cut in half lengthwise and opened to reveal normal tendon appearance on the right half (white star) and pseudotendon on the left half (black star).
Figure 6.
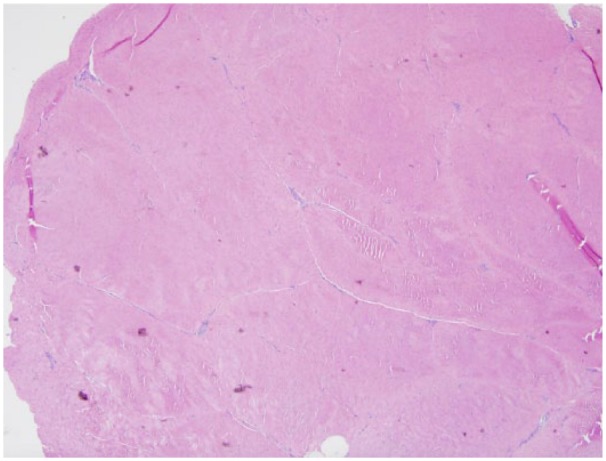
Photomicrograph of pseudotendon showing loss of normal tendon architecture with fibrotendinous tissue with perivascular chronic inflammation.
Following surgery, he was immobilized in a short-arm splint for 10 days. At the first postoperative visit, the sutures were removed and he began active range of motion with a removable orthoplast splint. He gradually discontinued the splint over the next several months.
He returned to the office 6 months following surgery. He had changed jobs and was working full-time as a diesel mechanic. He rated his pain as 0. The scar was well healed (Figure 7). There was no sign of any FCR tendon regeneration. He did complain of some paresthesia along the distal portion of the incision. Sensation was normal in the hand.
Figure 7.

Six-month postoperative photo of involved wrist.
Wrist range of motion was within normal limits (flexion, 50°; extension, 70°; supination, 80°; and pronation, 70°; Figures 8 and 9). Grip strength of the right hand was 106% compared with the left hand. QuickDASH at the 6-month exam was 9 (preoperative value, 72).
Figure 8.

Six-month postoperative wrist range of motion, extension.
Figure 9.
Six-month postoperative wrist range of motion, flexion.
Discussion
Rupture of the FCR tendon is uncommon in nonrheumatoid patients. Several studies have reported a small number of patients with an FCR tendon rupture (Table 1). When a rupture occurs, it is most frequently associated with scaphotrapeziotrapezoid (STT) arthritis or a previous cortisone injection of the tendon.1,3,4,6-8,13 The FCR tendon inserts into the base of the second and third metacarpal and is a major wrist flexor. The tendon enters the fibro-osseous tunnel of the trapezium occupying 90% of the available space and is in direct contact with the trapezium. This close proximity to the carpal structures may lead to communication between an arthritic scaphotrapezial joint and resultant inflammatory response in the FCR tendon.2,4,8
Table 1.
Flexor Carpi Radialis Tendon Lesions.
| Year | Author | Journal | Number of patients | Treatment | Result |
|---|---|---|---|---|---|
| 1968 | Fitton et al4 | J Bone Joint Surg Br | 30 | 18 operative | 11 satisfied |
| 12 nonoperative | |||||
| 3—fraying | |||||
| 1—rupture | |||||
| 1—gelatinous | |||||
| 1—red, adherent | |||||
| 1978 | Weeks14 | Plast Reconstr Surg | 4 (2 rupture) | 1 excision; 1 transverse carpal ligament | Good |
| 1984 | Bowe et al3 | J Hand Surg Am | 1—bilateral (rupture) | Nonoperative | Satisfactory |
| 1991 | Tonkin and Stern13 | J Hand Surg Br | 3 (rupture) | 1 operative; 2 nonoperative | |
| 1992 | Irwin et al8 | J Hand Surg Br | 1 (rupture) | Operative; stump excision | |
| 1994 | Gabel et al6 | J Bone Joint Surg Am | 10 (4 rupture) | 9 of 10 satisfied | |
| 2013 | Henry7 | J Hand Microsurg | 6 | Tendon excision | All improved |
Typically, patients with FCR tendon rupture have minimal disability and functional loss. This is in contrast to the dramatic loss of function seen in patients with digital flexor tendon ruptures.5-8,13,15 Pseudotendon formation commonly occurs after a flexor tendon injury. In 1985, Kulick et al10 reported pseudotendon formation involving both flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) tendons in 3 patients. The pseudotendon formation was noted after flexor tendon injury and was a result of attempted biologic repair of the divided flexor tendon. As in our patient, the pseudotendon showed loss of normal tendon architecture and lacked the white glistening surface of normal tendon. In addition, the tensile strength of the pseudotendon was less than normal tendon.10 Physical examination of this rare condition can be confusing. When the wrist is examined, the regenerated “pseudotendon”7 or “neotendon”8 can appear to be a normal tendon. The pseudotendon is thickened and will have a painful lump approximately 6 cm proximal to the wrist joint. This lump is the retracted FCR tendon. Pseudotendon formation is regeneration of the FCR tendon. Regeneration of the FCR tendon is common after full thickness use in carpometacarpal (CMC) joint arthroplasty.11 An MRI study of wrists following full-thickness FCR harvest for CMC joint arthroplasty showed the regenerative powers of the FCR tendon: partial regeneration in 79% of patients and complete regeneration in 14% of patients. The regenerated tendon was not normal in strength.11
Wrist extension and gripping will cause pain along the course of the weak regenerated pseudotendon.7 In this case, an MRI/arthrogram was done to evaluate the wrist for a possible ligament injury. A more cost-effective alternative would be an ultrasound exam of the wrist.9,12 Conservative, nonoperative modalities are the first line of treatment. These include therapy, anti-inflammatory medication, activity modification, splinting, and cortisone injections.3,4,6-8,13,14 If conservative measures fail, surgical options are available. Although tendon transfer has been described,6 complete excision of the pseudotendon and the ruptured proximal tendon is recommended.7,8,13,14
In this case, the proximal FCR tendon stump was sutured deep to the forearm fascia to prevent irritation from scar tissue.14
In the largest series of FCR tendon ruptures, Henry7 reported 6 patients with FCR tendon ruptures. All 6 patients had previous cortisone injections and 3 had symptomatic STT arthritis. All patients failed nonoperative treatment including splints, oral medication, therapy, and ultrasound. Definitive treatment consisted of complete excision of the FCR pseudotendon and FCR stump.
This operative treatment of complete tendon excision is based on the clinical outcomes of patients following complete harvest of the FCR tendon for CMC joint arthroplasty.7,11
Following full-thickness harvest of the tendon for CMC joint arthroplasty, significant changes in wrist kinetics are noted. In spite of the altered mechanics and loss of strength, excellent clinical outcomes (as measured by DASH scores, and pinch and grip strength testing) are seen in this group of arthroplasty patients.11
Henry7 reported 6 patients who all improved with complete excision of the pseudotendon and proximal stump. In that group, all patients had improvement in their preoperative symptoms. The average preoperative DASH scores were 32 and improved to 3 after surgery.
The majority of FCR tendon ruptures can be treated nonoperatively.8,13 Why this subgroup of patients has so much pain and disability from the tethered pseudotendon remains unanswered.7,8 This is in contrast to other cases of tendon ruptures at the wrist with loss of function and relatively little pain.8
In this case, the patient presented with a swollen, painful FCR tendon 4 months after a fall. The MRI/arthrogram of the wrist, done to rule out a ligament injury, showed an intrasubstance tear of the FCR tendon. This finding is similar to the “pseudotendon” described by Henry7 and the “neotendon” described by Irwin et al.8 This reaction may be a variant of FCR tendon regeneration.
Based on excellent historical outcomes following complete harvest of the FCR for CMC reconstruction, complete excision of the pseudotendon and retracted tendon stump was done for this patient.7 Following surgery, his clinical exam improved and he returned to his regular construction job.
Footnotes
Ethical Approval: This study was approved by our institutional review board.
Statement of Human and Animal Rights: This article does not contain any studies with human or animal subjects.
Statement of Informed Consent: No identifying patient information is present in this article.
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
- 1. Anzel SH, Covey KW, Weiner AD, Lipscomb PR. Disruption of muscles and tendons; an analysis of 1,014 cases. Surgery. 1959;45:406-414. [PubMed] [Google Scholar]
- 2. Bishop AT, Gabel G, Carmichael SW. Flexor carpi radialis tendinitis. Part I: operative anatomy. J Bone Joint Surg Am. 1994;76:1009-1014. [DOI] [PubMed] [Google Scholar]
- 3. Bowe A, Doyle L, Millender LH. Bilateral partial ruptures of the flexor carpi radialis tendon secondary to trapezial arthritis. J Hand Surg Am. 1984;9:738-739. [DOI] [PubMed] [Google Scholar]
- 4. Fitton J, Shea FW, Goldie W. Lesions of the flexor carpi radialis tendon and sheath causing pain at the wrist. J Bone Joint Surg Br. 1968;50:359-363. [PubMed] [Google Scholar]
- 5. Fitzgerald BT, Hofmeister EP, Fan RA, Thompson MA. Delayed flexor digitorum superficialis and profundus ruptures in a trigger finger after a steroid injection: a case report. J Hand Surg Am. 2005;30:479-482. [DOI] [PubMed] [Google Scholar]
- 6. Gabel G, Bishop AT, Wood MB. Flexor carpi radialis tendinitis. Part II: results of operative treatment. J Bone Joint Surg Am. 1994;76:1015-1018. [DOI] [PubMed] [Google Scholar]
- 7. Henry M. Pseudotendon formation causing painful tethering of ruptured flexor carpi radialis tendons. J Hand Microsurg. 2013;5:1-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Irwin LR, Outhwaite J, Burge PD. Rupture of the flexor carpi radialis tendon associated with scapho-trapezial osteoarthritis. J Hand Surg Br. 1992;17:343-345. [DOI] [PubMed] [Google Scholar]
- 9. Jeyapalan K, Bisson MA, Dias JJ, Griffin Y, Bhatt R. The role of ultrasound in the management of flexor tendon injuries. J Hand Surg Eur Vol. 2008;33:430-434. [DOI] [PubMed] [Google Scholar]
- 10. Kulick MI, Kilgore ES, Newmeyer WL., III Pseudotendon formation after flexor tendon injury. J Hand Surg Am. 1985;10:638-640. [DOI] [PubMed] [Google Scholar]
- 11. Naidu SH, Poole J, Horne A. Entire flexor carpi radialis tendon harvest for thumb carpometacarpal arthroplasty alters wrist kinetics. J Hand Surg Am. 2006;31:1171-1175. [DOI] [PubMed] [Google Scholar]
- 12. Schöffl VR, Schöffl I. Injuries to the finger flexor pulley system in rock climbers: current concepts. J Hand Surg Am. 2006;31:647-654. [DOI] [PubMed] [Google Scholar]
- 13. Tonkin MA, Stern HS. Spontaneous rupture of the flexor carpi radialis tendon. J Hand Surg Br. 1991;16:72-74. [DOI] [PubMed] [Google Scholar]
- 14. Weeks PM. A cause of wrist pain: non-specific tenosynovitis involving the flexor carpi radialis. Plast Reconstr Surg. 1978;62:263-266. [PubMed] [Google Scholar]
- 15. Yamada K, Masuko T, Iwasaki N. Rupture of the flexor digitorum profundus tendon after injections of insoluble steroid for a trigger finger. J Hand Surg Eur Vol. 2011;36:77-78. [DOI] [PubMed] [Google Scholar]