

First-line treatment for young/fit patients with chronic lymphocytic leukemia (CLL) is the combination of fludarabine, cyclophosphamide and rituximab (FCR), which has improved these patients’ progression-free survival and overall survival,1 but is poorly tolerated by elderly patients or patients with comorbidities.2 Such patients have been historically treated with chlorambucil, which is well tolerated but does not improve survival.3 To improve outcomes, chlorambucil has been combined with anti-CD20 monoclonal antibodies. Three prospective studies4–6 and one retrospective7 one investigated the combination of chlorambucil with rituximab (Chl-R) as front-line treatment for elderly CLL patients or for younger patients unsuitable for fludarabine-based therapies. Overall response rates ranging from 66% to 84% have been reported, with complete response rates of 8–26% and progression-free survival from 16.3 to 34.7 months.
In the present GIMEMA study we conducted a retrospective analysis of Chl-R used as front-line treatment in elderly (≥65 years) and/or unfit [Cumulative Illness Rating Scale (CIRS) score >6, calculated before treatment]8 CLL patients treated in 15 different Italian hematology centers. The primary aim was to establish the efficacy and safety of Chl-R and to investigate whether certain CLL subsets could benefit more from this combination. All patients with a minimum follow-up of 12 months and with an Eastern Cooperative Oncology Group (ECOG) score ≤2, treated between 2009 and 2011, were enrolled; their data were collected by treating physicians and inserted into the GIMEMA electronic database.
The treatment schedule differed between centers. The majority of patients (72/102) were treated according to schedules previously reported by Foà et al.5 and Laurenti et al.;7 the remaining patients were treated as reported by Goede et al.6 or with local protocols. Primary endpoints included the overall and complete response rates, evaluated according to the revised International Workshop CLL 2008 criteria9, with the exception of a few patients for whom a computed tomography scan and/or bone marrow biopsy were not available. Secondary endpoints included progression-free survival, time to retreatment, overall survival, and toxicity evaluated according to Common Terminology Criteria for Adverse Events version 4. Responses and outcome were correlated with clinical and biological parameters. For subgroup analyses, patients were classified as high-risk (patients with del17p), intermediate-risk (patients with unmutated IGHV and/or del11q) and low-risk (patients with mutated IGHV without del11q).10–12
Non-parametric tests were carried out for comparisons and logistic regression was performed to adjust for the effect of clinical and biological factors on the overall response rate. Overall response rates were stratified according to the immunophenotypic profile, fluorescence in situ hybridization-based cytogenetic evaluation, IGHV status, ECOG score and age. Survival distributions were estimated using the Kaplan-Meier product limit estimator. Differences in overall survival, progression-free survival and time to retreatment were evaluated using the log-rank test in univariate analyses and the Cox regression model in the adjusted analysis, after assessment of proportionality of hazards. All tests were two-sided, accepting P<0.05 as indicating a statistically significant difference and confidence intervals (CI) were calculated at a 95% level. All analyses were performed using SAS software (release 9.4).
One hundred and two patients (Table 1) were enrolled; 56 out of these 102 patients were already included in previous publications. Three patients discontinued treatment: two because of disease progression and one because of autoimmune hemolytic anemia. The median number of cycles of chlorambucil and rituximab administered was 8 (range, 2–12) and 6 (range, 1–9), respectively. The median total dose of chlorambucil administered during treatment was 600 mg per patient (median dose 90 mg each cycle) and the median dose of rituximab was 4200 mg per patient (median dose 700 mg each cycle). The dose of chlorambucil was reduced in 19% of patients, while rituximab was decreased in only 5% of patients.
Table 1.
Patients’ characteristics and results.
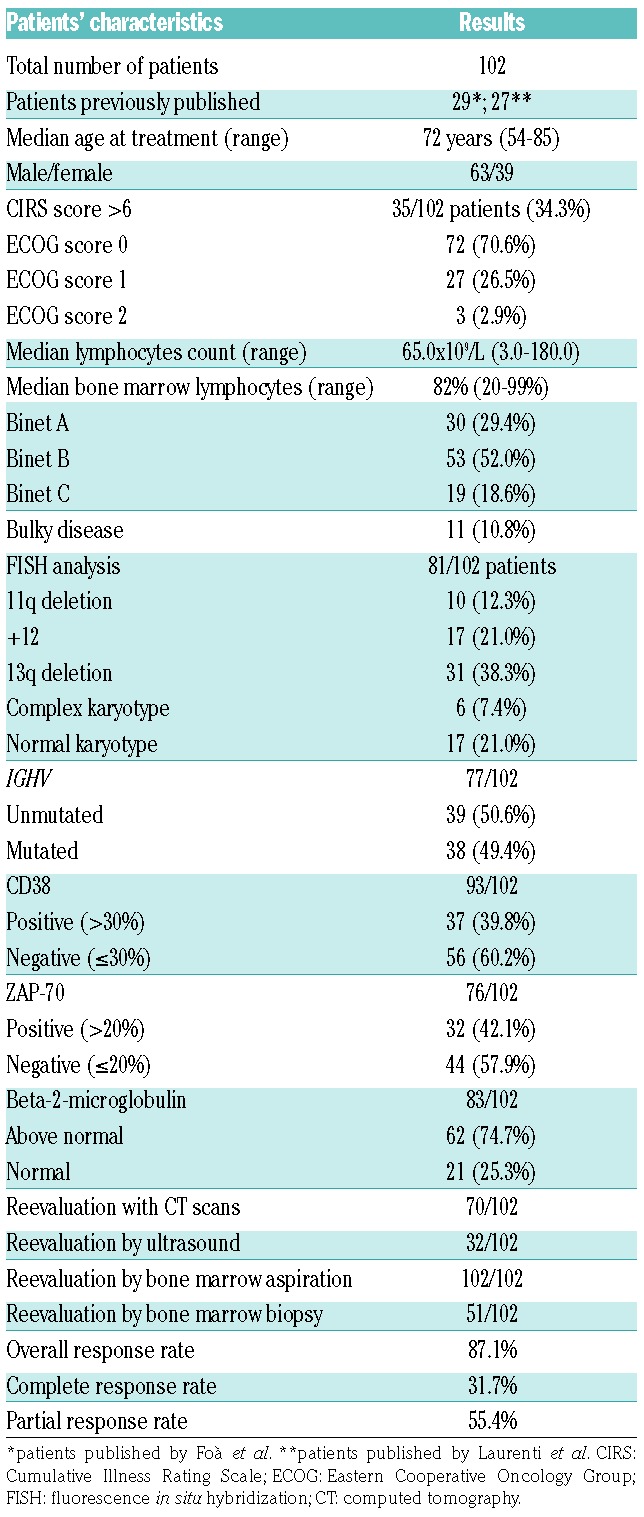
On an intention-to-treat basis, the overall response rate was 87.1%. Thirty-two patients (31.7%) obtained a clinical complete response and 56 patients (55.4%) a partial response (Table 1). No statistically significant differences in overall response rate were noted based on the variables analyzed (Table 2).
Table 2.
Time-dependent results.
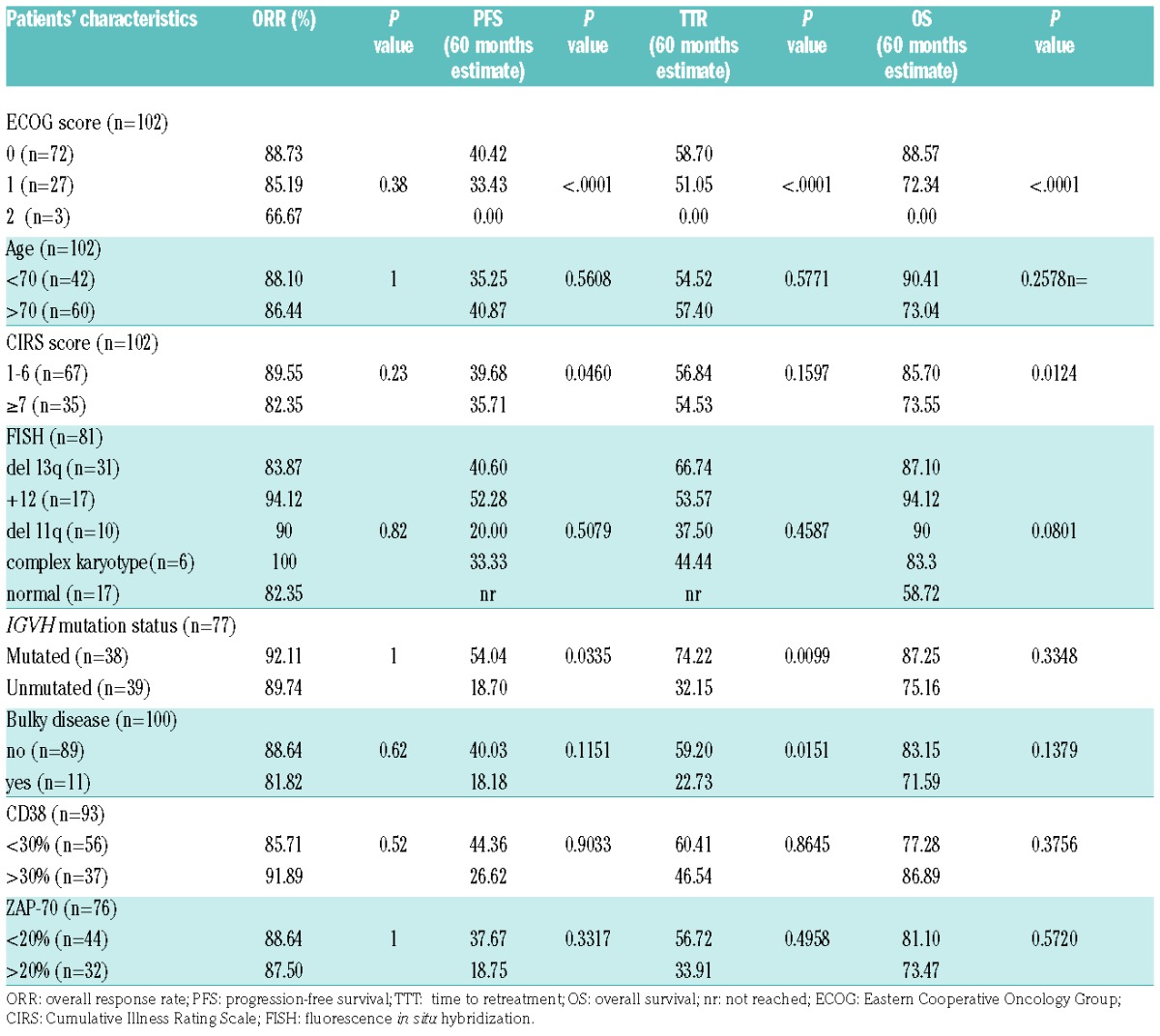
The median progression-free survival was reached at a median time of 43.7 months (Figure 1A). Among 58 patients who experienced progression, 35 (60.3%) received a second line of treatment after a median time of 72.3 months. Among all investigated clinical and biological characteristics, only an ECOG score of 2 (versus ECOG score of 0–1) and IGHV unmutated status (versus IGHV mutated) were bad prognosticators at univariate analysis for progression-free survival and time to retreatment.
Figure 1.

Progression-free survival and overall survival. (A) Progression-free survival (PFS) in the study population. (B) Overall survival (OS) in the study population. (C) PFS in low-risk and intermediate-risk patients. (D) OS in low-risk and intermediate-risk patients.
The median follow-up was 54 months, during which the median overall survival was not reached. Estimated survival rates after 48 and 60 months were 86.1% (95% CI: 79.4–93.5) and 81.2% (95% CI: 72.4–91.2), respectively (Figure 1B). ECOG score of 2 (versus ECOG score of 0–1), CIRS score >6 (versus CIRS score ≤6) and normal karyotype (versus +12 and del13q) showed negative impacts on overall survival at univariate analysis.
The 72 patients with available IGHV and fluorescence in situ hybridization data were classified as intermediate-risk (IGHV unmutated and/or del11q: 36 patients) and low-risk (IGHV mutated without del11q: 36 patients); there were no high-risk patients (del17p). The majority of low-risk patients (54.9%) and only 18.7% of intermediate-risk patients remained free from progression 60 months after treatment; low-risk patients showed a significantly better progression-free survival than intermediate-risk patients: 65.8 months versus 35.2 months (P=0.0116) (Figure 1C). A trend towards a better overall survival was observed, but this has so far not reached statistical significance (Figure 1D).
Forty neutropenic events were reported in 33 patients (32.3%), while anemia and thrombocytopenia were recorded in only three patients. Grade 3–4 neutropenia was reported in 14 patients (13.7%), seven were treated with granulocyte colony-stimulating factor. Two grade 3 pulmonary infections were recorded during the treatment. One patient discontinued treatment because of autoimmune hemolytic anemia and one patient experienced a grade 3 thrombocytopenia. No patient was admitted to hospital, except for the patient with autoimmune hemolytic anemia. Forty episodes of non-hematologic toxicity, mainly grade 1–2, were reported, most involving the respiratory and/or gastrointestinal tracts. Grade 3–4 non-hematologic toxicities were recorded in only ten patients (9.8%). Mild (grade 1–2) infusion-related reactions were reported in 30% of patients, in most cases during the first administration of rituximab. Fifteen patients died during follow-up: six from progressive disease or Richter transformation, six from myocardial infarction or other cardio-pulmonary complications, and three due to a solid tumor (glioblastoma, colon or thyroid cancer) 26, 19 and 14 months after the end of treatment, respectively.
The data presented support the recently reported findings from prospective clinical trials that Chl-R is well tolerated and effective in elderly/unfit CLL patients.4–7 When comparing our results to those of these studies, we wish to underline that our study is observational and characterized by less stringent measures for data collection and absence of central review.
Our results are slightly different from those reported by Hillmen et al.4 and Foà et al.5 with regards to both overall response rate (87.1% versus 84% and 82.4%, respectively) and complete response rate (31.7% versus 10% and 19%, respectively). These differences could be explained by the absence of del17p cases and a lower number of patients (51%) harboring unmutated IGHV genes in our series; in fact, in the studies by Hillmen et al.4 and Foà et al.,5 del17p was present in 3% and 6% of cases, and unmutated IGHV in 59% and 58% of patients, respectively. The higher complete response rate could also be due to the fact that 31% of our patients were evaluated by ultrasound and 50% by bone marrow biopsy, which does not enable identification of nodular partial response, whereas all the patients in the studies by Hillmen et al.4 and Foà et al.5 were evaluated by computed tomography scan.
In the CLL11 GCLLSG trial, Goede et al.6 observed an overall response rate of 65.9% and a complete response rate of 8.3%; these less favorable results are possibly due to the lower cumulative dose of chlorambucil (median dose 400 mg) or to differences in the populations studied (all patients were unfit and 7% of them carried del17p). These differences could also explain the longer median progression-free survival observed in our series compared to those in other studies (43.7 months versus 23.5 months in the study by Hillmen et al.,4 34.7 months in that by Foà et al.,5 and 16.3 months in the one by Goede et al.6).
The Chl-R regimen was well tolerated in all studies, with dose reductions or interruptions being recorded in only 24% of patients in our series and in 25% of patients in the series of Hillmen et al.4 and Foà et al.5 Grade 3–4 neutropenia occurred in 13.7% of our patients and in 19.6%, 28% and 41% of patients in the series reported by Foà et al.,5 Goede et al.,6 and Hillmen et al.,4 respectively. The greater incidence of neutropenia reported by Goede et al. and Hillmen et al. could be related to the greater number of unfit patients6 or the higher chlorambucil dose.4 Serious non-hematologic adverse events were rare in all studies; we observed no grade 3–4 infusion-related reactions, similarly to the other series.4–7
A recent study by Rossi et al.12 showed that CLL patients harboring mutated IGHV genes but neither del11q or del17p have a very low risk and can experience durable remissions after front-line FCR. The impact of IGHV status in patients treated first-line with FCR has been confirmed in two other studies.13,14 Subgroup analysis of the patients investigated in our study showed similar results. These data suggest that the Chl-R protocol is particularly effective for the treatment of elderly or unfit CLL patients with this highly favorable biologically-based prognostic profile.
In conclusion, treatment of elderly or unfit CLL patients with the Chl-R regimen is associated with low toxicity, high overall response rate and durable progression-free survival. Particularly good results are achieved in CLL patients with a mutated IGHV profile not carrying del17p or del11q, suggesting that in this low-risk subset Chl-R could represent a particularly promising therapeutic option, in view of its safety, efficacy and low treatment costs.
Supplementary Material
Footnotes
Funding: this study was partly supported by the Italian Association for Cancer Research (AIRC) Special Program Molecular Clinical Oncology, 5 × 1000, MCO1007 (to RF).
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Hallek M, Fischer K, Fingerle-Rowson G, et al. Addition of rituximab to fludarabine and cyclophosphamide in patients with chronic lymphocytic leukaemia: a randomised, open-label, phase 3 trial. Lancet. 2010;376(9747):1164–1174. [DOI] [PubMed] [Google Scholar]
- 2.Eichhorst B, Goede V, Hallek M. Treatment of elderly patients with chronic lymphocytic leukemia. Leuk Lymphoma. 2009;50(2):171–178. [DOI] [PubMed] [Google Scholar]
- 3.Eichhorst BF, Busch R, Stilgenbauer S, et al. First-line therapy with fludarabine compared with chlorambucil does not result in a major benefit for elderly patients with advanced chronic lymphocytic leukemia. Blood. 2009;114(16):3382–3391. [DOI] [PubMed] [Google Scholar]
- 4.Hillmen P, Gribben JG, Follows GA, et al. Rituximab plus chlorambucil as first-line treatment for chronic lymphocytic leukemia: final analysis of an open-label phase II study. J Clin Oncol. 2014; 32(12):1236–1241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Foà R, Del Giudice I, Cuneo A, et al. Chlorambucil plus rituximab with or without maintenance rituximab as first-line treatment for elderly chronic lymphocytic leukemia patients. Am J Hematol. 2014; 89(5):480–486. [DOI] [PubMed] [Google Scholar]
- 6.Goede V, Fischer K, Bosch F, et al. Updated survival analysis from the CLL11 study: obinutuzumab versus rituximab in chemoimmunotherapy-treated patients with chronic lymphocytic leukemia. Abstract ASH 2015. Blood. 2015;126:1733.26450950 [Google Scholar]
- 7.Laurenti L, Vannata B, Innocenti I, et al. Chlorambucil plus rituximab as front-line therapy in elderly/unfit patients affected by B-cell chronic lymphocytic leukemia: results of a single-centre experience. Mediterr J Hematol Infect Dis. 2013;5(1):e2013031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Miller MD, Paradis CF, Houck PR, et al. Rating chronic medical illness burden in geropsychiatric practice and research: application of the Cumulative Illness Rating Scale. Psychiatry Res. 1992;41(3):237–248. [DOI] [PubMed] [Google Scholar]
- 9.Hallek M, Cheson BD, Catovsky D, et al. Guidelines for the diagnosis and treatment of chronic lymphocytic leukemia: a report from the International Workshop on Chronic Lymphocytic Leukemia updating the National Cancer Institute-Working Group 1996 guidelines. Blood. 2008;111(12):5446–5456. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Döhner H, Stilgenbauer S, Benner A, et al. Genomic aberrations and survival in chronic lymphocytic leukemia. N Engl J Med. 2000; 343(26):1910–1916. [DOI] [PubMed] [Google Scholar]
- 11.Hamblin TJ, Davis Z, Gardiner A, et al. Unmutated Ig V(H) genes are associated with a more aggressive form of chronic lymphocytic leukemia. Blood. 1999;94(6):1848–1854. [PubMed] [Google Scholar]
- 12.Rossi D, Terzi-di-Bergamo L, De Paoli L, et al. Molecular prediction of durable remission after first-line fludarabine - cyclophosphamide -rituximab in chronic lymphocytic leukemia. Blood. 2015; 126(16):1921–1924. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Fischer K, Bahlo J, Fink AM, et al. Long-term remissions after FCR chemoimmunotherapy in previously untreated patients with CLL: updated results of the CLL8 trial. Blood. 2016;127(2):208–215. [DOI] [PubMed] [Google Scholar]
- 14.Jain N, O’Brien S. Targeted therapies for CLL: Practical issues with the changing treatment paradigm. Blood Rev. 2016;30(3):233–244. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.