

Abstract
Immunoglobulin G4-related systemic disease (IgG4-RSD) is a recently emerging disorder characterized by swelling lesions with storiform fibrosis and lymphoplasmacytic infiltration enriched with IgG4-positive plasma cells. IgG4-RSD has been found in multiple organs/tissues. The diagnosis requires the integration of clinical, serological, imaging, histopathological, and immunohistological features. The 2-[18F]-fluoro-2-deoxy-D-glucose–positron emission tomography/computed tomography (18F-FDG PET/CT) enables the acquisition of whole-body images and provides functional information about disease activity. However, its current role in IgG4-RSD is not well established in clinical practice. In our case, we studied a patient with systemic symptoms, submaxillary adenopathy, and imaging explorations that initially guided toward a lymphoproliferative process. However, the differential diagnosis with an autoimmune systemic disease type IgG4 was considered because of elevated levels of serum immunoglobulins. The study was completed with 18F-FDG PET/CT that not only allowed us to assess the extension disease and to locate the best lesion for biopsy but also allowed us to evaluate the response to treatment and to diagnose the suspicion of recurrence. In this case, PET/CT shows its usefulness in clinical practice.
Keywords: Immunoglobulin G4 related systemic disease, 2-18F-FDG PET CT, Steroid therapy response
Introduction
Immunoglobulin G4-related systemic disease (IgG4-RSD) is a recently defined disorder with a diffuse mass-forming inflammatory reaction. The mass could be solitary or multiple. This entity affects the exocrine glands, lymph nodes, and extranodal tissues, with lymphocytes and high IgG4-secreting plasma cells infiltrate, fibrosclerosis, and obliterating phlebitis, which affect medium- and small-caliber veins. The elevation of serum IgG4 is often present, but not always (1–3).
Epidemiology is partially unknown, because a considerable number of patients probably remain undiagnosed. It is more prevalent in males, in their fifth and sixth decades of life (4).
Clinical manifestations are highly variable as there may be focal or multi-organ involvement (with a synchronous or metachronous pattern): meninges, orbital tissue, salivary glands, thyroid, lungs, pericardium, pancreas, hepatobiliary tract, kidneys, lymph nodes (up to 80% of cases), aorta, retroperitoneum, prostates, breasts, and skin. Two of the most common characteristics are the presence of a mass or localized inflammation and a history of allergic diseases (1, 2, 4).
Diagnosis requires the integration of clinical, serological, imaging, histopathological, and immunohistological features (3, 5, 6).
The diagnostic criteria, as defined by Okazaki et al. (3), are as follows:
Clinical exam with characteristic diffuse/localized swelling or masses in single or multiple organs.
Hematological test with elevated serum IgG4 concentrations (≥135 mg/dL).
-
Histopathological exam:
- Marked lymphocyte and plasmacyte infiltration and fibrosis
- Infiltration of IgG4-positive plasma cells: ratio of IgG4/IgG positive cells >40% and >10 IgG4-positive plasma cells/HPF.
Definite diagnosis: (1)+(2)+(3); Probable diagnosis: (1)+(3); Possible diagnosis: (1)+(2).
The 18F-FDG PET/CT permits the acquisition of whole-body images and provides metabolic information about the disease activity. It is a useful tool in the assessment of disease extension, location of the lesion for biopsy, and follow-up responses to treatment. However, its current role in clinical practice is not well established.
Treatment is based on high-dose glucocorti-costeroids with subsequent de-escalation. This treatment is usually effective at the beginning, but disease flares are common (7, 8).
Case Presentation
A 56-year-old woman with hypertension, obesity, asthma, kidney stones, and subclinical hypothyroidism was enrolled, who reported weight loss not quantified in the latest months with anorexia and discomfort in the right upper abdominal quadrant.
A nodule in the right thyroid lobe and another in the left submandibular gland was seen in a neck ultrasound performed in her thyroid disease follow-up. The study was completed with a cervical CT that showed a replacement of the parotid gland tissue with adipose tissue. Laboratory tests showed elevated serum levels of acute phase reactants, rheumatoid factor, hypertransaminasemia, dissociated cholestasis pattern, and positives antinuclear antibodies.
Increased bile duct size and a pseudonodular hypoechoic lesion in the pancreatic head were seen in the abdominal ultrasound, both of which are suggestive of a possible proliferative lesion.
A thoracic–abdominal CT was performed, showing multiple abdominal and pelvic lymph nodes (periportal, celiac, retroperitoneal, common, and external iliac territories—more toward the left) involving left ureter and pancreatic head. In addition, mild hepatic steatosis was shown.
Due to the suspicion of a lymphoproliferation process or an IgG4-RSD, an 18F-FDG PET/CT (64-slice CT scanner, Siemens) was performed. It showed a high 18F-FDG uptake and an increase in size in the cervical, supradiaphragmatic, and infradiaphragmatic adenopathies. On the other hand, it also showed bilateral involvement in parotid and submaxillary glands and involvement in pancreas, pleura, and left adrenal gland, expanding the information provided by CT and ultrasound. The above findings are compatible with IgG4-RSD due to the distribution of the affected organs (lymph nodes, bilateral salivary glands, pancreas, etc.). The submandibular lymph nodes were the most accessible for biopsy (Figure 1–4).
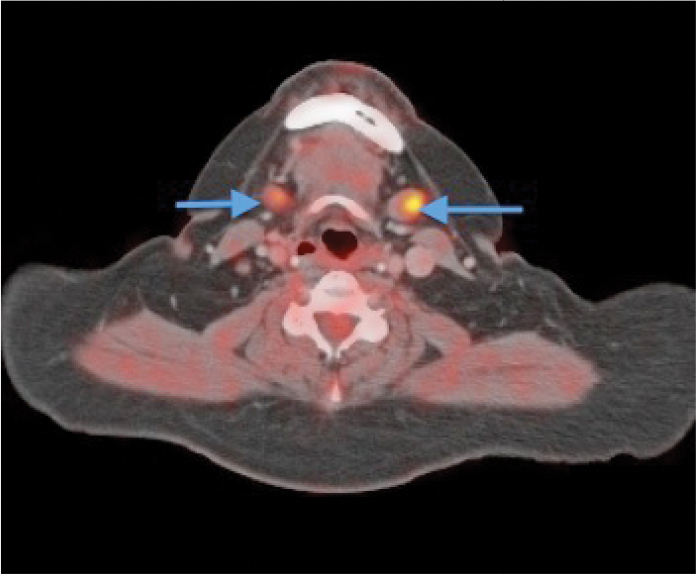
Figure 1.

Fusion 18F-FDG PET/CT axial slices before biopsy and glucocorticoids treatment. There is multi-organ synchronic involvement with increased uptake in the sublingual glands (blue arrows)
18F-FDG PET/CT: 2-[18F]-fluoro-2-deoxy-D-glucose–positron emission tomography/computed tomography
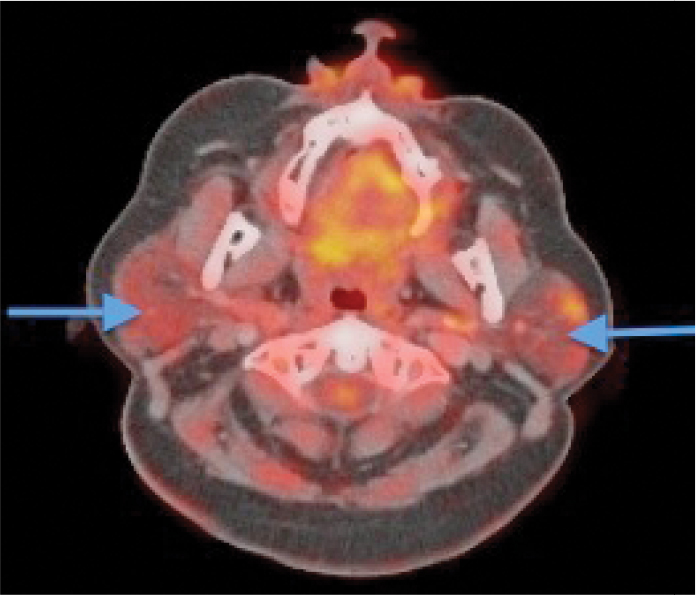
Figure 2.

Fusion 18F-FDG PET/CT axial slices before biopsy and glucocorticoids treatment. There is multi-organ synchronic involvement with increased uptake in the parotids glands (blue arrows)
18F-FDG PET/CT: 2-[18F]-fluoro-2-deoxy-D-glucose–positron emission tomography/computed tomography
Figure 3.
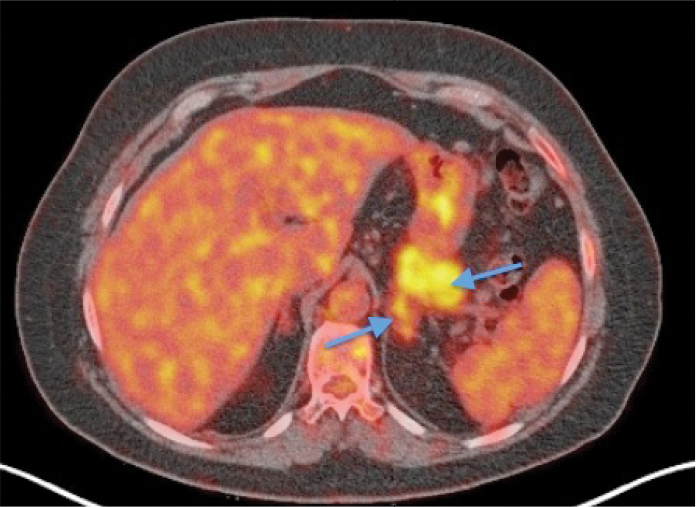
Fusion 18F-FDG PET/CT axial slices before biopsy and glucocorticoids treatment. There is multi-organ synchronic involvement with increased uptake in the pancreas and left adrenal gland (blue arrows)
18F-FDG PET/CT: 2-[18F]-fluoro-2-deoxy-D-glucose–positron emission tomography/computed tomography
Figure 4.
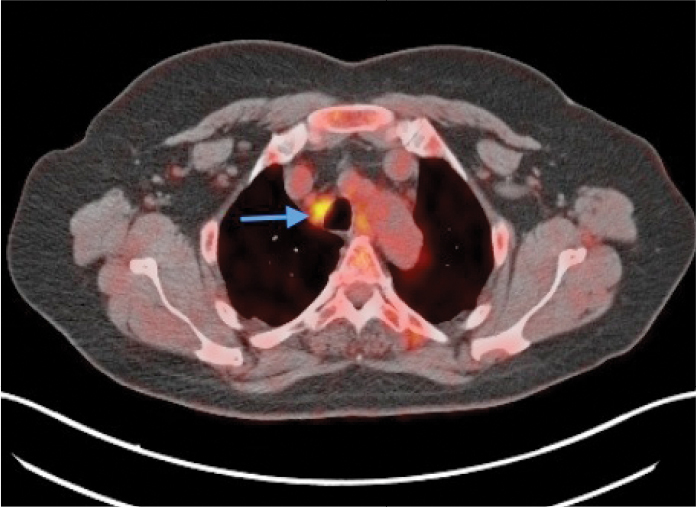
Fusion 18F-FDG PET/CT axial slices before biopsy and glucocorticoids treatment. There is multi-organ synchronic involvement with increased uptake in the mediastinal node “right upper paratracheal” (blue arrow)
18F-FDG PET/CT: 2-[18F]-fluoro-2-deoxy-D-glucose–positron emission tomography/computed tomography
Immunological study reported high levels of total immunoglobulins: 2012 mg/dL (N: 700–1600), IgG4: 798 mg/dL (N: 5–156).
A cervical adenopathy biopsy was performed. Histopathological findings showed an elevated number of mature plasma cells with an IgG4+/IgG+ plasma cell ratio >50% and the presence of numerous IgG4-positive plasma cells in the germinal zone without pathological lymphoid population.
According to these findings, the patient was diagnosed as having IgG4-RSD, following which oral glucocorticoids therapy was initiated. Patient’s symptoms improved immediately and the serum IgG4 levels were normalized. Furthermore, 18F-FDG PET/CT after 4 months of treatment showed that cervical, mediastinal, retroperitoneal lymph nodes, and visceral involvement (parotid and pancreas) had disappeared almost completely, indicating a good response to treatment (Figure 5–8).
Figure 5.

Fusion 18F-FDG PET/CT axial slices in follow-up after glucocorticoids treatment. There is no uptake of 18F-FDG in the sublingual glands (blue arrows)
18F-FDG PET/CT: 2-[18F]-fluoro-2-deoxy-D-glucose–positron emission tomography/computed tomography
Figure 6.

Fusion 18F-FDG PET/CT axial slices in follow-up after glucocorticoids treatment. There is no uptake of 18F-FDG in the parotids glands (blue arrows)
18F-FDG PET/CT: 2-[18F]-fluoro-2-deoxy-D-glucose–positron emission tomography/computed tomography
Figure 7.
Fusion 18F-FDG PET/CT axial slices in follow-up after glucocorticoids treatment. There is no uptake of 18F-FDG in the pancreas (blue arrow) and left adrenal gland, which has a persistent low uptake (yellow arrow)
18F-FDG PET/CT: 2-[18F]-fluoro-2-deoxy-D-glucose–positron emission tomography/computed tomography
Figure 8.
Fusion 18F-FDG PET/CT axial slices in follow-up after glucocorticoids treatment. There is no uptake of 18F-FDG in the mediastinal node “right upper paratracheal” (blue arrow)
18F-FDG PET/CT: 2-[18F]-fluoro-2-deoxy-D-glucose–positron emission tomography/computed tomography
Six months after decreasing glucocorticoids treatment, the patient showed an asymptomatic increase in the transaminases levels, but normal levels of IgG and IgG4 were maintained. Because of a disease reactivation suspicion, another 18F-FDG PET/CT was performed (6 months after the first control), showing an elevated 18F-FDG uptake in the parotid glands and submandibular glands and also in the laterocervical and mediastinal lymph nodes. Another finding was important hepatic steatosis (not seen in the previous study) without pancreatic involvement (Figure 9–12).
Figure 9.
Fusion 18F-FDG PET/CT axial slices performed due to suspicion of IgG4-RSD recurrence with normal levels of immunoglobulins. There is increased 18F-FDG uptake in the sublingual glands (blue arrows)
18F-FDG PET/CT: 2-[18F]-fluoro-2-deoxy-D-glucose–positron emission tomography/computed tomography
Figure 10.
Fusion 18F-FDG PET/CT axial slices performed due to suspicion of IgG4-RSD recurrence with normal levels of immunoglobulins. There is increased 18F-FDG uptake in the parotids glands (blue arrows)
18F-FDG PET/CT: 2-[18F]-fluoro-2-deoxy-D-glucose–positron emission tomography/computed tomography
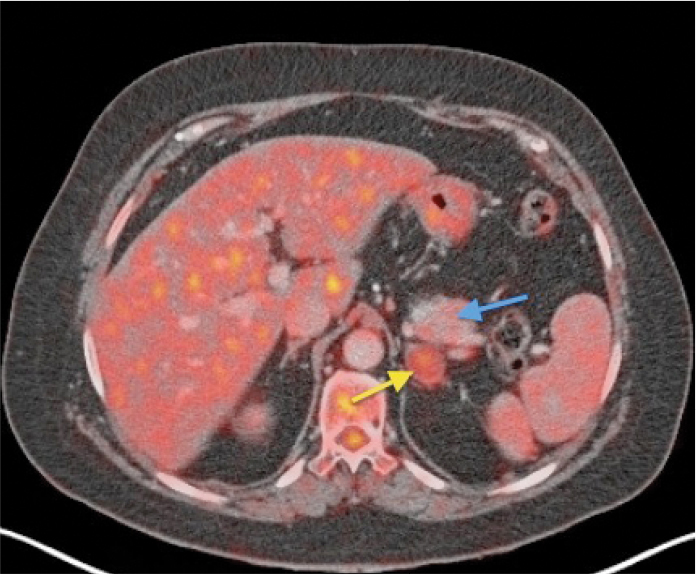
Figure 11.

Fusion 18F-FDG PET/CT axial slices performed due to suspicion of IgG4-RSD recurrence with normal levels of immunoglobulins. There is increased 18F-FDG uptake in the left adrenal gland (yellow arrow) and pancreas with no uptake (blue arrow)
18F-FDG PET/CT: 2-[18F]-fluoro-2-deoxy-D-glucose–positron emission tomography/computed tomography
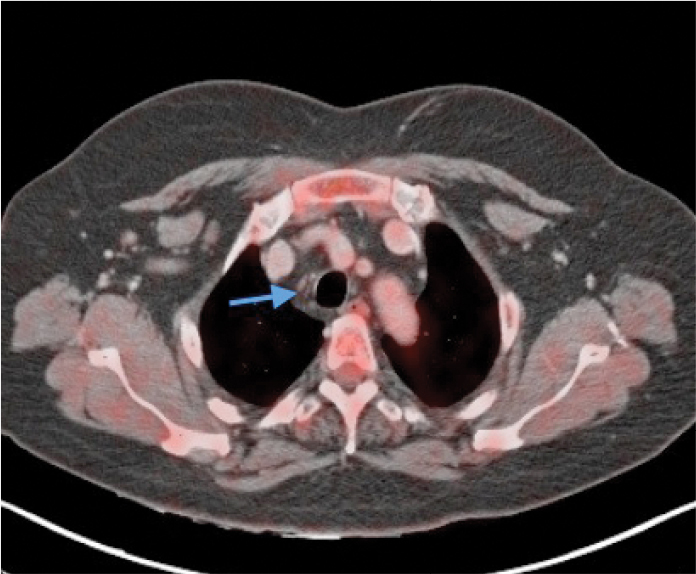
Figure 12.

Fusion 18F-FDG PET/CT axial slices performed due to suspicion of IgG4-RSD recurrence with normal levels of immunoglobulins. There is a low increase of 18F-FDG uptake in the mediastinal node “right upper paratracheal” (blue arrow)
18F-FDG PET/CT: 2-[18F]-fluoro-2-deoxy-D-glucose–positron emission tomography/computed tomography
After confirming the recurrence, it was decided to start biological treatment.
Discussion
This case described above is a difficult patient diagnosis in which the first clinical and imaging explorations (ultrasound and CT) guided toward a lymphoproliferative syndrome. However, when 18F-FDG PET/CT was performed, the tracer extranodal distribution was not expected in this diagnosis. The presence of high IgG4 levels and others findings in 18F-FDG PET/CT allowed the diagnosis of IgG4-RSD, which was later confirmed by biopsy.
According to literature, we observed that in our case, multi-organ involvement in IgG4-RSD showed in 18F-FDG PET/CT, highlighting the involvement of typical organs such as the pancreas, salivary glands, adrenals, and lymph nodes.
Initial 18F-FDG PET/CT helped the differential diagnosis with other processes, assessed the disease extension, and was also useful to localize an appropriate site for biopsy.
Another important advantage of 18F-FDG PET/CT was its usefulness in the follow-up of treatment response and the diagnostic suspicion of IgG4-RSD recurrence because some patients may be asymptomatic and with normal immunoglobulin levels, but they could have a disease relapse (as in our case report).
In conclusion, IgG4-RSD remains difficult to diagnose due to its extensive spectrum of presentation. Nowadays, 18F-FDG PET/CT does not have a well-established role in the appraisal of patients with IgG4-RSD, but in combination with the diagnostic criteria, it allows us to diagnose the disease. Further, it assists in the biopsy site selection, staging, and distribution of the disease. Additionally, it helps in the follow-up of the treatment response and diagnostic suspicion of recurrence.
Footnotes
Ethics Committee Approval: N/A.
Informed Consent: Written informed consent was obtained from the patient who participated in this study.
Peer-review: Externally peer-reviewed.
Author Contributions: : Concept - M.P., N.A., S.P.; Design - M.P., N.A., S.P.; Supervision - M.P., N.A., S.P.; Resources - M.P., N.A., S.P.; Materials - M.P., N.A., S.P.; Data Collection and/or Processing - M.P., N.A., S.P.; Analysis and/ or Interpretation - M.P., N.A., S.P.; Literature Search - M.P., N.A., S.P.; Writing Manuscript - M.P., N.A.
Conflict of Interest: No conflict of interest was declared by the authors.
Financial Disclosure: The authors declared that this study has received no financial support.
References
- 1.Campos J, Méndez C, Mulero J. Immunoglobulin G4-related systemic disease: why does it interest rheumatologists? Semin Fund Esp Reumatol. 2013;14:2–7. [Google Scholar]
- 2.Ebbo M, Grados A, Guedj E, Gobert D, Colavolpe C, Zaidan M, et al. Usefulness of 2-[18F]-fluoro-2-deoxy-D-glucose–positron emission tomography/ computed tomography for staging and evaluation of treatment response in IgG4-related disease: a retrospective multicenter study. Arthritis Care Res. 2014;66:86–96. doi: 10.1002/acr.22058. https://doi.org/10.1002/acr.22058. [DOI] [PubMed] [Google Scholar]
- 3.Okazaki K, Umehara H. Are classification criteria for IgG4-RD now possible? The concept of IgG4-related disease and proposal of comprehensive diagnostic criteria in Japan. JR. 2012;35:70–1. doi: 10.1155/2012/357071. https://doi.org/10.1002/acr.22058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Nakatani K, Nakamoto Y, Togashi K. Utility of FDG PET/CT in IgG4-related systemic disease. Clin Radiol. 2012;67:297–305. doi: 10.1016/j.crad.2011.10.011. https://doi.org/10.1155/2012/357071. [DOI] [PubMed] [Google Scholar]
- 5.Carruthers M, Stone J, Khosroshahi A. The latest on IgG4-RD: a rapidly emerging disease. Curr Opin Rheumatol. 2012;24:60–9. doi: 10.1097/BOR.0b013e32834ddb4a. https://doi.org/10.1097/BOR.0b013e32834ddb4a. [DOI] [PubMed] [Google Scholar]
- 6.Deshpande V, Zen Y, Chan JK, Yi EE, Sato Y, Yoshino T, et al. Consensus statement on the pathology of IgG4 related disease. Mod Pathol. 2012;25:1181–92. doi: 10.1038/modpathol.2012.72. https://doi.org/10.1038/modpathol.2012.72. [DOI] [PubMed] [Google Scholar]
- 7.Zhang J, Chen H, Ma Y, Xiao Y, Niu N, Lin W, et al. Characterizing IgG4-related disease with 18F-FDG PET/CT: a prospective cohort study. Eur J Nucl Med Mol Imaging. 2014;41:1624–34. doi: 10.1007/s00259-014-2729-3. https://doi.org/10.1007/s00259-014-2729-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Stone JH, Zen Y, Deshpande V. IgG4-related disease. N Engl J Med. 2012;366:539–5. doi: 10.1056/NEJMra1104650. https://doi.org/10.1056/NEJMra1104650. [DOI] [PubMed] [Google Scholar]