

Abstract
The Great East Japan Earthquake was a major earthquake, one of the largest (Magnitude 9.0) in Japan since 1900. 18 997 human lives were lost in the subsequent tsunami around the Sanriku coast of eastern Japan. Ishinomaki City, which was close to the epicenter, is one of the greatest locations that experienced of the greatest loss of human life: 3819 people. The Ishinomaki Red Cross Hospital (IRCH), which is the main trunk hospital of the Ishinomaki medical sphere, moved to a hill away from the Pacific Ocean in order to avoid future tsunami 5 years prior to the Great East Japan Earthquake. IRCH was therefore nearly intact and its functions were maintained after the Great East Japan Earthquake. Other neighboring medical facilities were in a catastrophic state; for emergency, patients were all concentrated at the IRCH, and the medical staff of IRCH became exhausted. In response, the Japanese Red Cross Society collected and transported physicians, nurses, pharmacists, medical engineers, and medical clerks, to IRCH from Red Cross hospitals across the country during the period of April to August 2011. The dispatched medical personnel operated a makeshift clinic on a rotating basis autonomously in the hospital to support the IRCH. In this temporary clinic, the primary and secondary emergency staff conducted the center's general practice.
Keywords: disaster medicine, general physician, the Great East Japan Earthquake
1. INTRODUCTION
Japan is located in the Pacific Rim area and is a country that experiences many earthquakes. It is well known that the word tsunami a high large wave that is caused by large earthquakes comes from the Japanese language. The Great East Japan Earthquake (magnitude: 9.0) happened on March 11, 2011, with 18 997 casualties. Many of the people were probably instantly taken away by the tsunami. This earthquake was the fourth largest in the world on record since 1900 (Table 1).1 To this day, many residents have been unable to come to a solution to the accident Fukushima Daiichi nuclear power plant accident caused by the tsunami wave, and they have requested relocation.
Table 1.
Largest earthquake in the world since 1900
| Location | Date UTC | Magnitude | Lat. | Long. | References | |
|---|---|---|---|---|---|---|
| 1. | Chile | 1960 05 22 | 9.5 | −38.29 | −73.05 | Kanamori, 1977 |
| 2. | Prince William Sound, Alaska | 1964 03 28 | 9.2 | 61.02 | −147.65 | Kanamori, 1977 |
| 3. | Off the West Coast of Northern Sumatra | 2004 12 26 | 9.1 | 3.30 | 95.78 | Park et al., 2005 |
| 4. | Near the East Coast of Honshu, Japan | 2011 03 11 | 9.0 | 38.322 | 142.369 | PDE |
| 5. | Kamchatka | 1952 11 04 | 9.0 | 52.76 | 160.06 | Kanamori, 1977 |
| 6. | Offshore Maule, Chile | 2010 02 27 | 8.8 | −35.846 | −72.719 | PDE |
| 7. | Off the Coast of Ecuador | 1906 01 31 | 8.8 | 1.0 | −81.5 | Kanamori, 1977 |
| 8. | Rat Islands, Alaska | 1965 02 04 | 8.7 | 51.21 | 178.50 | Kanamori, 1977 |
| 9. | Northern Sumatra, Indonesia | 2005 03 28 | 8.6 | 2.08 | 97.01 | PDE |
| 10. | Assam ‐ Tibet | 1950 08 15 | 8.6 | 28.5 | 96.5 | Kanamori, 1977 |
2. EARTHQUAKES AND TSUNAMIS IN JAPAN
The tsunami undulation that occurs after a big earthquake happens in a moment; the life of all creatures is dredged and the buildings and topography are destroyed. Japan is an island chain nations, a contact center through the sea to its neighboring countries, is mountainous, and has a history of many people having lived in the vicinity of its coast since time immemorial. In addition, from record written in ancient documents and on stele, it is clear that Japan received extensive damage caused by tsunamis during ancient times. Particularly, the area from the Sanriku Coast, to the Oshika Peninsula (Miyagi), to Hachinohe (Aomori) reveals a sawtooth coastline, like a fractal, caused by erosion from sea waves.
In Japan, since 1900, the Meiji Sanriku Earthquake (1896, magnitude: 8.2, and 21 959 dead), the Great Kanto Earthquake (1923, magnitude: 7.9, and 105 000 dead), the Showa Sanriku Earthquake (1933, magnitude: 8.1, and dead: 3064), and the recent Great Hanshin‐Awaji Earthquake (1995, magnitude: 7.3, and 18 997 dead) were especially large earthquakes (Figure 1). Many of the dead of the Great Kanto Earthquake were burned to death, and this was also the case with the Great Hanshin Earthquake. The cause of death was predominantly drowning by tsunami in the Meiji Sanriku Earthquake, the Showa Sanriku Earthquake, and the Great East Japan Earthquake.
Figure 1.
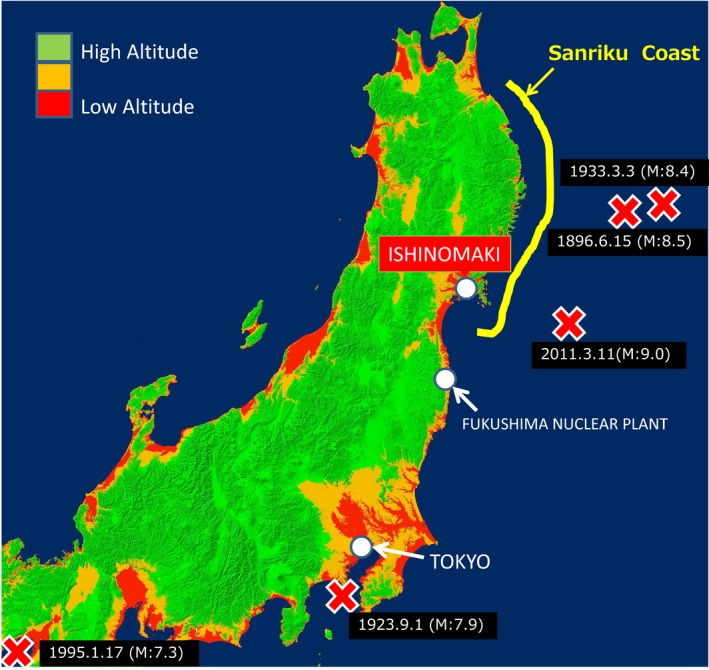
Great Earthquakes map in eastern Japan. Designed by Katsunori Goto
3. ISHINOMAKI RED CROSS HOSPITAL
At IRCH near the epicenter of the Great East Japan Earthquake, the medical function was completely retained because the hospital had moved to a location away from the Pacific Ocean after foreseeing the risk of a large tsunami 5 years prior to the Great East Japan Earthquake (Figure 2). However, medical dependence upon the IRCH rose greatly, and it became functionally impoverished because so many other facilities had destroyed.
Figure 2.
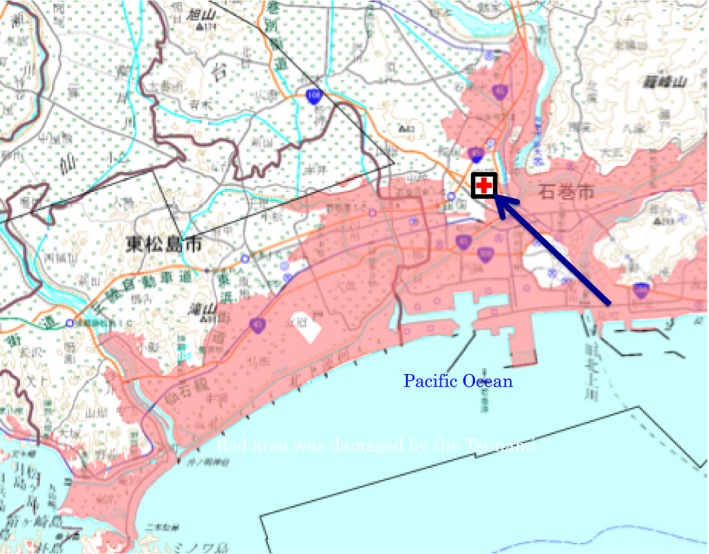
Ishinomaki Red Cross Hospital had moved to a place away from the sea, forecasting the tsunami three years ago, so it was intact even if damaged by the Great East Japan Earthquake
4. DISASTER MEDICAL ASSISTANCE TEAM
Owing to lessons learned in the tragedy of the Great Hanshin‐Awaji Earthquake in Japan, the Disaster Medical Assistance Team (DMAT) was established in 2004. The DMAT comprises disaster medical experts from several professions, including doctors, to be dispatched to disaster areas during the acute phase. The DMAT has contributed to disaster medical care as well as to training and study. Although immediately following the Great East Japan Earthquake, more than 340 DMATs provided relief efforts in the affected areas, a large number of deaths had already been caused by the large tsunami at the time of the DMAT's arrival. Many people had been washed away to sea. Therefore, the premise is that DMAT can perform its duties effective when there are survivors after a disaster, for example, cases such as the Great Hanshin Earthquake might be typical.
5. JAPAN SELF‐DEFENSE FORCES
There were noteworthy things regarding activities of the Japanese Self‐Defense Forces (JSDF), which supplied high support consistently in not only the acute but also the chronic phase. The JSDF dispatched personnel to a total of 10 million members, saving the lives of 19 286 people: The remaining housing spans 9505 people.2 The JSDF has continued disaster relief activities by being continuously stationed in Ishinomaki City.
6. PRIMARY CARE FOR ALL TEAM
The Japanese Primary Care Association Society, having the five medical ideals of “Accessibility,” “Comprehensiveness,” “Coordination,” “Continuity,” and “Accountability,” organized the Primary Care for All Team (PCAT) and also developed chronic comprehensive medical treatment in the disaster‐stricken areas. The correct mobilization number is not available because the presence other medical support made it difficult to fully grasp the active situation at a different central head office.
7. THE JAPANESE RED CROSS SOCIETY (JRCS)
The JRCS is listed as a Designated Public Corporation under the Disaster Countermeasures Basic Act for the four purposes of medical relief, stockpiling and distribution of relief supplies, provision of blood products, and collection of donation.3
One month later, the JRCS brought physicians, nurses, pharmacists, medical engineers, and clerks from the Red Cross Hospitals across the country to the headquarters of the JRCS in Tokyo, and it began a project to dispatch them on a rotating basis to the IRCH by bus over a period of 6 hours in order to support the IRCH in maintaining functions. Because the dispatched medical physicians, nurses, and clerks operated a temporary clinic within IRCH autonomously, performing the medical care of mainly ambulatory patients (primary emergency‐secondary emergency), it became possible for the medical staff of the IRCH to be devoted to ambulance care (tertiary emergency) (Figure 3).
Figure 3.
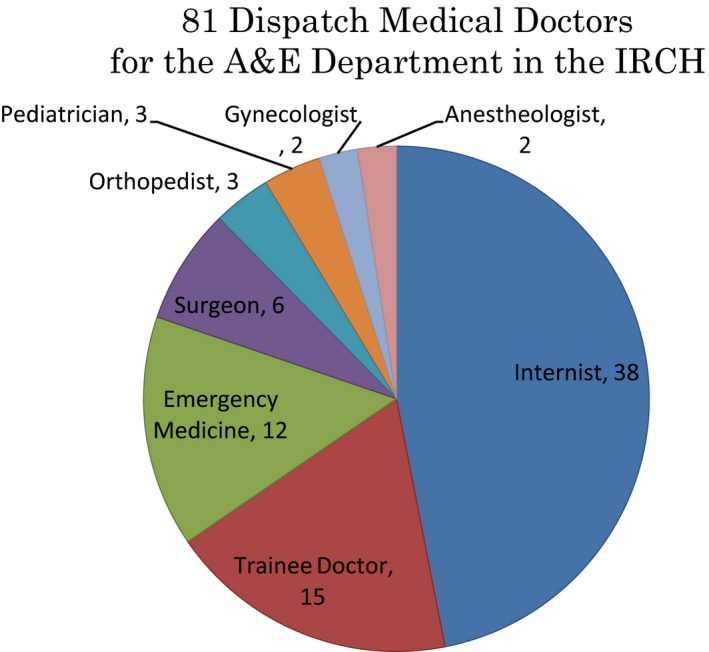
Breakdown of 81 dispatched physicians for the IRCH
This project involved a total of 81 emergency medical support doctors who were dispatched from April to August 2011. The breakdown of the doctors was as follows: 38 internal physicians, 15 medical trainers, 12 emergency physicians, six surgeons, three pediatricians, three plastic surgeons, two anesthesiologists, and two obstetrician‐gynecologists. Six doctors were stationed in IRCH for 6 days at first, and they initially provided first aid: Then I came into action and laid out a shift system complementarily (Figure 4).
Figure 4.

The first dispatch team to IRCH consisted of three physicians, two anesthesiologists and one pediatrician
There were bone fractures, surgeries, early stage treatments of injuries, infant diseases, and psychological diseases caused by the earthquake disaster, tidal wave, and radiation accident (PTSD), which required medical examination and treatment which passes to all subject. Additionally, 20 psychiatrists and 12 ward support doctors who treat PTSD were dispatched. Additionally, 372 nurses, 105 pharmacists, 25 engineers, and 113 clerical workers were dispatched. This project helped with rehabilitation in the Ishinomaki medical care zone.4, 5, 6
8. CONCLUSION
Because the needs for assistance in disaster medical care are diverse, we must have both axes of expertise and comprehensiveness. Particularly during the chronic phase, comprehensive care and cures are required that are tailored to a variety of pathological conditions of diverse patients, including children, the elderly, and sometimes pregnant women and mental health patients.
If possible, given the inevitable occurrence of earthquakes and tsunamis in Japan, medical institutions and nuclear power plants should be remotely located from the areas likely to experience the effects of the tsunami so that they can safely maintain their functions. Among the affected and destroyed public hospitals, Minamisanriku Hospital was moved to higher ground the soonest on December 4, 2015, and with economic assistance from the Taiwan Red Cross Society, it was reopened.7
9. CONFLICT OF INTEREST
The authors have stated explicitly that there are no conflicts of interest in connection with this article.
Hata T. The comprehensive role of general physicians is very important in the chronic phase of a disaster area: Beyond and after the Great East Japan Earthquake. J Gen Fam Med. 2017;18:212–216. https://doi.org/10.1002/jgf2.65
This report was presented at the American College of Physicians (ACP) Japan annual meeting in 2015 at Kyoto University, and it has been recommended as a paper to be published by the ACP Japan.
REFERENCES
- 1. Magnitude 8 and More Earthquakes since 1900. U.S. Geological. http://earthquake.usgs.gov/earthquakes/eqarchives/year/mag8/magnitude8_1900_date.php (accessed 5 April 2017).
- 2. The Great East Japan Earthquake. Ministry of Defense Homepage. http://www.mod.go.jp/e/d_act/disaster/index.html (accessed 5 April 2017).
- 3. Domestic Disaster Response. The Japanese Red Cross Society Homepage. www.jrc.or.jp/english/activity/domestic/ (accessed 5 April 2017).
- 4. Toshihiko H. Support provided on behalf of various Japanese Red Cross Society facilities to Ishinomaki Red Cross Hospital after the Great East Japan Earthquake: Project participant report. 10–12, Dec 2011. Governor's Newsletter for all ACP members. http://acpjc.naika.or.jp/jpnchap/pdf/gnewsE_Dec2011.pdf (accessed 5 April 2017).
- 5. Toshihiko H, Ken U, Human S, Takashi S, Hiroshi M, Hiroki T. Alternating Medical Dispatch Support Provided by the Japanese Red Cross Society after the Great East Japan Earthquake. The Journal of Academic Emergency Medicine. 2013;12:54–56. [Google Scholar]
- 6. Toshihiko H. Medical Support by the Japanese Red Cross Society to Survived Isinomaki Red Cross Hospital After the Great East Japan Earthquake. Indian Journal of Research. 2014;3:97–100. [Google Scholar]
- 7. Bereaved husband hails tsunami‐hit hospital's reopening. November 25, 2015. The Asahi Simbun. Asia & Japan Watch. http://ajw.asahi.com/article/0311disaster/life_and_death/AJ201511250069 (accessed 5 April 2017).