

Supplemental Digital Content is available in the text
Keywords: acute kidney injury, coronary artery bypass grafting, off-pump, on-pump
Abstract
Acute kidney injury (AKI) after coronary artery bypass grafting (CABG) is associated with a less favorable outcome. Off-pump surgery results in lower kidney dysfunction than conventional on-pump arrest surgery. On-pump arrest surgery results in a lower revascularization rate compared with off-pump surgery. On-pump beating heart (OPBH) CABG combines the advantages of beating heart surgery and cardiopulmonary bypass. This study compared the renal outcomes of 3 cardiac surgical methods. From January 2010 to December 2012, 373 patients who underwent on-pump CABG were enrolled. Propensity analysis was performed to compare the postoperative outcomes of postoperative AKI, renal replacement therapy (RRT), intensive care unit (ICU) stay, mortality, and extubating time. In total, 98 patients received conventional on-pump surgery, 160 received OPBH surgery, and 115 received off-pump surgery. The Society of Thoracic Surgeons scores of these 3 groups were 6.1 ± 13.6, 7.4 ± 13.6, and 5.6 ± 10.9, respectively. Propensity analysis revealed lower AKI incidence in the off-pump group than in the on-pump surgery group. No substantial differences were observed in mortality, RRT, and the ICU stay between the off-pump and OPBH surgery groups. Among the 3 surgical methods, off-pump surgery results in lower AKI incidence. The short-term outcome, including kidney function, of OPBH surgery is similar to that of the off-pump group. Therefore, OPBH surgery is a considerable choice for patients with a high surgical risk.
1. Introduction
Acute kidney injury (AKI) affects 12% to 50% of patients undergoing coronary artery bypass grafting (CABG).[1–5] Moreover, 2% to 11.2% patients with an increased mortality rate require renal replacement therapy (RRT).[6,7] Despite advances in cardiac surgery management, postoperative AKI still results in high short-term mortality, a complicated hospital course, high medical expenditure, and long-term dialysis dependence.[8] Age, sex, diabetes mellitus, congestive heart failure, chronic kidney disease, peripheral atherosclerosis, and chronic obstructive pulmonary disease are the risk factors for post-CABG AKI.[1,9] Several clinical trials have compared the effect of off-pump CABG and on-pump CABG on renal dysfunction.[10–12] Off-pump method had less incidence of AKI compared with on-pump arrest method. A recent study established on-pump beating heart (OPBH) surgery by combining standard on-pump surgery and off-pump surgery; the highest benefits of OPBH surgery are hemodynamic stability and the absence of cardioplegic arrest guaranteed during extensive heart manipulation, particularly for unstable, high-risk patients.[13] However, no previous study has compared the renal outcomes of the 3 surgical types. This study compared the incidence rates of AKI, RRT, and mortality after cardiac surgery.
2. Methods
2.1. Study design and patient population
This post hoc analysis of a prospectively collected database was approved by the Institutional Review Board of Chang Gung Memorial Hospital. Patient records were anonomized and analyzed, and individual consents were waived. The aforementioned database comprised the medical records of 440 consecutive patients who received isolated CABG between January 2010 and December 2012 in a tertiary referral hospital. To clarify renal outcomes, patients with end-stage renal disease, confirmed AKI, and extracorporeal membrane oxygenation before surgery were excluded. Those who underwent dialysis before surgery and those with missing perioperative creatinine (Cr) data were also excluded. In total, 373 patients were enrolled into this study.
2.2. Data collection and definitions
The clinical characteristics, demographic data, and Society of Thoracic Surgeons (STS) score were extracted from the database. The baseline Cr level was defined as the preoperative value obtained on the date closest to the operation date. The primary outcome was postoperative AKI within 7 days. According to the definition provided in the Kidney Disease Improving Global Outcomes guidelines (KDIGO), AKI was diagnosed based on the following conditions: an increase in serum Cr of over 0.3 mg/dL within 48 hours or an increase in Cr exceeding the baseline by 1.5 times.[14] The outcomes of the incidence of AKI, RRT, mortality, duration of ventilator usage, and intensive care unit (ICU) stay were compared among the different surgical types. Urgent and emergent operation was defined according to EuroSCORE.[15] Shock was defined as hypotension with systolic arterial blood pressure of 90 mm Hg, despite adequate fluid resuscitation.
2.3. Surgical technique and postoperative care
All surgeons in our institution are familiar with all 3 techniques; the choice of off-pump, OPBH, or conventional cardioplegic arrest CABG depended on the preference of the individual surgeons. In both on-pump cohorts, cardiopulmonary bypass was established in a similar manner through the use of pulsatile flow. In the conventional CABG group, myocardial protection was obtained using 1 L of cold blood cardioplegia delivered antegradely or retrogradely; this process was repeated every 30 minutes, as necessary. In the OPBH group, commercially available stabilizers were used, and intracoronary artery shunts were used in all anastomosis connections. No conversion of OPBH to conventional CABG was performed during the study period.
2.4. Statistical analysis
Data are presented as mean ± standard deviation for continuous data and number (percentage) for categorical data. We compared the baseline characteristics and the surgical details of the study patients among the different surgical methods by using 1-way analysis of variance for continuous variables or the Fisher exact test for categorical variables. To control for confounding factors when comparing outcomes among the different surgical methods, we performed propensity score subclassification analyses.[16] We calculated the propensity score using the following covariates that are associated with AKI: age, sex, preoperative Cr level, cardiac ejection fraction, emergent/urgent operation, use of intra-aortic balloon pump (IABP), preoperative ventilator use, diabetes mellitus, recent myocardial infarction, shock, and chronic obstructive pulmonary disease. The propensity score was further equally divided into a quintile and was treated as a stratum variable in the logistic regression model performed for comparing the categorical outcomes (ie, in-hospital death or AKI) among the different surgical methods. For comparing the continuous outcomes (ie, extubation hours or ICU duration), the quintile of propensity score was treated as a clustered variable (the second level), and the averaged intercept of each quintile was allowed to vary (random effect) in the linear mixed-effect model. The data were analyzed using SPSS 22 (IBM SPSS, Armonk, New York, NY: IBM Corp).
3. Results
3.1. Characteristics of the study population
A total of 373 patients with a mean age of 64.1 ± 11.3 years and including 307 (82.6%) men were investigated. All baseline characteristics are listed in Table 1. No significant differences were observed in age, sex, and preoperative renal and liver functions among the different surgical groups. A preoperative heart condition, such as the functional class of heart function, ejection fraction, IABP, recent myocardial infarction, and shock, was similar among these groups. The prevalence of chronic obstructive pulmonary disease was higher in the OPBH group than in the other groups (P = .022). The STS scores of mortality risk and renal failure were 6.5 ± 12.8 and 7.8 ± 13.4, respectively. No substantial differences were observed in the STS scores of mortality (P = .462) and renal failure (P = .689) among the 3 groups.
Table 1.
Baseline characteristics of patients who underwent conventional arrest coronary artery bypass surgery by surgical method.

3.2. Surgical details
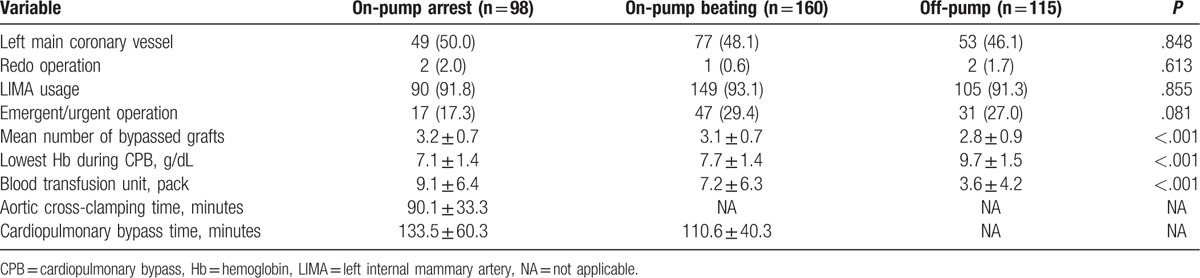
No significant differences were observed in left main coronary vessel disease, use of the left internal mammary artery (LIMA), and redo operation among all groups (Table 2). Patients in the on-pump arrest group were less likely to undergo emergent/urgent operations than patients in the OPBH and off-pump groups, although this trend was insignificant (17.3%, 29.4%, and 27%, respectively; P = .081). Compared with patients in the on-pump arrest or OPBH groups, patients in the off-pump group underwent bypass with fewer grafts (3.2 ± 0.7, 3.1 ± 0.7, and 2.8 ± 0.9, respectively; P < .001), had the highest levels of hemoglobin during cardiopulmonary bypass (7.1 ± 1.4, 7.7 ± 1.4, and 9.7 ± 1.5 g/dL, respectively; P < .001), and had a minimal volume of blood transfusion (9.1 ± 6.4, 7.2 ± 6.3, and 3.6 ± 4.2 units, respectively; P < .001). The time taken for cardiopulmonary bypass was 133.5 ± 60.3 and 110.6 ± 40.3 minutes in the on-pump arrest and OPBH groups, respectively.
Table 2.
Data for different surgical methods.
3.3. Postoperative complications and outcome
Table 3 shows the propensity score subclassification analysis of in-hospital death. The risk of in-hospital death was comparable among the 3 groups (the on-pump arrest group vs the OPBH group, P = .762; the on-pump arrest group vs the off-pump group, P = .946; the OPBH group vs the off-pump group, P = .759). In this study, AKI of any severity occurred in 98 patients (26.3%) within 7 days after surgery. As shown in Table 4, the incidence of AKI was higher in the on-pump arrest group than in the off-pump group (odds ratio [OR] 2.67, 95% confidence interval [CI] 1.35–5.26, P = .005). No significant difference was observed in AKI incidence between either the OPBH and off-pump groups (P = .066), or the on-pump arrest and OPBH groups (P = .162). However, as shown in Table 5, hemodialysis risk was comparable among these groups (the on-pump arrest group vs the OPBH group, P = .898; the on-pump arrest group vs the off-pump group, P = .811; the OPBH group vs the off-pump group, P = .547). The results are also shown in Fig. 1.
Table 3.
Comparison of incidence of in-hospital death among surgical methods using subclassification analysis of propensity score.

Table 4.
Comparison of incidence of acute kidney injury among surgical methods using subclassification analysis of propensity score.

Table 5.
Comparison of incidence of hemodialysis among surgical methods using subclassification analysis of propensity score.

Figure 1.

Comparison of incidence of categorical outcome among surgical methods. The combined odds ratio was estimated using the quintile of propensity score as a stratum variable in the logistic regression model.
Patients in the off-pump group received shorter extubation hours than those in the on-pump arrest group (23.0 ± 44.8 vs 41.6 ± 67.8 h; P = .017). However, no differences were observed between the on-pump arrest and OPBH groups, and between the OPBH and off-pump groups (P = .103 and P = .356, respectively, as presented in Supplement Table 1). No significant difference was observed in ICU stay among these groups (as illustrated in Supplement Table 2). The results are also illustrated in Fig. 2.
Figure 2.

Comparison of continuous outcome among surgical methods. The combined regression coefficient was estimated using the linear mixed-effect model using the quintile of propensity score as a clustered variable.
4. Discussion
Postcardiac surgery AKI is a part of cardiorenal syndrome and reflects the cumulative consequences of numerous perioperative factors that include ischemia–reperfusion, inflammatory cytokines, hemolysis, oxidase stress, and nephrotoxic agents, which result in tubular and vascular cell dysfunction, necrosis, apoptosis, and inflammation.[17,18] Even a minimal increase in serum Cr levels postoperatively is independently associated with long-term mortality and cardiovascular outcomes,[19] and might also contribute to chronic kidney dysfunction.[20] In 2012, the CORONARY trial that compared the 30-day outcome between on-pump surgery and off-pump surgery revealed an increased incidence of stage 1 and stage 2 AKI, but not stage 3 AKI and dialysis.[21] One-year follow-up analysis did not reveal substantial differences in loss of kidney function between the 2 groups.[22] Two explanations may be offered for this finding. First, the magnitude of AKI occurring after off-pump CABG might be related to prerenal azotemia without kidney structural damage. Second, revascularization might serve as a competing factor for the long-term renal outcome, whereas incomplete and suboptimal revascularization might be related to technical difficulties in long-term follow-up.[23] Reduction of cardiopulmonary bypass duration also attenuates pump-induced hemolysis, thereby releasing hemoglobin and free iron, and injuring the renal tubule.[24] Large-scale hemodilution and more blood transfusion during on-pump beating surgery might reduce oxygen delivery and induce inflammation through blood transfusion.[25,26] Although off-pump CABG might reduce the physiologic derangement caused by the systemic inflammatory response and attenuate the myocardial injury caused by ischemia–reperfusion, the on-pump method provides improved long-term survival, because of the patency of the anastomosis of blood vessels.[27]
In the past decade, a hybrid method (ie, OPBH surgery) combining standard on-pump surgery and the off-pump CABG technique has been used to avoid cardioplegic arrest and its nonphysiological nature, which may lead to mortality and morbidity in patients with poor cardiac function. The absence of cardioplegic arrest and hemodynamic stability are the highest benefits of this technique, particularly for patients with left ventricular dysfunction.[13,28,29] We hypothesized that OPBH surgery would provide improved systemic circulation and influence the renal outcome.[30] Chaudhry et al and Ueki et al, respectively, performed a good meta-analysis to compare the results between OPBH and conventional arrest CABG, both of them concluded that dialysis-requiring renal failure was less in OPBH-CABG. [31–33] There are no data regarding AKI by KDIGO definition in meta-analysis. In our result, dialysis seems to be less in OPBH, tough it did not reach statistical significance using propensity score analysis. In this study, we directly compared the short-term survival and renal outcomes among the OPBH, no-pump arrest, and off-pump CABG groups through propensity analysis. Regarding AKI incidence, off-pump surgery is superior to on-pump arrest, but not dialysis; this result is similar to that of a meta-analysis.[34] No substantial difference was observed in mortality, AKI, and RRT between the OPBH and off-pump groups. The avoidance of systemic hypothermia, cardiac arrest, rewarming, and recovery from myocardial stunning theoretically maintained the stability of systemic circulation and might facilitate the reduction of renal ischemia. This study provides evidence that in patients with a high surgical risk, the short-term outcomes, including mortality and renal dysfunction, of the OPBH method, are not inferior to those of off-pump surgery. Further comparisons of long-term outcomes would be valuable.
4.1. Study limitations
Despite the favorable results, several limitations should be noted. First, compared with other large-scale trials, our investigation was based on a small number of risky patients and was conducted at a single tertiary care medical center in Asia; therefore, regional and ethnic differences should be considered. Second, because postoperative care, postoperative bleeding, and infection contribute to AKI, researchers who aspire to expand the application to AKI occurring after postoperative day 7 should exercise caution. Finally, though all surgeons in this study were familiar with these surgical techniques, a selection bias that is caused by surgeon preference still might exist. Additional randomized trials are warranted to eliminate this limitation.
5. Conclusions
This study is the first to directly compare the incidence of AKI among the 3 surgical types. The on-pump arrest CABG method results in a higher incidence of AKI, which contributes to a lower incidence of mild and moderate AKI when compared with conventional CABG. In patients with a high surgical risk, the OPBH method is a reasonable choice.
Acknowledgments
The authors thank Alfred Hsing-Fen Lin and all the participating patients of the Kidney Research Center of Chang Gung Memorial Hospital, Linkou, Taiwan.
Supplementary Material
Footnotes
Abbreviations: AKI = acute kidney injury, CABG = coronary artery bypass grafting, CI = confidence interval, Cr = creatinine, IABP = intra-aortic balloon pump, ICU = intensive care unit, KDIGO = Kidney Disease Improving Global Outcomes, LIMA = left internal mammary artery, OPBH = on-pump beating heart, OR = odds ratio, RRT = renal replacement therapy, STS score = Society of Thoracic Surgeons score.
M-JC and C-CL contributed equally to this work.
Funding: This research was supported by a research grant from Chang Gung Medical Foundation (CORPG3F0211).
Conflicts of interest: Dr C-H Chang was supported by the Ministry of Science and Technology (MOST 103–2314-B-182A-018-MY3).
Supplemental Digital Content is available for this article.
References
- [1].Rosner MH, Okusa MD. Acute kidney injury associated with cardiac surgery. Clin J Am Soc Nephrol 2006;1:19–32. [DOI] [PubMed] [Google Scholar]
- [2].Gallagher S, Jones DA, Lovell MJ, et al. The impact of acute kidney injury on midterm outcomes after coronary artery bypass graft surgery: a matched propensity score analysis. J Thorac Cardiovasc Surg 2014;147:989–95. [DOI] [PubMed] [Google Scholar]
- [3].Ryden L, Ahnve S, Bell M, et al. Acute kidney injury after coronary artery bypass grafting and long-term risk of myocardial infarction and death. Int J Cardiol 2014;172:190–5. [DOI] [PubMed] [Google Scholar]
- [4].Reents W, Hilker M, Borgermann J, et al. Acute kidney injury after on-pump or off-pump coronary artery bypass grafting in elderly patients. Ann Thorac Surg 2014;98:9–14. [discussion 14-15]. [DOI] [PubMed] [Google Scholar]
- [5].Chen SW, Chang CH, Fan PC, et al. Comparison of contemporary preoperative risk models at predicting acute kidney injury after isolated coronary artery bypass grafting: a retrospective cohort study. BMJ Open 2016;6:e010176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Thakar CV, Worley S, Arrigain S, et al. Improved survival in acute kidney injury after cardiac surgery. Am J Kidney Dis 2007;50:703–11. [DOI] [PubMed] [Google Scholar]
- [7].Tsai HS, Tsai FC, Chen YC, et al. Impact of acute kidney injury on one-year survival after surgery for aortic dissection. Ann Thorac Surg 2012;94:1407–12. [DOI] [PubMed] [Google Scholar]
- [8].Chen TH, Chang CH, Lin CY, et al. Acute kidney injury biomarkers for patients in a coronary care unit: a prospective cohort study. PloS One 2012;7:e32328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Haase M, Haase-Fielitz A, Bellomo R. Cardiopulmonary bypass, hemolysis, free iron, acute kidney injury and the impact of bicarbonate. Contrib Nephrol 2010;165:28–32. [DOI] [PubMed] [Google Scholar]
- [10].Nathoe HM, van Dijk D, Jansen EW, et al. A comparison of on-pump and off-pump coronary bypass surgery in low-risk patients. N Engl J Med 2003;348:394–402. [DOI] [PubMed] [Google Scholar]
- [11].Straka Z, Widimsky P, Jirasek K, et al. Off-pump versus on-pump coronary surgery: final results from a prospective randomized study PRAGUE-4. Ann Thorac Surg 2004;77:789–93. [DOI] [PubMed] [Google Scholar]
- [12].Puskas JD, Williams WH, Mahoney EM, et al. Off-pump vs conventional coronary artery bypass grafting: early and 1-year graft patency, cost, and quality-of-life outcomes: a randomized trial. JAMA 2004;291:1841–9. [DOI] [PubMed] [Google Scholar]
- [13].Ferrari E, Stalder N, von Segesser LK. On-pump beating heart coronary surgery for high risk patients requiring emergency multiple coronary artery bypass grafting. J Cardiothorac Surg 2008;3:38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Palevsky PM, Liu KD, Brophy PD, et al. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for acute kidney injury. Am J Kidney Dis 2013;61:649–72. [DOI] [PubMed] [Google Scholar]
- [15].Roques F, Michel P, Goldstone AR, et al. The logistic EuroSCORE. Eur Heart J 2003;24:881–2. [DOI] [PubMed] [Google Scholar]
- [16].Sjolander A. Propensity scores and M-structures. Stat Med 2009;28:1416–20. [author reply 1420-1413]. [DOI] [PubMed] [Google Scholar]
- [17].Chang CH, Yang CH, Yang HY, et al. Urinary biomarkers improve the diagnosis of intrinsic acute kidney injury in coronary care units. Medicine 2015;94:e1703. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Yang CH, Chang CH, Chen TH, et al. Combination of urinary biomarkers improves early detection of acute kidney injury in patients with heart failure. Circ J 2016;80:1017–23. [DOI] [PubMed] [Google Scholar]
- [19].Liotta M, Olsson D, Sartipy U, et al. Minimal changes in postoperative creatinine values and early and late mortality and cardiovascular events after coronary artery bypass grafting. Am J Cardiol 2014;113:70–5. [DOI] [PubMed] [Google Scholar]
- [20].Coca SG, Singanamala S, Parikh CR. Chronic kidney disease after acute kidney injury: a systematic review and meta-analysis. Kidney Int 2012;81:442–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Lamy A, Devereaux PJ, Prabhakaran D, et al. Off-pump or on-pump coronary-artery bypass grafting at 30 days. N Engl J Med 2012;366:1489–97. [DOI] [PubMed] [Google Scholar]
- [22].Garg AX, Devereaux PJ, Yusuf S, et al. Kidney function after off-pump or on-pump coronary artery bypass graft surgery: a randomized clinical trial. JAMA 2014;311:2191–8. [DOI] [PubMed] [Google Scholar]
- [23].Schwann NM, Horrow JC, Strong MD, 3rd, et al. Does off-pump coronary artery bypass reduce the incidence of clinically evident renal dysfunction after multivessel myocardial revascularization? Anesth Analg 2004;99:959–64. [table of contents]. [DOI] [PubMed] [Google Scholar]
- [24].Vermeulen Windsant IC, Snoeijs MG, Hanssen SJ, et al. Hemolysis is associated with acute kidney injury during major aortic surgery. Kidney Int 2010;77:913–20. [DOI] [PubMed] [Google Scholar]
- [25].Karkouti K, Beattie WS, Wijeysundera DN, et al. Hemodilution during cardiopulmonary bypass is an independent risk factor for acute renal failure in adult cardiac surgery. J Thorac Cardiovasc Surg 2005;129:391–400. [DOI] [PubMed] [Google Scholar]
- [26].Habib RH, Zacharias A, Schwann TA, et al. Role of hemodilutional anemia and transfusion during cardiopulmonary bypass in renal injury after coronary revascularization: implications on operative outcome. Crit Care Med 2005;33:1749–56. [DOI] [PubMed] [Google Scholar]
- [27].Kim JB, Yun SC, Lim JW, et al. Long-term survival following coronary artery bypass grafting: off-pump versus on-pump strategies. J Am Coll Cardiol 2014;63:2280–8. [DOI] [PubMed] [Google Scholar]
- [28].Rastan AJ, Bittner HB, Gummert JF, et al. On-pump beating heart versus off-pump coronary artery bypass surgery-evidence of pump-induced myocardial injury. Eur J Cardiothorac Surg 2005;27:1057–64. [DOI] [PubMed] [Google Scholar]
- [29].Erkut B, Dag O, Kaygin MA, et al. On-pump beating-heart versus conventional coronary artery bypass grafting for revascularization in patients with severe left ventricular dysfunction: early outcomes. Can J Surg 2013;56:398–404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].Tsai YT, Lin FY, Lai CH, et al. On-pump beating-heart coronary artery bypass provides efficacious short- and long-term outcomes in hemodialysis patients. Nephrol Dial Transplant 2012;27:2059–65. [DOI] [PubMed] [Google Scholar]
- [31].Chaudhry UA, Harling L, Sepehripour AH, et al. Beating-heart versus conventional on-pump coronary artery bypass grafting: a meta-analysis of clinical outcomes. Ann Thorac Surg 2015;100:2251–60. [DOI] [PubMed] [Google Scholar]
- [32].Ueki C, Sakaguchi G, Akimoto T, et al. On-pump beating-heart technique is associated with lower morbidity and mortality following coronary artery bypass grafting: a meta-analysis. Eur J Cardiothorac Surg 2016;50:813–21. [DOI] [PubMed] [Google Scholar]
- [33].Yanagawa B, Puskas JD. Invited commentary. Ann Thorac Surg 2015;100:2261. [DOI] [PubMed] [Google Scholar]
- [34].Seabra VF, Alobaidi S, Balk EM, et al. Off-pump coronary artery bypass surgery and acute kidney injury: a meta-analysis of randomized controlled trials. Clin J Am Soc Nephrol 2010;5:1734–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.