

Abstract
Periodontitis is one of the most prevalent oral diseases. In this study, we probed the nationwide registered database to assess the time trends of prevalence of periodontitis in Taiwan.
A retrospective study was conducted to analyze the registered database compiled by the National Health Insurance provided by the Department of Health, Taiwan, from 1997 to December 2013.
We found that the prevalence of periodontitis significantly increased from 11.5% in 1997 to 19.59% in 2013 (P for trend < .0001). The mean age ± standard deviation with periodontitis from 1997 to 2013 was 54.46 ± 14.47 and 45.51 ± 16.58 years old, respectively. The proportion of individuals with periodontitis in age group >65 years old decreased markedly. The proportion of individuals with periodontitis in age groups <25 and 26 to 35 years old demonstrated an increased pattern. Compared to the reference cohort of 1953 to 1957, the recent birth cohort of 1993 to 1997 revealed the highest relative risk (RR) of periodontitis (male: RR, 67.42, 95% confidence interval [CI], 17.04–266.76; female: RR, 65.85, 95% CI, 16.70–259.70). Both male and female groups showed the similar age-effect pattern in the cross-sectional age curve from age–period–cohort model. There was an upturn with advancing age up to 40 to 50 years old and then a downward trend in both genders. Population dwelling in suburban area (RR, 0.95; 95% CI, 0.94–0.97) and rural area (RR, 0.97; 95% CI, 0.95–0.99) had the lower risk of periodontitis than those who lived in urban area. The higher income group revealed the higher risk of periodontitis compared with lower income group (RR, 1.20; 95% CI, 1.18–1.23).
The prevalence of periodontitis significantly increased in Taiwan over past 17 years. The mean age with periodontitis was shown in a decreased pattern. The use of a nationwide population-based database could provide sufficient sample size, generalizability, and statistical power to assess the periodontal status in Taiwan.
Keywords: nationwide population-based study, periodontitis, prevalence, Taiwan
1. Introduction
In addition to caries, periodontal disease is the most prevalent oral diseases among adults worldwide that average 11.2% of the populations suffer from severe chronic periodontitis worldwide.[1] In general, periodontitis accounts for most cases of tooth loss, and their impact increases with age. The prevalence of periodontally healthy individuals is increasing and severe periodontitis is more common in older age groups.[2–6] Smoking, inadequate oral hygiene, stress, and lifestyle-related comorbidities are well-known risk factors for periodontitis.[7] Studies have also shown that irregular or no use of dental health services and low education level are important factors associated with periodontitis.[8–10]
Currently, in Taiwan, periodontitis is reported to have affected more than half of the adult population with the definition of community periodontal index ≥3.[11] However, up to now, a retrospective large national cohort study involving patient samples stratified on the basis of demographic information has not been conducted. Taiwan's National Health Insurance (NHI) began in March 1, 1995 and covered 99.9% of Taiwan's residents by 2014.[12] Such a high coverage rate made the NHI database the best national indicator of health issues and easier to update annually de-identified by scrambling the identification codes of both patients and medical facilities formatted as a National Health Insurance Research Database (NHIRD).
The aim of this study was then to investigate the prevalence of periodontitis in Taiwan from NHIRD. In addition, the age, sex, income, geographical region, and urbanization factors using the same methodology to investigate the prevalence of periodontitis in data available from cross-sectional analysis conducted from 1997 to 2013. In addition, age–period–cohort (APC) analysis was performed to investigate the effects of age, diagnosis period, and birth cohort with periodontitis from 1999 to 2013.
2. Materials and methods
2.1. Data source and ethical consideration
This study was approved by the Ethics Review Board at the Chung Shan Medical University Hospital. With strict confidentiality guidelines being closely followed in accordance with personal electronic data protection regulations; the National Health Research Institutes anonymized and maintained the NHI reimbursement data as files suitable for researches. No written informed consent was obtained from the participants, because the identification numbers used in the NHIRD assure patient anonymity. The data subset systematic sampling of the ambulatory care expenditures by visit together with the related records in details of ambulatory care orders was used for this study from 1997 to 2013. This report complies with Strengthening the Reporting of Observational Studies in Epidemiology guidelines for the observational studies.
2.2. Patient identification and measurements
The diagnostic coding of NHI in Taiwan is according to the International Classification of Diseases, Ninth Clinical Modification (ICD-9-CM). The cases of periodontitis were identified with ICD-9 codes of 523.3, 523.4, and 523.5. To ensure the criteria of indication and the accuracy of diagnosis for periodontitis, ICD-9 procedure code 9654, 2431, and 2439 were also defined. The codes 9654, 2431, and 2439 corresponding to Taiwan NHI's Fee Schedule for Medical Services claim codes from 91004 to 91010 were included. Information about the collection of pocket depth data in the patient's record has been described for each periodontal treatment. The estimated annual prevalence rate of periodontitis from 1997 to 2013 was extracted from population of systematic sampling of the ambulatory care expenditures by visit together with the related records in details of ambulatory care orders. The population aged equal to or under 12-year, older than 90-year and with missing data were excluded. Monthly income was categorized as follows: <New Taiwan Dollar (NTD) $20,000, NTD $20,000 to 40,000, and >NTD$40,000. The urbanization of the locations of NHI registration was used as a proxy parameter for socioeconomic status. Urbanization was categorized 3 levels: urban, suburban, and rural areas based on the classification scheme proposed by Liu et al.[13]
2.3. Statistical analysis
Annual prevalence rate of periodontitis was examined by Cochran–Armitage trend test for probing the trend from 1997 to 2013. A P value for trend <.05 was set to declare statistical significance. Mean age with standard deviation (SD) of population of periodontitis was presented annually. The age-specific estimates and prevalence rates by age distribution which divided into 6 subgroups (≤25, 26–35, 36–45, 46–55, 56–65, and ≥65) were calculated. We conducted Student t test to investigate the differences within continuous variables and one sample chi-squared test within categorical variables.
APC analysis was performed to investigate the effects of age, diagnosis period, and birth cohort with periodontitis. Cases of periodontitis were categorized into 15 age groups (16–20 to 86–90), 3 period groups (1999–2003, 2004–2008, and 2009–2013), and 17 birth cohort groups (1913–1917 to 1993–1997) with a corresponding 5-year interval. Several models such as age alone, period alone, cohort alone, and APC were generated. The goodness of fit for the specified model was evaluated by the deviance/degree of freedom. Relative risk (RR), percent per year (PPY), and 95% confidence interval (CI) of periodontitis for males and females by APC analysis were calculated. The socioeconomic-specific estimates and prevalence rates by subgroups including distribution of urbanization and payroll bracket (monthly income) were calculated separately. The RR and 95% CI of periodontitis for urbanization and payroll bracket from 1997 to 2013 after adjusting for year, gender, and age groups were evaluated by multivariate Poisson regression. The results were considered significant with a 2-tailed P < .05. All statistical analyses were performed with the SPSS version 22 (SPSS, Chicago, IL). For APC analysis, we performed with a web tool (Division of Cancer Epidemiology and Genetics, National Cancer Institute, National Institutes of Health, Maryland).[14]
3. Results
A total of 904,380 subjects were enrolled into this study. Of these, 144,473 subjects (66,585 males and 77,708 females, respectively) were diagnosed as periodontitis according to the ICD-9-CM criteria in this study. As shown in Fig. 1, the annual prevalence steadily increased for overall and both gender during the study period. The annual prevalence rates of periodontitis examined by Cochran–Armitage trend test indicated significant increasing trends for prevalence of periodontitis (P for trend <.0001). The prevalence of periodontitis by year gradually increased from 11.5% in 1997 to 19.59% in 2013 over the 17-year study period. The prevalence of periodontitis was also increased significantly in both genders (male: P for trend <.0001; female: P for trend <.0001).
Figure 1.
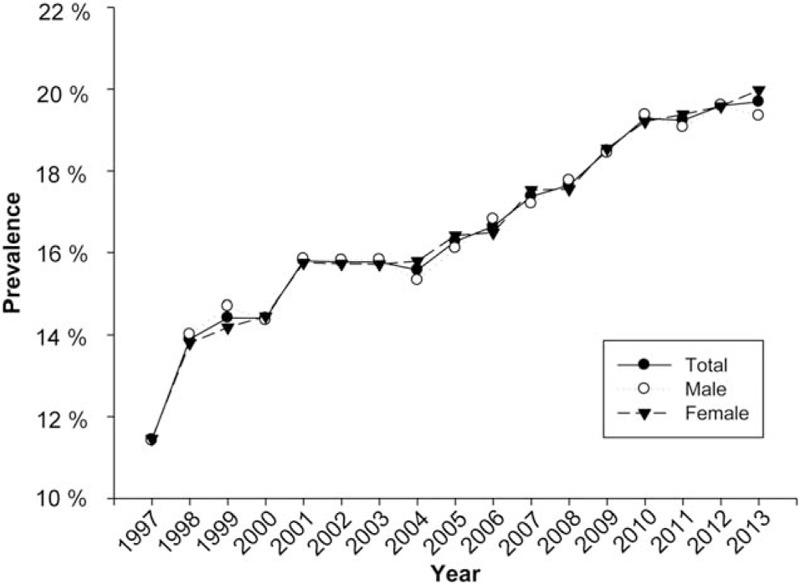
Time trends for the prevalence of periodontitis in Taiwan. The prevalence of periodontitis increased significantly from 11.5% in 1997 to 19.59% in 2013.
As shown in Fig. 2, the mean age for periodontitis was shown a decreased pattern from 1997 to 2013. The mean age ± SD of patients with periodontitis in Taiwan from 1997 to 2013 was demonstrated in Table 1. The mean age ± SD with periodontitis from 1997 to 2013 was 54.46 ± 14.47 and 45.51 ± 16.58 years old, respectively. In addition, the mean age ± SD in male group from 1997 to 2013 was 55.87 ± 14.58 and 45.83 ± 16.72 years old, respectively. The mean age ± SD in female group from 1997 to 2013 was 53.27 ± 14.27 and 45.35 ± 16.41 years old, respectively.
Figure 2.
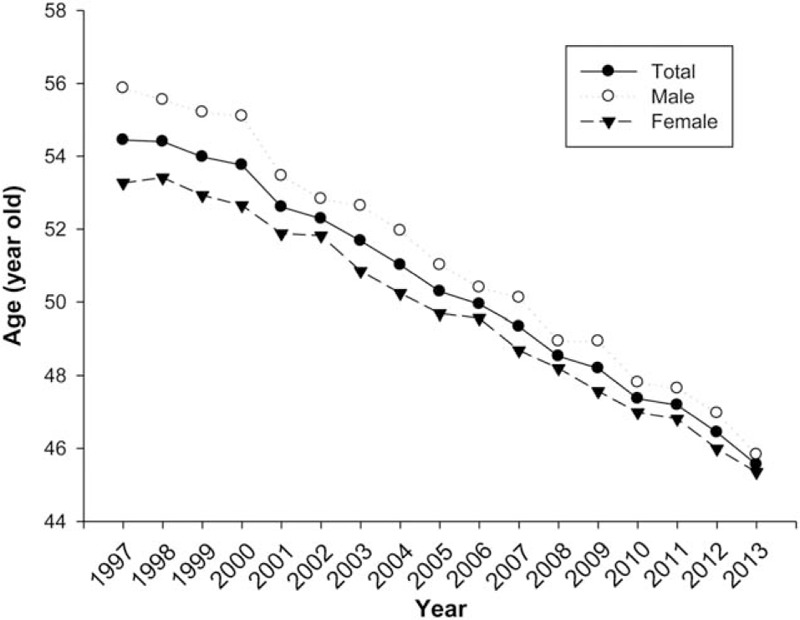
Mean age of patients with periodontitis in Taiwan. The mean age for periodontitis was shown a decrease pattern from 1997 to 2013.
Table 1.
Mean age of patients with periodontitis in Taiwan from 1997 to 2013.

Prevalence categorized by age group and gender is shown in Table 2. The prevalence of periodontitis at age group ≤25, 26–35, 36–45, 46–55, 56–65, and >65 years old was 4.66%, 15.51%, 19.85%, 21.22%, 20.83%, and 16.04%, respectively. It was also noted that male with significantly higher prevalence rates than female in age group of 46 to 55 and 56 to 65 years old (P < .0001), while female who aged <25 years old had a significantly higher prevalence rate than male (P < .0001).
Table 2.
Population and prevalence of periodontitis by age distribution in Taiwan from 1997 to 2013.

Frequency distribution (%) of patients with periodontitis in various age groups in Taiwan from 1997 to 2013 is shown in Fig. 3. The proportion of age group >65 years old with periodontitis individuals decreased markedly. Interestingly, the proportion of age groups <25 and 26 to 35 years old with periodontitis individuals significantly increased.
Figure 3.
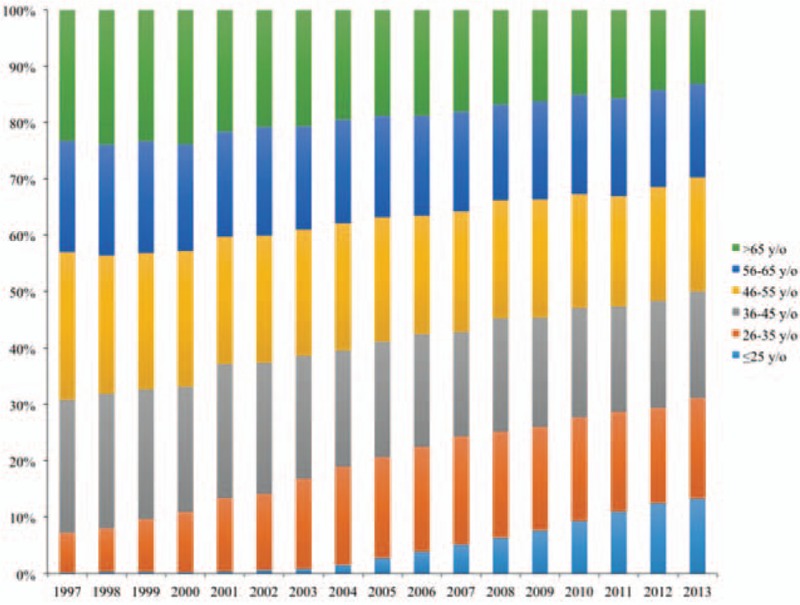
Frequency distribution of age-specific group in the prevalence of periodontitis in Taiwan from 1997 to 2013.
Table 3 showed the results of APC model for male and female groups. The effects of age, diagnosis period, and birth cohort of periodontitis by gender were revealed in Table 4. The full APC model provided a significantly better fit to the data in male (P = .12) than that in female (P = .03). The age effect showed significant differences in both gender, indicating the age groups 16 to 20 years old had highest PPY than any other age groups. Compared to the reference cohort of 1953 to 1957, the recent birth cohort of 1993 to 1997 had highest RR of periodontitis (male: RR, 67.42; 95% CI, 17.04–266.76; female: RR, 65.85; 95% CI, 16.70–259.70). No obvious period effect of periodontitis was observed in both genders. As shown in Fig. 4, it was evident that both male and female demonstrated the similar age-effect pattern in the cross-sectional age curve from APC model. There was an upturn with advancing age up to 40 to 50 years old and then a downward trend in both genders.
Table 3.
Results of age–period–cohort model for periodontitis in Taiwan from 1999 to 2013.

Table 4.
Percent per year (PPY), relative risk (RR), and 95% confidence interval (CI) of periodontitis for males and females by age–period–cohort analysis in Taiwan from 1999 to 2013.

Figure 4.
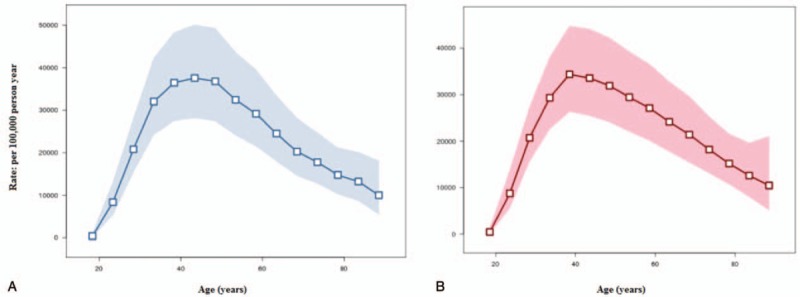
Cross-sectional age curve from age–period–cohort model in the rate of periodontitis in Taiwan from 1999 to 2013. (A) Male group, (B) Female group.
The results of multivariate Poisson regression on the risk of periodontitis for urbanization and payroll bracket (monthly income) in Taiwan from 1997 to 2013 were shown in Table 5. Population dwelling in suburban area (RR, 0.95; 95% CI, 0.94–0.97) and rural area (RR, 0.97; 95% CI, 0.95–0.99) had the lower risk of periodontitis than those who lived in urban area. In addition, the higher income group revealed the higher risk of periodontitis compared with lower income group (RR, 1.20; 95% CI, 1.18–1.23).
Table 5.
Multivariate Poisson regression of urbanization and payroll bracket for periodontitis in Taiwan from 1997 to 2013.

4. Discussion
The nationwide survey of the prevalence of periodontitis had been reported in France,[2] German,[3] China,[15] the United States,[10] and Taiwan.[11] Several studies of the trends in periodontal conditions had been reported in the cities of Europe.[4–6,16–19] These surveys were mostly based on the cross-section design, noninstitutionalized population data according to the level of clinical attachment loss and the depth of probing pocket depth. In the present study, to the best of our knowledge, this is the first large-scale, retrospective, and longitudinal population-based study to investigate the prevalence of in Taiwan from NHIRD. In this study, the prevalence of periodontitis in Taiwan significantly increased from 1997 to 2013. In 2013, the prevalence of periodontitis in Taiwan is approximately up to 20%. However, the ratio is significantly lower than previous nationwide periodontitis survey reports.[2,3,10,11,15] The reasons may be explained as following. In this study, the collected data regarding the diagnoses of periodontitis based on the ICD-9 codes recorded in the NHIRD may not truly indicate the severity of periodontitis. In addition, the use of dental care was estimated up to 45% of Taiwan's population in 2013.[12] Therefore, prevalence and severity of disease might be underestimated by using nationwide registration system in Taiwan. However, our results discover the important findings that the prevalence of periodontitis increased gradually by year from 1997 to 2013.
To the best of our knowledge, we first found that the mean age of patients suffered from periodontitis was significantly decreased, especially, the proportion of age groups <25 and 26 to 35 years old. Consequently, the proportion of individuals in age group >65 years old with periodontitis was decreased markedly. The reason for this age decreasing trend is not quite clear. It may be due to the data bank used from NHIRD is based on the dental treatment records. A government-run insurer with a single-payer insurance system was established by the Taiwanese Government in 1995 with the goal of ensuring health coverage for the entire population. Moreover, the awareness of periodontitis in Taiwan Government, NHI offers dental prophylaxis twice a year to the public above 12 years old. The youngest cohort aged 16 to 20 years old in 2013 was fully covered by NHI after birth. Therefore, this efficient strategy has successfully increased the rates of early diagnosis and the treatment need for periodontitis.
Socioeconomic statuses such as lower income peoples have been shown to be associated with periodontitis.[15,20,21] By contrast, our results found higher income and the level of urbanization with RR of the periodontitis. It might be due to the convenient of dental service. In addition, patients’ attitudes toward dental treatment could also influence people's utilization of NHI in Taiwan. However, in a systematic review, socioeconomic variables were less important when smoking was included in the analysis.[22] Similar results have been shown in other studies of socioeconomic status and periodontal disease.[20,23] It is well known that smoking is an important risk factor for periodontitis. The information retrieved from this database did not contain health-related behaviors or status such as smoking. Thus, the effects of smoking or the relation of this behavior and the severity of disease could not be demonstrated in this study.
In Taiwan, the Bureau of NHI routinely samples patient charts randomly to cross-check the quality of claims from all medical institutions, and bias from miscoding or misclassification could be minimized. The use of a nationwide population-based database can provide sufficient sample size, generalizability, and statistical power to assess the periodontal status in Taiwan. It may be beneficial to provide additional data analysis and assist in planning treatment strategies in this national medical care system in periodontal treatment.
Footnotes
Abbreviations: APC = age–period–cohort analysis, CI = confidence interval, ICD-9-CM = International Classification of Diseases Ninth Clinical Modification, NHI = National Health Insurance, NHIRD = National Health Insurance Research Database, NTD = New Taiwan Dollar, PPY = percent per year, RR = relative risk, SD = standard deviation.
This study is based in part on data from the NHIRD provided by the Bureau of National Health Insurance, Department of Health and managed by National Health Research Institutes. The interpretation and conclusions contained herein do not represent those of National Health Insurance Administration, Department of Health or National Health Research Institutes.
The authors have no funding and conflicts of interest to disclose.
References
- [1].Kassebaum NJ, Bernabe E, Dahiya M, et al. Global burden of severe periodontitis in 1990–2010: a systematic review and meta regression. J Dent Res 2014;93:1045–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Bourgeois D, Bouchard P, Mattout C. Epidemiology of periodontal status in dentate adults in France, 2002–2003. J Periodontal Res 2007;42:219–27. [DOI] [PubMed] [Google Scholar]
- [3].Holtfreter B, Kocher T, Hoffmann T, et al. Prevalence of periodontal disease and treatment demands based on a German dental survey (DMS IV). J Clin Periodontol 2010;37:211–9. [DOI] [PubMed] [Google Scholar]
- [4].Skudutyte-Rysstad R, Eriksen HM, Hansen BF. Trends in periodontal health among 35-year-olds in Oslo, 1973–2003. J Clin Periodontol 2007;34:867–72. [DOI] [PubMed] [Google Scholar]
- [5].Hugoson A, Sjodin B, Norderyd O. Trends over 30 years, 1973–2003, in the prevalence and severity of periodontal disease. J Clin Periodontol 2008;35:405–14. [DOI] [PubMed] [Google Scholar]
- [6].Edman K, Öhrn K, Nordström B, et al. Trends over 30 years in the prevalence and severity of alveolar bone loss and the influence of smoking and socio-economic factors-based on epidemiological surveys in Sweden 1983–2013. Int J Dent Hygiene 2015;13:283–91. [DOI] [PubMed] [Google Scholar]
- [7].Jiang Y, Okoro CA, Oh J, et al. Sociodemographic and health-related risk factors associated with tooth loss among adults in Rhode Island. Prev Chronic Dis 2013;10:E45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Oliveira Costa F, Miranda Cota LO, Pereira Lages EJ, et al. Progression of periodontitis in a sample of regular and irregular compliers under maintenance therapy: a 3-year follow-up study. J Periodontol 2011;82:1279–87. [DOI] [PubMed] [Google Scholar]
- [9].Paulander J, Axelsson P, Lindhe J. Association between level of education and oral health status in 35-, 50-, 65- and 75-year-olds. J Clin Periodontol 2003;30:697–704. [DOI] [PubMed] [Google Scholar]
- [10].Eke PI, Dye BA, Wei L, et al. Update on prevalence of periodontitis in adults in the United States: NHANES 2009 to 2012. J Periodontol 2015;86:611–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Lai H, Su CW, Yen AM, et al. A prediction model for periodontal disease: modelling and validation from a National Survey of 4061 Taiwanese adults. J Clin Periodontol 2015;42:413–21. [DOI] [PubMed] [Google Scholar]
- [12].National Health Insurance Administration, Ministry of Health and Welfare, Taiwan, ROC. National Health Insurance Annual Report 2014; 2014–2015. [Google Scholar]
- [13].Liu CY, Hung YT, Chuang YL, et al. Incorporating development stratification of Taiwan townships into sampling design of large scale health interview survey. J Health Manag 2006;4:1–22. [Google Scholar]
- [14].Rosenberg PS, Check DP, Anderson WF. A web tool for age-period-cohort analysis of cancer incidence and mortality rates. Cancer Epidemiol Biomarkers Prev 2014;23:2296–302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Zhang Q, Li Z, Wang C, et al. Prevalence and predictors for periodontitis among adults in China, 2010. Global Health Action 2014;7:24503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Ankkuriniemi O, Ainamo J. Dental health and dental treatment needs among recruits of the Finnish defence forces, 1919–91. Acta Odontol Scand 1997;55:192–7. [DOI] [PubMed] [Google Scholar]
- [17].Hugoson A, Norderyd O, Slotte C, et al. Distribution of periodontal disease in a Swedish adult population 1973, 1983 and 1993. J Clin Periodontol 1998;25:542–8. [DOI] [PubMed] [Google Scholar]
- [18].Kalsbeek H, Truin GJ, Poorterman JH, et al. Trends in periodontal status and oral hygiene habits in Dutch adults between 1983 and 1995. Commun Dent Oral Epidemiol 2000;28:112–8. [DOI] [PubMed] [Google Scholar]
- [19].Hugoson A, Koch G, Göthberg C, et al. Oral health of individuals aged 3–80 years in Jonkoping, Sweden during 30 years (1973–2003). II. Review of clinical and radiographic findings. Swed Dent J 2005;29:139–55. [PubMed] [Google Scholar]
- [20].Albandar JM. Global risk factors and risk indicators for periodontal diseases. Periodontol 2000 2002;29:177–206. [DOI] [PubMed] [Google Scholar]
- [21].Croucher R, Marcenes WS, Torres MC, et al. The relationship between life-events and periodontitis. A case-control study. J Clin Periodontol 1997;24:39–43. [DOI] [PubMed] [Google Scholar]
- [22].Klinge B, Norlund A. A socio-economic perspective on periodontal diseases: a systematic review. J Clin Periodontol 2005;32:314–25. [DOI] [PubMed] [Google Scholar]
- [23].Norderyd O, Hugoson A. Risk of severe periodontal disease in a Swedish adult population. A cross-sectional study. J Clin Periodontol 1998;25:1022–8. [DOI] [PubMed] [Google Scholar]