

Abstract
Objectives:
To delineate the clinical features and outcomes of dengue infection and to guide clinician of early diagnosis and identification of risks factors for dengue hemorrhagic fever.
Methods:
This study is a retrospective cross-sectional. Clinical records of 567 patients with a confirmed diagnosis of dengue infection, admitted to a single hospital in Jeddah, Saudi Arabia, between January 2010 and June 2014 were reviewed.
Results:
Dengue infection was most common in adult males. Sixty-eight percent of infections were in Saudi nationals. In addition to the diagnostic clinical features, leucopenia and thrombocytopenia were typical of dengue infection. Approximately 4.1% of adult patients and 7.1% of pediatric patients developed dengue hemorrhagic fever (DHF). Abdominal pain and vomiting were more common in patients developing DHF. Mean platelet count was lower in adult, but not pediatric patients developing DHF. Peak alanine aminotransferase (ALT) was higher in adult and pediatric patients developing DHF. Three patients died, 2 of them developed DHF. Ninety-eight percent of adult patients and 92% of pediatric patients made a full recovery.
Conclusions:
Dengue infection is common in Jeddah. Abdominal pain and vomiting, thrombocytopenia, and elevated ALT are typical of severe infection, which is more likely to be associated with significant morbidity and mortality.
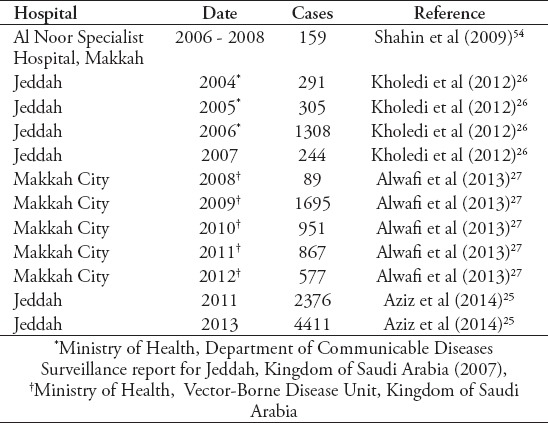
Dengue is a systemic viral infection that has emerged as a significant health threat primarily in tropical and subtropical countries with an estimated 390 million dengue infections per annum, 96 million of which manifest clinically1 with 3.9 billion people at risk worldwide.2 Dengue has been suggested to be the most important arthropod-borne viral infection of humans.3,4 Since 1970, more than 10 fold increase in the number of countries in which the World Health Organization (WHO) considers dengue to be endemic.1 The first patient to be confirmed to have dengue infection by virological analysis in Saudi Arabia, was admitted to Dr. Soliman Fakeeh Hospital in Jeddah in October 1993.3 Two further cases diagnosed in February 19943 heralded the first epidemic of dengue infection in Saudi Arabia with 289 cases.5 A number of additional studies document the increase in dengue cases in Jeddah and Makkah between 2004 and 2013 (Table 1), although these studies did not document clinical features. In 2009, the Saudi Ministry of Health reported 3350 cases across Saudi Arabia with a fatality rate of 4.6/1000.6 These studies demonstrate a clear increase in dengue incidence in Saudi Arabia since 1993. It has been suggested that pilgrims visiting Makkah for the Hajj may be a significant source of dengue infection.5,7 However, detailed phylogenetic analysis of virus strains circulating in Jeddah has suggested dengue to now be endemic in Saudi Arabia8 and the presence of dengue in western coastal areas of Saudi Arabia and throughout the region of Makkah is clearly documented1 (Table 1).
Table 1.
Studies documenting numbers of confirmed cases of dengue infection in Jeddah and Makkah City 2004-2013.
The dengue virus belongs to the genus flavivirus in the Flaviviridae family and is usually spread by mosquitos of the genus Aedes aegypti and less often Aedes albopictus.1,9 The virus is a single stranded positive sense RNA virus that exists as 4 different serotypes (DEN-1, DEN-2, DEN-3, and DEN-4),10 all of which encode 3 structural proteins and 7 non-structural proteins.4,11 The 4 viruses share approximately 65% of the genome and cause nearly identical clinical syndromes, but elicit serotype specific immune responses that do not cross-protect.1,12-14 After an incubation period of 3-7 days, dengue fever typically evolves in 3 stages: an initial febrile phase of 2-7 days, a critical phase of 1-3 days, and a spontaneous recovery phase of 3-5 days.15 The typical clinical features of dengue infection are fever, in association with headache, retro-orbital pain, myalgia and arthralgia, nausea, abdominal pain, and vomiting.16-19 More than 50% of patients are described as developing a skin rash, although the classic erythematous rash with islands of white may not be seen until the recovery phase. In the initial phase, mild hemorrhagic manifestations, tender hepatomegaly, and a fall in white cell count may be seen.19 Patients may recover without going through the critical phase. The critical phase is typified by severe abdominal pain, progressive fall in white count and platelet count, a rise in hematocrit, hemorrhagic manifestations, and radiological evidence of free fluid in the chest or abdomen. Hypovolemic shock, severe bleeding, and organ failure may be seen. Asthma, diabetes, and other chronic diseases have been suggested to be associated with increased risk of death.20-22 The most recent WHO classification recognizes mild, moderate, and severe dengue infections, severe infection being characterized by development of hemorrhagic episodes (dengue hemorrhagic fever) and hypovolemic shock (dengue shock syndrome).15 Importance of early diagnosis and treatment has been emphasized by the WHO,19 making recognition of dengue infection by admitting clinicians of paramount importance. The present study describes clinical features for all 567 cases of dengue fever presenting to Dr. Soliman Fakeeh Hospital in Jeddah, Saudi Arabia between 2010 and 2014. This is the largest series of dengue cases in Saudi Arabia for which clinical characteristics have been documented. Comparison is made between these cases and those previously described, in order to further clarify the typical presenting features of dengue in Saudi Arabia, aiding early diagnosis and optimal management.
Methods
This study is a retrospective cross-sectional where the admission and discharge diagnoses for all patients admitted to Dr. Soliman Fakeeh Hospital in Jeddah, Saudi Arabia between January 2010 and June 2014 were reviewed and 567 patients with a discharge diagnosis of dengue fever or dengue hemorrhagic fever/dengue shock syndrome were identified. Admission notes and laboratory data are stored electronically in this hospital with additional paper medical charts used for daily patient monitoring. Electronic and paper charts were reviewed for all patients. Demographic data, presenting clinical features, laboratory results including serology and dengue polymerase chain reaction (PCR) (the kits used for the serological tests were enzyme-linked immunosorbent assay [ELISA] technique, brand name was “Panbio” and “Omega Diagnostics Pathozyme” while PCR carried out by in house real time PCR [RT-PCR]) using Qiagen one-step RT-PCR kit, radiology (chest x-ray and abdominal ultrasound), clinical course, and outcome were documented. Diagnoses of dengue fever were reviewed with reference to the WHO1,23 guidelines. We included in this study any patient that was admitted during the specified period with one of the following criteria: 1) positive dengue PCR, 2)positive anti-dengue IgM or anti-dengue IgG in a patient who has fever <7 days, platelet count of <100x103 mm3 with no evidence for another infectious etiology that explains the clinical picture, and 3) International Classification of Diseases diagnosis of dengue fever at time of discharge and on review of the clinical record, either criteria 1 or 2.
One patient with acute dengue infection was excluded due to concomitant influenza A infection, making identification of the clinical features due to dengue infection impossible. We documented the presence of the typical clinical features of fever (including duration and whether was biphasic), headache, photophobia, generalized aching (including arthralgia and myalgia), abdominal pain, vomiting, lymphadenopathy, and rash. White blood cell count, platelet count, hematocrit, and alanine aminotransferase (ALT) were reviewed as parameters associated with both the diagnosis of dengue infection and development of severe dengue fever. Similarly, chest x-ray and abdominal ultrasound findings (including evidence of acalculous cholecystitis) were reviewed for evidence of plasma leakage syndrome.
Dengue hemorrhagic fever (DHF) was defined as dengue fever (as above) characterized by thrombocytopenia (≤100,000 cells per mm3), plasma leakage syndrome (pleural effusion or ascites) or a hemorrhagic tendency (spontaneous bleeding namely, petechiae, ecchymoses, or purpura, bleeding from mucosal surfaces, hematemesis, hemoptysis, epistaxis.15
Dengue shock syndrome was defined as cases meeting the criteria for dengue hemorrhagic fever who also had clinical evidence of circulatory failure.15
Results
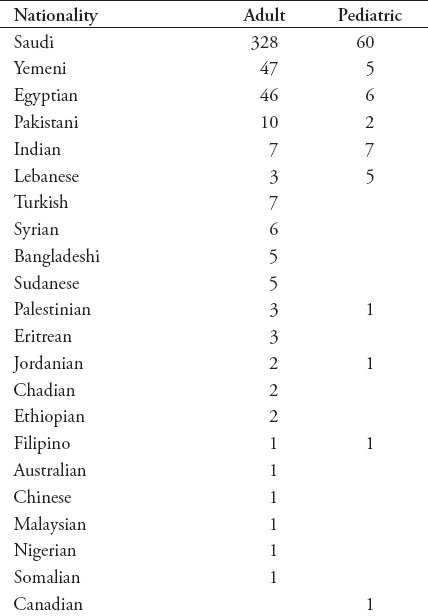
Five hundred and sixty-seven patients had a diagnosis of dengue infection. Of these, 482 were adult patients (mean age 34 years, range 14-73 years) and 85 were pediatric patients (mean age 7.1 years, range 2 months to 13 years). Sixty-seven percent of adult and 63% of pediatric patients were male. Three patients had previously been admitted with dengue fever. In each case, the 2 episodes were considered to be separate infections rather than persistent infection. Patients of 22 different nationalities were identified (Table 2). Sixty-eight percent of adult and 71% of pediatric patients were Saudi nationals.
Table 2.
Nationality of patients with dengue infection.
Clinical features
Review of travel histories confirmed that all infections were contracted in Saudi Arabia. Ninety-seven percent of patients had documented fever. The fever was monophasic in 86% of adult and pediatric patients. More than 80% of records documented the presence or absence of generalized body ache (including arthralgia and myalgia), headache, vomiting, abdominal pain, or rash. Generalized body ache was reported by 83% of patients with this symptom documented. Where documented, 36% of patients complained of headache, 40% of vomiting, 35% of abdominal pain and 26% of rash. Seventy-five percent of adult patients and 90% of pediatric patients had no co-morbidities. Forty-three adult patients had a diagnosis of diabetes mellitus, 5 of these also having a diagnosis of ischemic heart disease. Ten adult patients had a diagnosis of asthma. One patient with diabetes and one patient with asthma developed DHF. Seven patients were pregnant (including one patient with asthma) at between 15 weeks and 7 months gestation. Six pediatric patients had asthma, one of these patients also having epilepsy, one had a ventricular septal defect (VSD) and one had glucose-6-phosphate dehydrogenase (G6PD) deficiency. None of these patients developed DHF.
Laboratory investigations
In the adult population, leukopenia was typical with a mean nadir white blood cells WBC count of 2.9 (1.0-11.9) with 113 patients having a count <2. The nadir occurred a mean of 4.9 (1-19) days post onset of fever (with 19 patients not having documented fever). The mean nadir platelet count was 98 (7.0-431) with 271 patients having a count <100, 180 of whom had a nadir <80. The nadir occurred a mean of 5.6 (1-15) days post onset of fever. Two patients (count of 13 and 15) required platelet transfusions but made full recoveries without long term sequelae. In the pediatric population, the mean nadir WBC count was 4.6 (0.9-16.3) with 14 patients having a count <2. The nadir occurred a mean of 5.0 (1-21) days post onset of fever (with 5 patients not having documented fever). The mean nadir platelet count was 147 (7-523) with 31 patients having a count <100, 16 of whom had a nadir <80. The nadir occurred a mean of 5.4 (1-21) days post onset of fever.
Diagnostic investigations
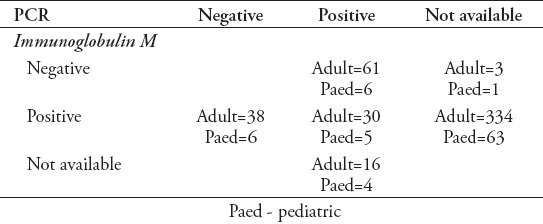
Serology was available for 466 of 482 adult patients and 81 of 85 pediatric patients (Table 3). If initial serology was negative a second acute sample was analyzed. If a second sample was taken the day of this second sample was recorded, overall serology results recorded being at a mean of 4.8 days (range 1-30 days) post onset of fever for adult patients and a mean of 4.8 days (range 1-15 days) post onset of fever for pediatric patients. Immunoglobulin G serology was also available for 56 adult patients and 4 pediatric patients including 3 adult patients and one pediatric patient for whom IgM results were not available. Polymerase chain reaction was available for 145 adult patients and 21 pediatric patients (Table 3) had a mean of 4.2 (1-13) days after onset of fever for adult and 4.3 (1-10) days after onset of fever for pediatric patients. One hundred and thirty-two adult patients and 18 pediatric patients had both serology (IgG only for 3) and PCR results available. Thirty-eight adult patients were positive for IgM with a negative PCR, 61 were negative for IgM with a positive PCR, and 30 were positive for both tests. Three patients were positive for IgG, negative for IgM with PCR not available.
Table 3.
Three additional adult patients and one pediatric patient had positive results for dengue IgG with negative IgM. Polymerase chain reaction (PCR) was not available for these patients.
Radiology
Pleural effusion on chest x-ray or the presence of ascites on abdominal ultrasound was taken as diagnostic of plasma leakage associated with severe dengue infection. It is of note that 7 adults and one pediatric patient had lobar consolidation on chest x-ray (CXR) in the absence of any other clinical features of severe dengue infection.
Clinical outcome
Data was available on hospital course, including complications, in 458 of 482 adult patients (Table 4). Eighty-three (17%) adult patients were managed as outpatients. Ninety-eight percent of adult patients made a full recovery without complications. Two patients died, one having multiorgan failure and the other due to acute respiratory distress syndrome and sepsis. Nineteen adult patients (4.1%) developed DHF with clinical evidence of bleeding including epistaxis, hemoptysis, gingival bleeding, vaginal bleeding and gastrointestinal system bleeding or radiological evidence of plasma leakage syndrome. A further patient with DHF had a ruptured spleen. One patient developed acute kidney injury, one patient developed hepatitis, one patient developed encephalitis, and one developed convulsions. Twelve adult patients (2.6%) required transfer to the intensive care unit (ICU). Nine adult patients (1.9%) developed acalculous cholecystitis. Seven adults patients (1.5%) had lobar consolidation on CXR in the absence of any other clinical features of severe dengue infection.
Table 4.
Data for full clinical course available in 458 adult and 84 pediatric patients.
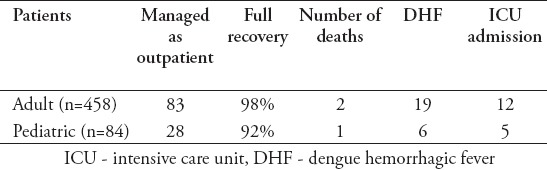
Among the pediatric population, data was available on hospital course for 84 of 85 patients including complications (Table 4). Twenty-eight (33%) pediatric patients were managed as outpatients. One patient died having developed hepatorenal syndrome. One patient developed quadriparesis due to Guillain-Barre syndrome with some residual weakness at the time of discharge. Seventy-seven patients made a full recovery. Five pediatric patients (5.9%) required transfer to the ICU with 6 developing hemorrhagic fever (7.1%) and one developing dengue shock syndrome. One pediatric patient developed a calculous cholecystitis. One pediatric patient had lobar consolidation on CXR in the absence of any other clinical features of severe dengue infection. No patients required platelet transfusions.
Considering the 19 adult patients and 6 pediatric patients who developed hemorrhagic fever, one patient had diabetes mellitus, 2 were noted to be hypertensive pre-admission, one had rheumatoid arthritis and hypothyroidism, one had thyrotoxicosis, and one had sickle cell disease and thalassemia. For the adult patients with DHF, 5 patients complained of headache at presentation, 12 complained of vomiting, 12 complained of abdominal pain, 11 complained of generalized body ache and 7 reported rashes (confirmed on examination). Thirteen patients made a full recovery without complications. Five patients had residual complications at the time of discharge with data not available for one patient. One patient in this group died. Seven patients required admission to the ICU although no patients developed shock syndrome. All patients with DHF developed thrombocytopenia (median nadir 23x103/mm3 range 9-97 at a median of 6 days after onset of fever, range 4-9 days). Ten patients had anti-dengue IgM detectable at a median of 4.5 days after onset of fever (range 3-7 days). The remaining patient had anti-dengue IgG detectable at 7 days after onset of fever. Polymerase chain reaction for dengue was only available for one patient, in whom it was positive. One of 3 pediatric patients with a diagnosis of hemorrhagic fever died. One patient developed encephalitis, with residual complications at the time of discharge.
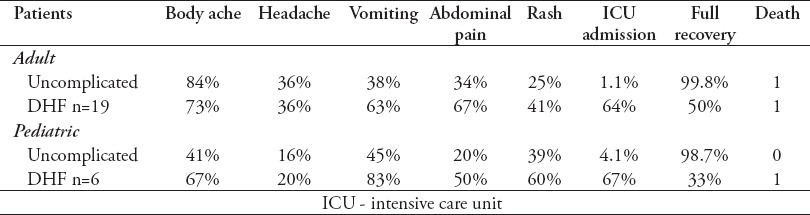
Comparing clinical findings and laboratory results in uncomplicated patients and patients who developed DHF, no clinical or laboratory parameters definitively identified patients who went on to develop hemorrhagic fever. However, vomiting and abdominal pain were more common in adult and pediatric patients who developed DHF than in patients who followed an uncomplicated course. Not surprisingly, patients who developed hemorrhagic fever were more likely to require ICU admission and less likely to make a full recovery. The nadir platelet count was lower and peak alanine aminotransferase (ALT) higher in patients who developed DHF. Two of the 3 patients who died in this study developed this syndrome, emphasizing the poor prognosis associated with development of hemorrhagic fever. None of the patients who died had significant comorbidity.
Discussion
This study describes the clinical features and outcome of 567 patients admitted with proven dengue infection to a specialty hospital in Jeddah, Saudi Arabia from 2010 to 2014. In keeping with most previous studies,24-26 85% of patients in this study were adults with a mean age of 34 years, while only 15% were children with a mean age of 7 years. Again in agreement with these previous reports, more male than female patients presented. This has been attributed to social factors by other authors27 as males, in contrast to females, predominantly work outdoors and women are more likely to be covered due to the conservative Saudi dress code. The present study showed a majority (68%) of dengue cases among Saudi nationals. Previously published work presents a range of findings in this regard. Ayyub et al28 recorded only 15% of patients presenting in Jeddah as being Saudi nationals. Aziz et al25 recorded 38% of patients as being Saudi, and Alzahrani et al (51.4%)24 and Kholedi et al (51.9%)26 reported Saudi nationals in their studies, in Jeddah. However, Alwafi et al27 reported >70% of patients identified in an epidemiological study in Makkah City to be Saudi nationals. El-Gilany et al7 reported 63.4% Saudi nationals presenting with dengue infection in Makkah City. These previously published studies suggest that differences may exist between Jeddah and Makkah City. In contrast to previous reports from Jeddah, this report has demonstrated the majority of patients presenting with clinically significant dengue infection in Jeddah to be Saudi nationals. The findings of this study; therefore, emphasized that Saudi nationals are at significant risk of dengue infection, which is important for health care profession also to recognize and may help the development of effective eradication strategies.
In the present study, DHF was manifested in 4.1% of adults and 7.1% in pediatric patients, which is in accordance with reports both from Saudi Arabia and elsewhere.28-30 El-Gilany et al7 reported a significantly higher incidence of DHF (39.43%) in a cohort of 71 patients admitted to hospital in Makkah City during the Hajj season in 2006. The higher incidence than reported here is most likely due to criteria being used by El-Gilany et al for diagnosis of DHF that are not necessarily associated with severe disease, for example, platelet count <100x103/mm3. Two hundred and seventy-two patients in our study had a nadir platelet count <100x103/mm3 of which only 11 developed DHF. This criterion cannot therefore be taken as diagnostic of severe disease, although should alert clinicians to the possibility of severe disease developing. The development of DHF is a serious complication, and it is not therefore surprising that most patients in this study with DHF were admitted to the ICU. Numbers in this series are small, but a mortality of 5.3% was seen in adult and 16.7%in pediatric patients. In terms of clinical symptoms, severe body ache, vomiting, and abdominal pain were the most commonly reported symptoms in adult and pediatric patients in both dengue infection and DHF (Table 5). In addition, skin rashes were common in pediatric cases of dengue infection and DHF. This is consistent with the previous published reports in both Saudi Arabia and internationally.28,31 In this series, vomiting and severe abdominal pain were particularly prevalent in patients developing DHF as described previously.19,32 Vomiting is relatively uncommon in patients with uncomplicated dengue infection and this clinical feature should therefore highlight the possibility of development of DHF. Consolidation on chest x-ray was an uncommon finding in our cohort of patients with dengue fever (1.4%). However, it should be noted that it can occur in this setting.
Table 5.
Comparison of uncomplicated cases with patients developing dengue hemorrhagic fever (DHF).
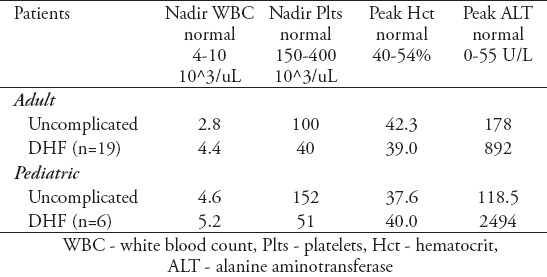
This study demonstrates thrombocytopenia and leucopenia to be characteristic of both dengue infection and DHF, counts being lowest at 5 days post onset of fever in keeping with other studies.28,33,34 Platelet counts were lower in patients developing DHF (Table 6). In-addition, more marked elevation in aminotransferases (20 to 50 fold) was recorded among patients developing DHF (adult and pediatric) than in patients with uncomplicated dengue infection (3 to 5 fold increase) (Table 6). Hepatic necrosis has been suggested to occur in DHF,35-37 and several studies reported a significant association between elevated liver enzymes and severity of dengue infection.28,38-41 It is established that evidence of plasma leakage due to increased vascular permeability is associated with an elevated hematocrit ≥20% above the population mean for age and gender or a decline in hematocrit after volume-replacement treatment of ≥20% of the baseline.23 Unfortunately serial hematocrit measurements early in the disease were not available.
Table 6.
Comparison of uncomplicated cases with patients developing dengue hemorrhagic fever (DHF).
Dengue infection was confirmed by anti-dengue virus IgM and IgG antibody ELISA and dengue virus specific PCR.42 Immunoglobulin M antibodies are first detected 3-5 days after onset of infection while IgG antibodies are detected after 14 days. The virus is present throughout but may not be associated with sufficient blood viral load to be detected by PCR. In keeping with this IgM is typically no more than 50% sensitive before day 5 post onset of fever, rising to >90% after day 5 post onset of fever. In this study, serology was more sensitive than PCR in both adult and pediatric patients (IgM serology adult [87%], pediatric [91%], PCR adult [74%], pediatric [71%]) in keeping with previous reports.43-45 This is despite the mean day of testing for serology and PCR both being <5 days, when serology might be expected to be less sensitive. We do not have sufficient data to comment on differences between serology and PCR at different time points, but these findings support the use of serology for confirmation, even at time points <5 days from onset of fever, although at these early time points it would be advisable to repeat testing or perform PCR if dengue infection is suspected and anti-dengue IgM is not detected. The lower sensitivity of PCR demonstrated here may be due to the existence of multiple serotypes in co-circulation as reported in studies conducted in Jeddah and Makkah.
Seven adult (1.5%) and one pediatric patient (1.2%) had lobar consolidation on chest x-ray without pleural effusion or clinical evidence of plasma leakage syndrome. All patients made a full recovery without development of severe dengue infection. These findings suggest that lobar consolidation may not have the same prognostic significance as radiological findings more clearly associated with plasma leakage namely, pleural effusion and ascites on abdominal ultrasound. Prior infection with dengue was reported as a risk factor for DHF in literature. In our series, 3 adult patients had confirmed prior diagnosis of dengue and did not develop DHF in subsequent infection, the sample size is too small to make valid conclusion but is worth mentioning.
Finally, complete recovery of 98% is reported among adult and 92% in pediatric patients respectively. It is noteworthy that no specific anti-viral treatments were used and only 2 patients received platelet infusions. This is in keeping with several studies reporting no benefit of high dose platelet transfusion.46 This is perhaps in keeping with direct toxic effects of infection in susceptible individuals, transfused platelets being infected as readily as endogenous platelets. There is an ever increasing need for the development of effective therapeutic interventions that can potentially reduce the duration and severity of disease, particularly in patients with DHF. Several studies assessed the potential of anti-viral drugs such as chloroquine, prednisolone, lovastatin, celgosivir, and balapiravir in modulation of immune response.47-51 No clear clinical benefit has been found for any of these agents and the current treatment strategy remains limited largely to fluid resuscitation and supportive care.23
Dengvaxia (CYD-TDV), the first dengue vaccine, was registered in Mexico in December of 2015. Dengvaxia is a live recombinant tetravalent vaccine that has been administered as a 3 dose series (0.6 and 12 months) in Phase III clinical studies. Vaccine administration has been authorized for individuals of 9-45 years of age living in endemic areas. The WHO recommends that countries should only consider introducing the vaccine on a geographical basis (nationally and sub-nationally) where epidemiological data indicates high incidence.52 Paradoxically data from studies showed a higher rate of hospitalization of Dengue in those who received the vaccine 3 years prior, than those who were not vaccinated.53 The results suggest that the vaccine causes the immune system mire susceptible making the subsequent infection more severe.52
The main limitation of this study it is a single centre experience and represents retrospective finding which cannot generalize the finding on other society. However, as all cases of dengue infection within the specified time were collected, this limitation is minimized allowing the study to add significant information about the disease manifestations in Saudi Arabia.
Acknowledgment
We would like to thank the Research-Medics for their editorial assistance in the preparation of this manuscript.
Footnotes
Statistics.
Excerpts from the Uniform Requirements for Manuscripts Submitted to Biomedical Journals updated November 2003.
Available from www.icmje.org
Describe statistical methods with enough detail to enable a knowledgeable reader with access to the original data to verify the reported results. When possible, quantify findings and present them with appropriate indicators of measurement error or uncertainty (such as confidence intervals). Avoid relying solely on statistical hypothesis testing, such as the use of P values, which fails to convey important information about effect size. References for the design of the study and statistical methods should be to standard works when possible (with pages stated). Define statistical terms, abbreviations, and most symbols. Specify the computer software used.
References
- 1.Bhatt S, Gething PW, Brady OJ, Messina JP, Farlow AW, Moyes CL, et al. The global distribution and burden of dengue. Nature. 2013;496:504–507. doi: 10.1038/nature12060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Brady OJ, Gething PW, Bhatt S, Messina JP, Brownstein JS, Hoen AG, et al. Refining the global spatial limits of dengue virus transmission by evidence-based consensus. PLoS Negl Trop Dis. 2012;6:e1760. doi: 10.1371/journal.pntd.0001760. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Fakeeh M, Zaki AM. Virologic and serologic surveillance for dengue fever in Jeddah, Saudi Arabia, 1994-1999. Am J Trop Med Hyg. 2001;65:764–767. doi: 10.4269/ajtmh.2001.65.764. [DOI] [PubMed] [Google Scholar]
- 4.Guzman MG, Halstead SB, Artsob H, Buchy P, Farrar J, Gubler DJ, et al. Dengue: a continuing global threat. Nat Rev Microbiol. 2010;8(12 Suppl):S7–S16. doi: 10.1038/nrmicro2460. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Fakeeh M, Zaki AM. Dengue in Jeddah, Saudi Arabia. Dengue Bulletin. 2003;27:1994–2002. [Google Scholar]
- 6.Alhaeli A, Bahkali S, Ali A, Househ MS, El-Metwally AA. The epidemiology of Dengue fever in Saudi Arabia: A systematic review. J Infect Public Health. 2016;9:117–124. doi: 10.1016/j.jiph.2015.05.006. [DOI] [PubMed] [Google Scholar]
- 7.El-Gilany AH, Eldeib A, Hammad S. Clinico-epidemiological features of dengue fever in Saudi Arabia. Asian Pac J Trop Med. 2010;3:220–223. [Google Scholar]
- 8.Zaki A, Perera D, Jahan SS, Cardosa MJ. Phylogeny of dengue viruses circulating in Jeddah Saudi Arabia:1994 to 2006. Trop Med Int Health. 2008;13:584–592. doi: 10.1111/j.1365-3156.2008.02037.x. [DOI] [PubMed] [Google Scholar]
- 9.Paupy C, Delatte H, Bagny L, Corbel V, Fontenille D. Aedes albopictus, an arbovirus vector: from the darkness to the light. Microbes Infect. 2009;11:1177–1185. doi: 10.1016/j.micinf.2009.05.005. [DOI] [PubMed] [Google Scholar]
- 10.Calisher CH, Karabatsos N, Dalrymple JM, Shope RE, Porterfield JS, Westaway EG, et al. Antigenic relationships between flaviviruses as determined by cross-neutralization tests with polyclonal antisera. J Gen Virol. 1989;70(Pt 1):37–43. doi: 10.1099/0022-1317-70-1-37. [DOI] [PubMed] [Google Scholar]
- 11.Yacoub S, Mongkolsapaya J, Screaton G. Recent advances in understanding dengue. F1000Res. 2016;5:5. doi: 10.12688/f1000research.6233.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Halstead SB. Pathogenesis of dengue: challenges to molecular biology. Science. 1988;239:476–481. doi: 10.1126/science.3277268. [DOI] [PubMed] [Google Scholar]
- 13.Kurane I. Dengue hemorrhagic fever with special emphasis on immunopathogenesis. Comp Immunol Microbiol Infect Dis. 2007;30:329–340. doi: 10.1016/j.cimid.2007.05.010. [DOI] [PubMed] [Google Scholar]
- 14.Halstead SB. Dengue virus-mosquito interactions. Annu Rev Entomol. 2008;53:273–291. doi: 10.1146/annurev.ento.53.103106.093326. [DOI] [PubMed] [Google Scholar]
- 15.Simmons CP, Farrar JJ, Nguyen V, Wills B. Dengue. N Engl J Med. 2012;366:1423–1432. doi: 10.1056/NEJMra1110265. [DOI] [PubMed] [Google Scholar]
- 16.Ahmed FU, Mahmood CB, Sharma JD, Hoque SM, Zaman R, Hasan MS. “Dengue and dengue haemorrhagic fever in children during the 2000 outbreak in Chittagong, Bangladesh,”. Dengue Bulletin. 2001;25:33–39. [Google Scholar]
- 17.Narayanan M, Aravind MA, Thilothammal N, Prema R, Sargunam CS, Ramamurty N. Dengue fever epidemic in Chennai - a study of clinical profile and outcome. Indian Pediatr. 2002;39:1027–1033. [PubMed] [Google Scholar]
- 18.Rigau-Pérez JG, Clark GG, Gubler DJ, Reiter P, Sanders EJ, Vorndam AV. Dengue and dengue haemorrhagic fever. Lancet. 1998;352:971–977. doi: 10.1016/s0140-6736(97)12483-7. [DOI] [PubMed] [Google Scholar]
- 19.World Health Organization. Handbook for clinical management of dengue. Handbook for clinical management of dengue. Geneva: WHO; 2012. [Google Scholar]
- 20.Halstead SB, Nimmannitya S, Cohen SN. Observations related to pathogenesis of dengue hemorrhagic fever. IV. Relation of disease severity to antibody response and virus recovered. Yale J Biol Med. 1970;42:311–328. [PMC free article] [PubMed] [Google Scholar]
- 21.Kouri GP, Guzmán MG, Bravo JR. Why dengue haemorrhagic fever in Cuba? 2. An integral analysis. Trans R Soc Trop Med Hyg. 1987;81:821–823. doi: 10.1016/0035-9203(87)90042-3. [DOI] [PubMed] [Google Scholar]
- 22.Lee MS, Hwang KP, Chen TC, Lu PL, Chen TP. Clinical characteristics of dengue and dengue hemorrhagic fever in a medical center of southern Taiwan during the 2002 epidemic. J Microbiol Immunol Infect. 2006;39:121–129. [PubMed] [Google Scholar]
- 23.World Health Organization. Research SPf, Diseases TiT, Diseases WHODoCoNT, Epidemic WHO, Alert P. Dengue: guidelines for diagnosis, treatment, prevention and control. Geneva: WHO; 2009. [PubMed] [Google Scholar]
- 24.Alzahrani AG, Al Mazroa MA, Alrabeah AM, Ibrahim AM, Mokdad AH, Memish ZA. Geographical distribution and spatio-temporal patterns of dengue cases in Jeddah Governorate from 2006-2008. Trans R Soc Trop Med Hyg. 2013;107:23–29. doi: 10.1093/trstmh/trs011. [DOI] [PubMed] [Google Scholar]
- 25.Aziz AT, Al-Shami SA, Mahyoub JA, Hatabbi M, Ahmad AH, Rawi CS. An update on the incidence of dengue gaining strength in Saudi Arabia and current control approaches for its vector mosquito. Parasit Vectors. 2014;7:258. doi: 10.1186/1756-3305-7-258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Kholedi AA, Balubaid O, Milaat W, Kabbash IA, Ibrahim A. Factors associated with the spread of dengue fever in Jeddah Governorate, Saudi Arabia. East Mediterr Health J. 2012;18:15–23. doi: 10.26719/2012.18.1.15. [DOI] [PubMed] [Google Scholar]
- 27.Alwafi OM, McNabb S, Memish ZA, Assiri A, Alzahrani SH, Asiri SA, et al. Dengue Fever in Makkah, Kingdom of Saudi Arabia, 2008-2012. American Journal of Research Communication. 2013;1:123–139. [Google Scholar]
- 28.Ayyub M, Khazindar AM, Lubbad EH, Barlas S, Alfi AY, Al-Ukayli S. Characteristics of dengue fever in a large public hospital, Jeddah, Saudi Arabia. J Ayub Med Coll Abbottabad. 2006;18:9–13. [PubMed] [Google Scholar]
- 29.Khan NA, Azhar EI, El-Fiky S, Madani HH, Abuljadial MA, Ashshi AM, et al. Clinical profile and outcome of hospitalized patients during first outbreak of dengue in Makkah, Saudi Arabia. Acta Trop. 2008;105:39–44. doi: 10.1016/j.actatropica.2007.09.005. [DOI] [PubMed] [Google Scholar]
- 30.Sung V, O'Brien DP, Matchett E, Brown GV, Torresi J. Dengue Fever in travelers returning from southeast Asia. J Travel Med. 2003;10:208–213. doi: 10.2310/7060.2003.40555. [DOI] [PubMed] [Google Scholar]
- 31.Kabra SK, Jain Y, Pandey RM, Madhulika Singhal T, Tripathi P, et al. Dengue haemorrhagic fever in children in the 1996 Delhi epidemic. Trans R Soc Trop Med Hyg. 1999;93:294–298. doi: 10.1016/s0035-9203(99)90027-5. [DOI] [PubMed] [Google Scholar]
- 32.Lum L, Ng C, Khoo E. Managing dengue fever in primary care: A practical approach. Malays Fam Physician. 2014;9:2–10. [PMC free article] [PubMed] [Google Scholar]
- 33.García S, Morales R, Hunter RF. Dengue fever with thrombocytopenia: studies towards defining vulnerability of bleeding. Bol Asoc Med P R. 1995;87:2–7. [PubMed] [Google Scholar]
- 34.Jyothi P, Metri BC. Correlation of serological markers and platelet count in the diagnosis of Dengue virus infection. Adv Biomed Res. 2015;4:26. doi: 10.4103/2277-9175.150396. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Huerre MR, Lan NT, Marianneau P, Hue NB, Khun H, Hung NT, et al. Liver histopathology and biological correlates in five cases of fatal dengue fever in Vietnamese children. Virchows Arch. 2001;438:107–115. doi: 10.1007/s004280000329. [DOI] [PubMed] [Google Scholar]
- 36.Lin YL, Liu CC, Lei HY, Yeh TM, Lin YS, Chen RM, et al. Infection of five human liver cell lines by dengue-2 virus. J Med Virol. 2000;60:425–431. doi: 10.1002/(sici)1096-9071(200004)60:4<425::aid-jmv10>3.0.co;2-a. [DOI] [PubMed] [Google Scholar]
- 37.World Health Organization. Dengue haemorrhagic fever: diagnosis, treatment, prevention and control. Geneva: WHO; 1997. [Google Scholar]
- 38.Nimmannitya S, Suntayakom S, Vaughn D, Nisalak A, Green S, Chansiriwongs V, et al. Can doctors make an accurate diagnosis of dengue infections at an early stage. Dengue Bulletin. 1999:23. [Google Scholar]
- 39.Mohan B, Patwari AK, Anand VK. Hepatic dysfunction in childhood dengue infection. J Trop Pediatr. 2000;46:40–43. doi: 10.1093/tropej/46.1.40. [DOI] [PubMed] [Google Scholar]
- 40.Pancharoen C, Rungsarannont A, Thisyakorn U. Hepatic dysfunction in dengue patients with various severity. J Med Assoc Thai. 2002;85(Suppl1):S298–S301. [PubMed] [Google Scholar]
- 41.Petdachai W. Hepatic Dysfunction in Children with Dengue Shock Syndrome. Dengue Bulletin. 2005;29:112–118. [Google Scholar]
- 42.Lanciotti RS, Calisher CH, Gubler DJ, Chang GJ, Vorndam AV. Rapid detection and typing of dengue viruses from clinical samples by using reverse transcriptase-polymerase chain reaction. J Clin Microbiol. 1992;30:545–551. doi: 10.1128/jcm.30.3.545-551.1992. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Cardosa MJ, Tio PH, Nimmannitya S, Nisalak A, Innis B. IgM capture ELISA for detection of IgM antibodies to dengue virus: comparison of 2 formats using hemagglutinins and cell culture derived antigens. Southeast Asian J Trop Med Public Health. 1992;23:726–729. [PubMed] [Google Scholar]
- 44.Gubler D, Sather G. Laboratory diagnosis of dengue and dengue hemorrhagic fever. Simpósio Internacional sobre Febre Amarela e Dengue. 1988;15:291–322. [Google Scholar]
- 45.Innis BL, Nisalak A, Nimmannitya S, Kusalerdchariya S, Chongswasdi V, Suntayakorn S, et al. An enzyme-linked immunosorbent assay to characterize dengue infections where dengue and Japanese encephalitis co-circulate. Am J Trop Med Hyg. 1989;40:418–427. doi: 10.4269/ajtmh.1989.40.418. [DOI] [PubMed] [Google Scholar]
- 46.Khan Assir MZ, Kamran U, Ahmad HI, Bashir S, Mansoor H, Anees SB, et al. Effectiveness of platelet transfusion in dengue Fever: a randomized controlled trial. Transfus Med Hemother. 2013;40:362–368. doi: 10.1159/000354837. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Low JG, Sung C, Wijaya L, Wei Y, Rathore AP, Watanabe S, et al. Efficacy and safety of celgosivir in patients with dengue fever (CELADEN): a phase 1b, randomised, double-blind, placebo-controlled, proof-of-concept trial. Lancet Infect Dis. 2014;14:706–715. doi: 10.1016/S1473-3099(14)70730-3. [DOI] [PubMed] [Google Scholar]
- 48.Nguyen NM, Tran CN, Phung LK, Duong KT, Huynh HA, Farrar J, et al. A randomized, double-blind placebo controlled trial of balapiravir, a polymerase inhibitor, in adult dengue patients. J Infect Dis. 2013;207:1442–1450. doi: 10.1093/infdis/jis470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Tam DT, Ngoc TV, Tien NT, Kieu NT, Thuy TT, Thanh LT, et al. Effects of short-course oral corticosteroid therapy in early dengue infection in Vietnamese patients: a randomized, placebo-controlled trial. Clin Infect Dis. 2012;55:1216–1224. doi: 10.1093/cid/cis655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Tricou V, Minh NN, Van TP, Lee SJ, Farrar J, Wills B, et al. A randomized controlled trial of chloroquine for the treatment of dengue in Vietnamese adults. PLoS Negl Trop Dis. 2010;4:e785. doi: 10.1371/journal.pntd.0000785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Whitehorn J, Van Vinh Chau N, Truong NT, Tai LT, Van Hao N, Hien TT, et al. Lovastatin for adult patients with dengue: protocol for a randomised controlled trial. Trials. 2012;13:203. doi: 10.1186/1745-6215-13-203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Ferguson NM, Rodríguez-Barraquer I, Dorigatti I, Mier-Y-Teran-Romero L, Laydon DJ, Cummings DA. Benefits and risks of the Sanofi-Pasteur dengue vaccine: modeling optimal deployment. Science. 2016;353:1033–1036. doi: 10.1126/science.aaf9590. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Hadinegoro SR, Arredondo-García JL, Capeding MR, Deseda C, Chotpitayasunondh T, Dietze R, et al. CYD-TDV Dengue Vaccine Working Group. Efficacy and long-term safety of a dengue vaccine in regions of endemic disease. N Engl J Med. 2015;373:1195–1206. doi: 10.1056/NEJMoa1506223. [DOI] [PubMed] [Google Scholar]
- 54.Shahin W, Nassar A, Kalkatttawi M, Bokhari H. Dengue fever in a tertiary hospital in Makkah, Saudi Arabia. Dengue Bulletin. 2009;33:34–43. [Google Scholar]