

Abstract
Objectives:
To assess the consumption of sweets, carbonated beverages, and energy drinks along with their correlates among primary school children.
Methods:
A total of 725 children (7-12 years old) were randomly recruited from 10 elementary schools from Al-Baha city, Saudi Arabia in 2013, using a multi-stage stratified sampling technique and pre-tested validated questionnaire.
Results:
Approximately 26.1% of children reported consuming sweets on daily basis, and 63.4% consumed sweets occasionally during the week. Approximately 56.3% children were reportedly drinking carbonated beverages weekly and 17.1% in daily basis. Weekly consumption of energy drinks was reported in 21.9% and daily consumption in 4.3% of the children. Daily sweets consumption was positively associated with children age (odds ratio [OR]=1.5, 95% confidence interval [CI]: 4.5-9.5, p=0.035), consuming carbonated beverages (OR=3.4, 95% CI: 2.2-5.2, p<0.001), energy drinks (OR=2.5, 95% CI: 1.1-5.4, p=0.029), eating high fat food (OR= 1.6, 95% CI: 1.1 - 2.4, p=0.023), and inversely with children body mass index (BMI) (OR=0.9, 95% CI: 0.8-0.9, p<0.001). Consuming carbonated beverages on regular basis was positively associated with consuming energy drinks (OR=9.0, 95% CI: 4.0-21.0, p<0.001).
Conclusion:
Unhealthy dietary choices were found to be prevalent at early age. Comprehensive intervention programs should be established to prevent unhealthy dietary choices and promote healthier dietary behaviors. Qualitative studies are needed for better understanding of children’s dietary behaviors.
Childhood is a unique stage of human lifecycle, in which a child experience critical growth and development physiologically, psychologically, and socially. For ensuring adequate growth and development, it is recommended to develop healthy dietary behaviors that results in better health status. A healthy diet is helpful for the children to reduce the risk of malnutrition in all its forms as well as protects health against many types of noncommunicable diseases, including obesity, diabetes, cardiovascular diseases, and some types of cancer.1 However, the dietary habits have changed as a result of industrialization, urbanization, and globalization. Unfortunately, poor nutritional diet (for example soft drinks, sugary snacks, sports and energy drinks) has replaced the healthy diet (for example milk, vegetables and fruit), especially among the children. The World Health Organization has showed that poor dietary behaviors have emerged as a risk towards health.1
The consumption of softdrink and carbonated drinks is popular in the modern society. Specifically, the consumption of soft carbonated drinks is popular among school children and adolescents. It has been further evaluated that excessive consumption of carbonated soft drinks is witnessed among children (6 to 15 years old). Moreover, 97.9% of the girls and 97.3% of the boys have also reported that they consume soft drinks on weekly basis.2 Moreover, frequent/weekly consumption of sweets and chocolate were more than 95% among both boys and girls.2 Similarly, daily candy/chocolate consumption was 37% for male and 52% for female Saudi adolescents.3 It has been reported that the increased consumption of sweets and carbonated drinks among male school children (10-14 years) in Saudi Arabia consequently increased the reporting of obesity and overweight.4 Children and adolescents with higher intakes of carbonated beverages could be at increased risk of metabolic syndrome, abdominal obesity, and hypertension.5 Moreover, carbonated beverages were found to be significantly associated with waist circumference, triglyceride level, and blood pressure.6 Therefore, it has been suggested that sugar intake should be reduced throughout the life course.7
Consumption of energy drinks is prevalent among adolescents with the growing market of energy drinks.8 In a review study, it has been reported that energy drinks are consumed by 30% to 50% school aged children.9 The consumption of energy drinks increases the risk of caffeine overdose and toxicity among children and teenagers.9,10 Moreover, it has been reported that high density sugar beverages consumption has increased dramatically in the United States, in parallel with the epidemic of type 2 diabetes, overweight, and obesity.11 Energy drinks are commonly available in Saudi market. However, the data regarding consuming energy drinks among school children is extremely rare.
The aim of nutritional assessment in childhood is to identify unhealthy dietary behaviors and their negative outcomes and correlates. Limited data is present regarding the consumption of sweets, carbonated-soft beverages, and energy drinks among children in Saudi Arabia. Therefore, this study has aimed to address the gap in previous literature and to increase awareness about the consumption of sweets, carbonated beverages and energy drinks and their associations among school children in Baha city, Saudi Arabia.
Methods
Study setting and sampling procedure
A random sample of 725 school children was recruited, aged 7 to 12 years, from 10 primary schools of Al-Baha city, Saudi Arabia in 2013. The study was conducted among elementary schools, using multi-stage probability proportional to size sampling technique. This cross-sectional study was carried out to evaluate the consumptions of sweet products, carbonated beverages, and energy drinks among children. An ethical approval was obtained from research review board, and administrative permission was taken from the Ministry of Education.
Data collection
Literature searches were conducted with PubMed and Google Scholar to find similar studies. The assessment of daily consumptions of sweets, carbonated beverages and energy drinks was investigated using food frequency questionnaire (FFQ) of the food type inquiring only about frequencies without specification to portion size. The 6 response categories were: never/seldom, sometimes during the weekdays, one time per day, 2 times per day, 3 to 4 times per day, and 5 serving or more per day. The responses were dichotomized for further regression analyses to daily consumption (namely 1 or more a day) versus no daily consumption (namely never/not daily). Body mass index (BMI) was calculated using the equation BMI = (weight [kg]/height [m2]).
The questionnaire was pretested through a pilot study, which was performed among 32 school children of the similar age as the main study participants. It has been found that the Saudi children were not aware of their family socioeconomic status; such as their parents’ education level and family income, which limit the analyses.
The aim and the importance of the study were explained to students. They were also informed that their contribution to the study is totally voluntary and they could quit at any moment. Questionnaire was read aloud for children to clarify the meaning of questions and to help them in filling up the questionnaire. Questionnaire was administered and collected in classrooms during regular class time; thus, it took approximately 30 to 45 minutes. Students were assured that the information would remain confidential and anonymous; thus, they were encouraged to be honest in their answers. Moreover, privacy was ensured, and school staff was asked to not enter the classrooms, where the children filled the questionnaire, aiming to prevent the tendency in the favor of socially acceptable behavior. The participants were encouraged to approach the examiner, whenever they needed clarification at any issue. All students in the selected schools have the similar chances to be included in the study.
Statistical analysis
The data has been analyzed using SPSS Statistics for Windows, Version 22.0 (Armonk, NY: IBM Corp.). Chi-square test was used to determine association of students’ age with regards to sweets, soft-carbonated, and energy drinks consumptions. Moreover, binary regression analysis for daily consumptions of sweets, carbonated beverages and energy drinks was performed to investigate its associations with certain dietary behaviors; such as, consuming high fat food, fast food, and other health outcome (BMI). Odds ratios (OR) and 95% confidence interval (CI) were stated, and p-value of 0.05 was used as a level of statistical significance.
Results
Table 1 presents the age distribution of participated school children. The sample was comprised of 725 children. The mean age of school children was 9.8 years (SD ± 1.6), ranged between 7-12 years old.
Table 1.
Age distributions of 725 school children participated in the study.
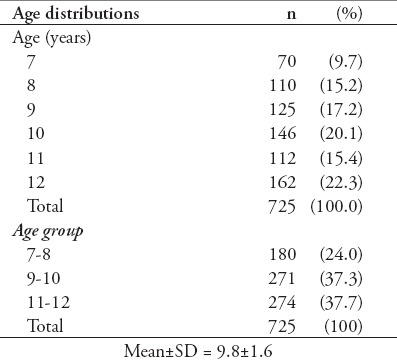
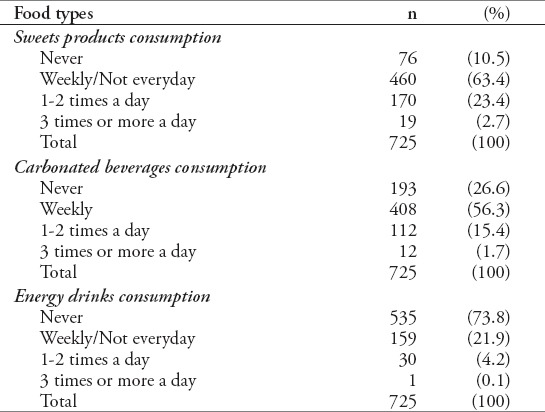
Table 2 shows that 63.4% of the children never or rarely consumed sweets products during the week, and only 26.1% of the children reported consuming sweets products at least once daily. Approximately 56.3% of the children consumed soft drinks weekly; whereas, 17.1% were daily consumers. Weekly consumption of energy drinks were reported by 21.9% of the children, and by 4.3% as a daily users.
Table 2.
Distributions of sweets products, soft and energy drinks consumption among school children.
The association between age and frequency of sweets products, carbonated soft-beverages, and energy drinks daily consumption was calculated by Chi-square test (Table 3). Table 3 shows that the daily consumption of sweets (p=0.018) and soft drinks (p=0.017) were more prevalent among older age. Moreover, the daily consumption of energy drinks tends to increase with an increase in children age, since 2.2% of the 7-8 year children, 6.3% of the 9-10 year and 3.6% of the 11-12 years were daily users, but the deference was not significant (p=0.083).
Table 3.
Distributions and association of sweet foods, soft drink, and energy drinks consumption with regard to children’s age-specific.
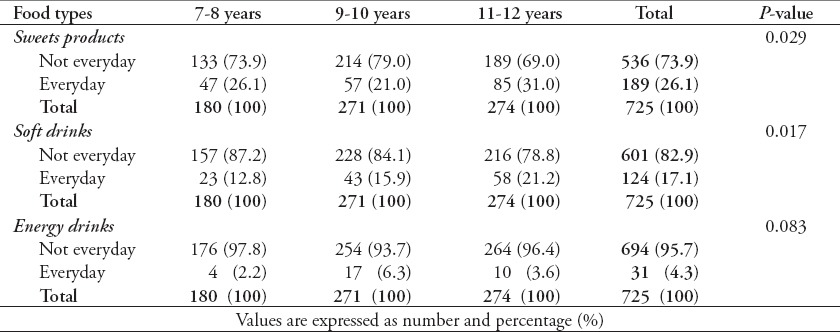
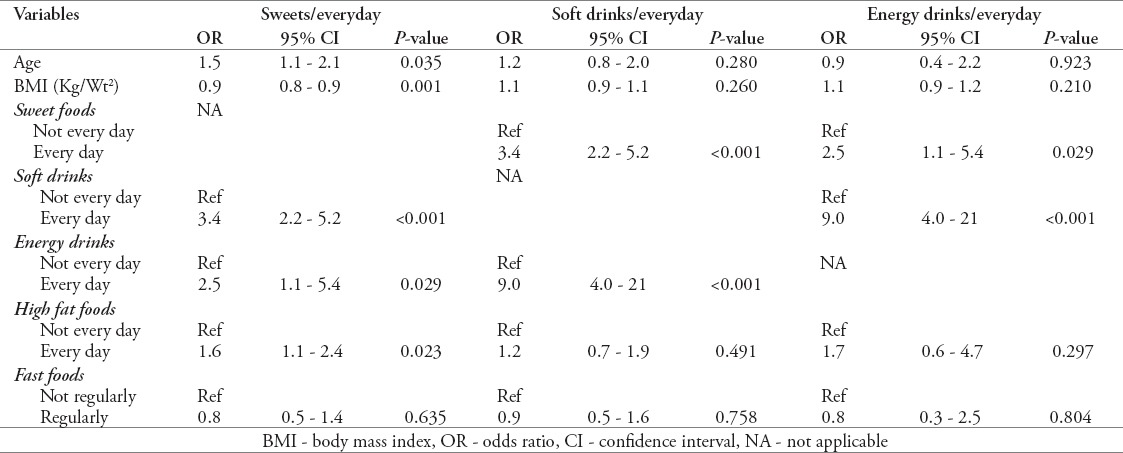
Table 4 represents the binary logistic regression analyses of unhealthy food groups, associated with many dietary behaviors. The analyses showed that consuming sweet foods daily was positively associated with increased child’s age (OR=1.5, 95% CI: 1.1-2.1, p=0.035), consuming soft drinks (OR= 3.4, 95% CI: 2.2-5.2, p<0.001), energy drinks consumption (OR= 2.5, 95% CI: 1.1-5.4, p=0.029), and eating high fat food (OR= 1.6, 95% CI: 1.1-2.4, p=0.023) on daily basis. On the contrary, it was inversely associated with children body mass index (BMI) (OR= 0.9, 95% CI: 0.8-0.9, p=0.001). Moreover, the daily consumption of carbonated beverages was positively associated with consuming energy drinks daily (OR= 9.0, 95% CI: 4.0-21.0, p<0.001).
Table 4.
Regression analyses of daily consumption of sweet foods, carbonated drinks and energy drinks with regards to their correlates among children.
Discussion
The current cross-sectional questionnaire survey was conducted with the aim of assessing the consumption of sweets, soft-carbonated, and energy drinks along with their correlation among Saudi school children. This study revealed that energy drinks, at early age, is far worrying. The consumption of energy drinks may increase the possibility of caffeine overdose and toxicity among children and teenagers.10 In this study, weekly and daily consumers of energy drinks were reported to be 26.2% of total school children. The results of this study provided an evidence that the consumption of energy drinks is common among younger population in Saudi Arabia. Similarly, it has been reported that 45% of school children, aged 12 to 19 years, consumed energy drinks in Saudi Arabia.11 At the same time, it has been reported that the frequent consumption of energy drinks was reported by 16% of the students among high school students.8 In a review study, the consumption of energy drinks was reported to be 30% to 50% by adolescents and young adults.9 It may strongly indicate that energy drinks consumption tends to increase as age increases, which highlighted the importance of this study and the need to tackle unhealthy behavior among school children. Such findings would serve as a baseline for future studies related to energy drinks consumption among children in Saudi Arabia and Arab Gulf countries. The most common reasons for consuming energy drinks were friends, taste, curiosity, boosting energy, and advertisement.12,13
The findings have also indicated higher consumption of sweets products and sweetened-carbonated soft drinks among children, suggesting a trend towards sugar-rich foods among children. In this study, it is evident that sweet products and sweetened carbonated beverages were regularly consumed by most Saudi children. In line with that, it has been reported that unhealthy dietary choices; such as, sweet food consumption and sweetened beverages were most often consumed among school children in Saudi Arabia.3 Also, it has been described that carbonated drinks are the major types of sweetened beverages, consumed by the school children.11 Similarly, it has been also reported that the consumption of sugar-sweetened beverages was higher among older versus younger children, signifying a trend towards sugar-rich foods with advancing age.14 However, it has been reported that there was a negative relationship between sweetened beverage consumption and water intake,15 which suggested future research to investigate water consumption and its determinates among Saudi population.
As represented in Table 4, unhealthy food consumptions were clustered and correlated with many outcomes. Furthermore, this study found that consuming sweets on daily basis was associated positively with consuming soft drinks daily, energy drinks, and eating high fat food. Moreover, consuming carbonated soft drinks daily was also associated positively with consuming energy drinks. Similarly, it has also been found that the consumption of sweets products was correlated significantly with consuming sweetened-soft drinks, energy drinks, and fast food in Saudi Arabia.3 Also, sweetened carbonated beverages consumption was found to be positively associated with unhealthy dietary behaviors; such as, fast food meal intake and sugar intake.14 A systematic review study reported positive associations between regular carbonated soft consumption and lower levels of exercise, high levels of TV watching, low vegetable intake, and high fast-food consumption.16 Moreover, daily carbonated soft beverages consumption was associated with eating snacks, while watching television and with regular meal consumption in a fast food restaurant.17 Such findings provided a clear evidence that unhealthy dietary behaviors are clustered among children, and their collective negative effect might be critical to children’s health and to their life in future. The unhealthy dietary choices may often lead to many health and medical problems; some of which can cause permanent damage.1,5-7,9,10,19-23
Also, the binary logistic analyses showed that consuming sweets on daily basis was associated positively with increased children age and negatively with children BMI. Children with lower BMI tend to consume sugar daily as compared to higher BMIs children. A negative relationship between sugar intake and BMI was reported among Saudi adolescents and elsewhere.3,24,25 One possible explanation is that people with higher BMIs may tend to avoid or consume less sugar as a method to lose some body weight.
The presented findings have important implication for public health practice. There is a co-occurrence of multiple poor dietary behaviors, which may increase the risk of chronic disease and poor health outcomes. Strategies to improve children’s dietary behaviors in both the school and home environment are needed to be implemented. School-based nutrition education can make a vital contribution to healthy eating. Schools are particularly suitable for nutrition education, because they reach most children, on a regular basis, for a number of years. Therefore, progressive changes within the academic environment or educational processes may lead to the application of healthy behaviors. It has been evaluated that productive policies along with the supportive environment is associated with healthy food choices.26 Thus, school policies, promoting healthy food choices and healthier behaviors choices, are required in Saudi Arabia. To have a greater impact on children’s dietary behaviors, any program implemented should include parents and family component. Parents can influence their children dietary behaviors accordingly. They are the decision makers, and can be seen as role models for their children; therefore, they should be included in any healthy lifestyle program targeting children. Numerous nutritional and behavioral studies have suggested that parental modeling and home-environmental; such as availability and accessibility factors, are associated with children nutritional behaviors.27-30 Thus, interventions, including all the members of the family, are necessary to have a greater impact in improving children’s dietary behaviors.
Study limitations
There are some limitations that ought to be highlighted. Firstly, this study was conducted in 2013 and the design (cross-sectional) did not allow the establishment of causal relationship. Secondly, sweet, soft-carbonated beverages, and energy drinks were assessed by self-reported questionnaire, which might be subjected to over reporting or under-reporting. Moreover, the researcher was limited to obtain information about the socioeconomic condition of the family because of younger participants. At the same time, the factors, related with parents’ education level, family dietary behaviors, and family economic status and students’ dietary behaviors were not examined.
In conclusion, healthy diet is considered as an important pillar for health and education. This study revealed that a high proportion of children consumed a relatively high amount of sweets, sweetened-carbonated beverages, and energy drinks. Moreover, it is evident that unhealthy dietary behaviors were prevalent, clustered, and started at early age among Saudi children. Therefore, there is a need to prevent the unhealthy dietary behaviors among children at early years. Schools can play a significant role in enhancing students’ knowledge regarding the importance of healthy diet, and influence their nutritional behaviors. Thus, Saudi Ministry of Education should play an active role in developing and promoting healthier dietary behaviors through comprehensive school-based intervention programs. Further in-depth descriptive studies are needed to provide more comprehensive understanding of children’s dietary behaviors and their correlates.
Footnotes
References
- 1.World Health Organization. Healthy diet. Fact sheet N. 394. Geneva: World Health Organization; 2015. [Google Scholar]
- 2.Quadri FA, Hendriyani H, Pramono A, Jafer M. Knowledge, attitudes and practices of sweet food and beverage consumption and its association with dental caries among schoolchildren in Jazan, Saudi Arabia. East Mediterr Health J. 2015;21:403–411. doi: 10.26719/2015.21.6.403. [DOI] [PubMed] [Google Scholar]
- 3.Al-Hazzaa HM, Abahussain NA, Al-Sobayel HI, Qahwaji DM, Musaiger AO. Physical activity, sedentary behaviors and dietary habits among Saudi adolescents relative to age, gender and region. Int J Behav Nutr Phys Act. 2011;8:140. doi: 10.1186/1479-5868-8-140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Amin TT, Al-Sultan AI, Ali A. Overweight and obesity and their relation to dietary habits and socio-demographic characteristics among male primary school children in Al-Hassa, Kingdom of Saudi Arabia. Eur J Nutr. 2008;47:310–318. doi: 10.1007/s00394-008-0727-6. [DOI] [PubMed] [Google Scholar]
- 5.Mirmiran P, Yuzbashian E, Asghari G, Hosseinpour-Niazi S, Azizi F. Consumption of sugar sweetened beverage is associated with incidence of metabolic syndrome in Tehranian children and adolescents. Nutrition &Metabolism. 2015;12:25. doi: 10.1186/s12986-015-0021-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ejtahed HS, Bahadoran Z, Mirmiran P, Azizi F. Sugar-sweetened beverage consumption is associated with metabolic syndrome in Iranian adults: Tehran lipid and glucose study. Endocrinol Metab (Seoul) 2015;30:334–342. doi: 10.3803/EnM.2015.30.3.334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.World Health Organization. Guideline: Sugars intake for adults and children. Geneva: World Health Organization; 2015. [PubMed] [Google Scholar]
- 8.Nowak D, Jasionowski A. Analysis of the consumption of caffeinated energy drinks among Polish adolescents. Int J Environ Res Public Health. 2015;12:7910–7921. doi: 10.3390/ijerph120707910. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Seifert SM, Schaechter JL, Hershorin ER, Lipshultz SE. Health effects of energy drinks on children, adolescents, and young adults. Pediatrics. 2011;127:511–528. doi: 10.1542/peds.2009-3592. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bigard AX. Risks of energy drinks in youths. Arch Pediatr. 2010;17:1625–1631. doi: 10.1016/j.arcped.2010.08.001. [DOI] [PubMed] [Google Scholar]
- 11.Bleich SN, Wang YC, Wang Y, Gortmaker SL. Increasing consumption of sugar-sweetened beverages among US adults 1988-1994 to 1999-2004. Am J Clin Nutr. 2009;89:372–381. doi: 10.3945/ajcn.2008.26883. [DOI] [PubMed] [Google Scholar]
- 12.Musaiger AO, Zagzoog N. Knowledge, attitudes and practices toward energy drinks among adolescents in Saudi Arabia. Glob J Health Sci. 2014;27:42–46. doi: 10.5539/gjhs.v6n2p42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ibrahim NK, Iftikhar R, Murad M, Fida H, Abalkhaeil B, Al Ahmadi J. Energy drinks consumption amongst medical students and interns from three colleges in Jeddah, Saudi Arabia. Journal of Food and Nutrition Research. 2014;2:174–179. [Google Scholar]
- 14.Collison KS, Zaidi MZ, Subhani SN, Al-Rubeaan K, Shoukri M, Al-Mohanna FA. Sugar-sweetened carbonated beverage consumption correlates with BMI, waist circumference, and poor dietary choices in school children. BMC Public Health. 2010;10:234. doi: 10.1186/1471-2458-10-234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Cullen KW, Eagan J, Baranowski T, Owens E. Effect of a la carte and snack bar foods at school on children's lunchtime intake of fruits and vegetables. J Am Diet Assoc. 2000;100:1482–1486. doi: 10.1016/s0002-8223(00)00414-4. [DOI] [PubMed] [Google Scholar]
- 16.Rao G, Kirley K, Weiss-Coleman R, Inman JJ, Bauer V, Zhou Y, Wang C, Hledin V. Consumption Patterns of Sugar-Sweetened Carbonated Beverages Among Children and Adolescents. Curr Cardiovasc Risk Rep. 2015;9:17. [Google Scholar]
- 17.Verzeletti C, Maes L, Santinello M, Vereecken CA. Soft drink consumption in adolescence: associations with food-related lifestyles and family rules in Belgium Flanders and the Veneto Region of Italy. Eur J Public Health. 2010;20:312–317. doi: 10.1093/eurpub/ckp150. [DOI] [PubMed] [Google Scholar]
- 18.Emmett PM, Heaton KW. Is extrinsic sugar a vehicle for dietary fat? Lancet. 1995;345:1537–1540. doi: 10.1016/s0140-6736(95)91087-5. [DOI] [PubMed] [Google Scholar]
- 19.Tinanoff N, Palmer CA. Dietary determinants of dental caries and dietary recommendations for preschool children. J Public Health Dent. 2000;60:197–206. doi: 10.1111/j.1752-7325.2000.tb03328.x. [DOI] [PubMed] [Google Scholar]
- 20.Amin TT, Al-Abad BM. Oral hygiene practices, dental knowledge, dietary habits and their relation to caries among male primary school children in Al Hassa, Saudi Arabia. Int J Dent Hyg. 2008;6:361–370. doi: 10.1111/j.1601-5037.2008.00310.x. [DOI] [PubMed] [Google Scholar]
- 21.Lim S, Sohn W, Burt BA, Sandretto AM, Kolker JL, Marshall TA, et al. Cariogenicity of soft drinks, milk and fruit juice in low-income african-american children: a longitudinal study. J Am Dent Assoc. 2008;139:959–697. doi: 10.14219/jada.archive.2008.0283. [DOI] [PubMed] [Google Scholar]
- 22.Burt BA, Pai S. Sugar consumption and caries risk: a systematic review. J Dent Educ. 2001;65:1017–1023. [PubMed] [Google Scholar]
- 23.Al-Malik MI, Holt RD, Bedi R. The relationship between erosion, caries and rampant caries and dietary habits in preschool children in Saudi Arabia. Int J Paediatr Dent. 2001;11:430–439. [PubMed] [Google Scholar]
- 24.Bolton-Smith C, Woodward M. Dietary composition and fat to sugar ratios in relation to obesity. Int J Obes. 1994;18:820–828. [PubMed] [Google Scholar]
- 25.Macdiarmid JI, Vail A, Cade JE, Blundell JE. The sugar-fat relationship revisited: differences in consumption between men and women of varying BMI. Int J Obes Relat Metab Disord. 1998;22:1053–1061. doi: 10.1038/sj.ijo.0800724. [DOI] [PubMed] [Google Scholar]
- 26.Ishdorj A, Crepinsek MK, Jensen HH. Children's Consumption of Fruits and Vegetables: Do School Environment and Policies Affect Choices at School and Away from School? Appl Econ Perspect Policy. 2013;35:341–359. [Google Scholar]
- 27.DeVet E, De Ridder DT, DeWit JB. Environmental correlates of physical activity and dietary behaviours among young people: a systematic review of reviews. Obes Rev. 2011;12:e130–e142. doi: 10.1111/j.1467-789X.2010.00784.x. [DOI] [PubMed] [Google Scholar]
- 28.McClain AD, Chappuis C, Nguyen-Rodriguez ST, Yaroch AL, Spruijt-Metz D. Psychosocial correlates of eating behavior in children and adolescents: a review. Int J Behav Nutr Phys Act. 2009;6:54. doi: 10.1186/1479-5868-6-54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Gebremariam MK, Henjum S, Terragni L, Torheim LE. Correlates of fruit, vegetable, soft drink, and snack intake among adolescents: the ESSENS study. Food Nutr Res. 2016;60:32512. doi: 10.3402/fnr.v60.32512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Sleddens EF, Kroeze W, Kohl LF, Bolten LM, Velema E, Kaspers PJ, et al. Determinants of dietary behavior among youth: an umbrella review. Int J Behav NutrPhys Act. 2015;12:7. doi: 10.1186/s12966-015-0164-x. [DOI] [PMC free article] [PubMed] [Google Scholar]