

Abstract
The aim of this trial was to examine the effects of antihypertensive fixed combination of lisinopril plus hydrochlorothiazide (Lopril H, Bosnalijek dd, Bosnia and Herzegovina) on regression of left ventricular hypertrophy in patients with essential arterial hypertension. We included 297 patients in our trial, aged 54,65±9,6 years, with treated or untreated hypertension and with high risk of cardiac events, in an opened trial of therapy based on lisinopril plus hydrochlorothiazide. Patients from five European countries were followed up for a period of 12 weeks. Duration of treatment was 12 weeks. We adjusted daily doses of lisinopril plus hydrochlorothiazide after every clinical examination and recorded adverse effects of drugs.
In the beginning and after 12 weeks of treatment, 277 patients (93,2%) underwent 2-dimensional echocardiography and there were 186 patients evaluated for efficacy of treatment on left ventricular hypertrophy (LVH). We recorded a regression of index mass LVH (168,56 vs 161,51 g/m2, P<0,0001), and regression was something more in women vs men.
We recorded average reduction of left ventricular mass index for patients with LVH (N=186) by 7,05 g/m2 (4,18%) in all patients, by 6,73 g/m2 (3,93%) in men and 7,27 g/m2 (4,37%) in women. The proportion of patients who attained a regression of left ventricular mass tended to be greater in men (54,55% vs 53,21%).
This research has proved regression of LVH in more than 53% patients after using fixed combination of lisinopril plus hydrochlorothiazide.
Keywords: essential hypertension, left ventricular hypertrophy, lisinopril, hydrochlorthiazide
INTRODUCTION
Left ventricular (LV) hypertrophy is a strong predictor of cardiovascular morbidity and mortality in the general population, and particularly in patients with hypertension. Regression of LV hypertrophy by antihypertensive therapy appears to reduce the risk for developing cardiovascular complications. Consequently, reversal of LVH is an important goal of antihypertensive therapy. Angiotensin converting enzyme (ACE) inhibitors reduce LV mass to a greater extent than other antihypertensive drug classes, when equivalent levels of blood pressure reduction are achieved. This provides strong evidence for the role of the renin-angiotensin-aldosterone system in the development or maintenance of LV hypertrophy.
The aim of this trial was to examine influence of fixed combination lisinopril plus hydrochlorothiazide (Lopril H, Bosnalijek dd, Bosnia and Herzegovina) on regression of left ventricular hypertrophy in patients with essential arterial hypertension.
PAINTS AND METHODS
The trial was open, multi-centre, prospective, clinical trial lasting 12 weeks per patient. Totally 277 subjects with essential hypertension were included in the trial, both genders aged 35 to 65 years. Total duration of the trial per patient was 12 weeks. The following examinations and measuring were performed prior to including into trial: Blood pressure and pulse
Electrocardiogram (Sokolow - Lyons; Cornell)
Echocardiography (of heart obligatory LVMI - left ventricle mass index)
Average age of all patients included into trial was 54,64±9,6 years, and 157 women and 140 men were included into trial. On the basis of initial results of echocardiography we found 186 patients with left ventricular hypertrophy. Average duration of illness for all patients was around 6,24±5,18 years.
In addition to high blood pressure, increased body weight (body mass index 25,0-29,9) was present in 39% women and 47,5% men, and obesity (body mass index above 30) was present in 41,5% women and 31% men, so that completely 19,5% women and 21,5% men had optimal body weight.
Statistical processing of results
Statistical analyses were made in statistical programme MedCalc for Windows, version 9.2.1.0 (MedCalc Software, Mariakerke, Belgium). Results are shown through the usual descriptive statistics and paired samples T-test.
As an estimate of significance of differences between the average measuring, significance was taken of P<0,05.
Methods
The study was done in compliance with Guidelines for Good Clinical Practice and Helsinki Declaration of the World Medical Association and all patients provided written informed consent before the beginning of the study. This 12-week opened prospective clinical trial was done at 12 centres in five European countries. After 2 weeks of washout period for patients receiving antihypertensive medications, patients entered the study. Patients were followed up for period of 12 weeks and duration of treatment was 12 weeks. We adjusted daily doses of lisinopril plus hydrochlorothiazide (Lopril H, Bosnalijek dd, Bosnia and Herzegovina) after every clinical examination and recorded adverse effects of drugs. LVH was documented by echocardiogram (Devereux criteria [LV mass index >134 g/m2 for men and>110 g/ m2 for women]) (1).
RESULTS
Total number of 297 patients (ITT) were included in the trial, 277 patients completely finalised the trial (by trial protocol, PP, 93,27%), and for 20 patients we did not make analyses of echocardiography (6,73%). Reasons for giving up the trial are not related to side-effects of drugs, nor intolerance to medicines, but they are linked to patients’ non-cooperation in the trial (e.g. irregular coming to control check-ups and irregular administration of therapy). We made analysis of blood pressure for all included patients (n=297) in the trial, and average lowering was accomplished for sys/dia BP 33,22mmHg/19,17mmHg, or by 20,56%/19,43%. Analysis of results has shown that we obtained the best results in medication’s effect on the systolic blood pressure, where lowering was accomplished in all the groups from 15,36% to 26,57%, while differences between baseline and final values of diastolic blood pressure by groups were from 15,66% to 22,28%. Treatment with fixed combinations of lisinopril plus hydrochlorthiazide in all patients resulted in mean change of LVH mass index 4,63±15,72 g/m2 (p < 0,0001) (Table 2; Figure 1). Treatment with fixed combinations of lisinopril plus hydrochlorthiazide in all patients with LVH resulted in mean change of LVH mass index 7,06±16,54 g/m2 (p<0,0001) (Table 3; Figure 2). Treatment with fixed combinations of lisinopril plus hydrochlorthiazide in men with LVH resulted in mean change of LVH mass index 6,77±16,49 g/m2 (p = 0,0006) (Table 4; Figure 3). Treatment with fixed combinations of lisinopril plus hydrochlorthiazide in women with LVH resulted in mean change of LVH mass index 7,28±16,64 g/m2 (p < 0,0001) (Table 5; Figure 4). We recorded average reduction of left ventricular mass index for patients with LVH (N=186) by 7,05 g/ m2 (4,18%) in all patients, by 6,73 g/m2 (3,93%) in men and 7,27 g/m2 (4,37%) in women. The proportion of patients who attained a regression of left ventricular mass tended to be greater in men (54,55% vs 53,21%). This research has proved regression of LVH in more than 53% patients after using fixed combination of lisinopril plus hydrochlorothiazide.
TABLE 1.
Baseline characteristics and risk factors of the patients
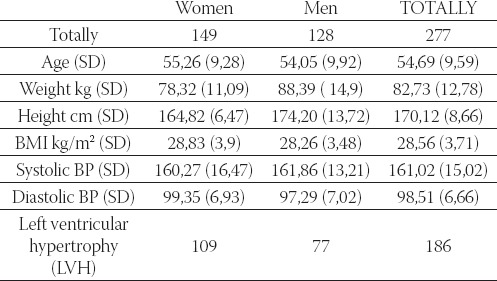
TABLE 2.
Echocardiography results of all patients included in trial (N=277) Legend: SD - standard deviation, *p<0,05.
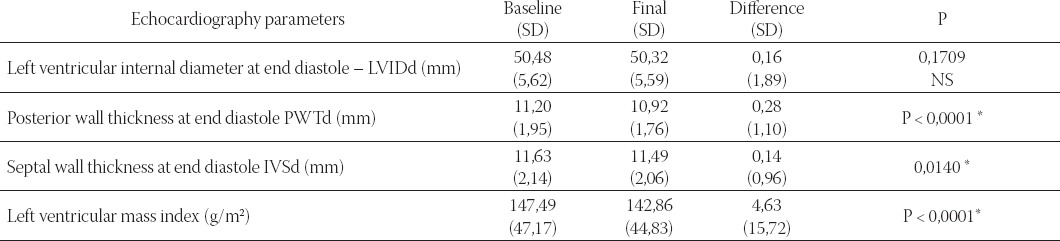
FIGURE 1.
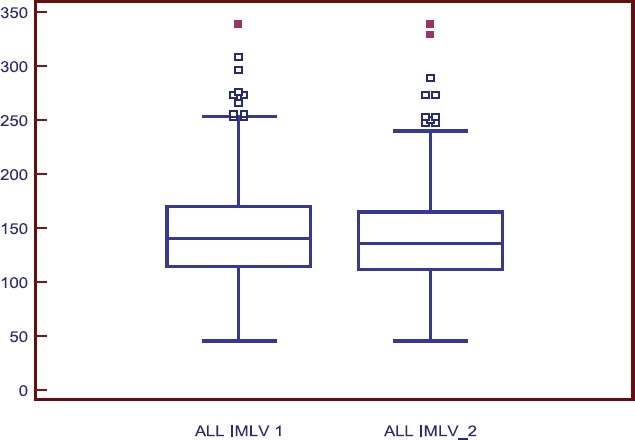
Changes in left ventricular mass index (g/m2) of all patients included in trial Legend ALL IMLV1 - left ventricular mass index of all patients, first measure; ALL IMLV 2 - left ventricular mass index of all patients, second measure
TABLE 3.
Echocardiography results of patients with LVH included in trial (n=186) Legend: SD - standard deviation, *P<0.05.
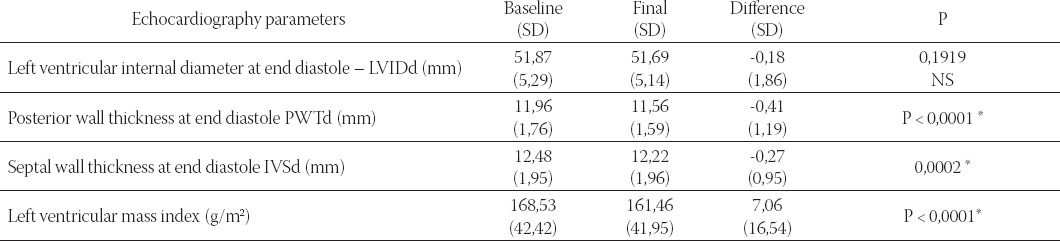
FIGURE 2.
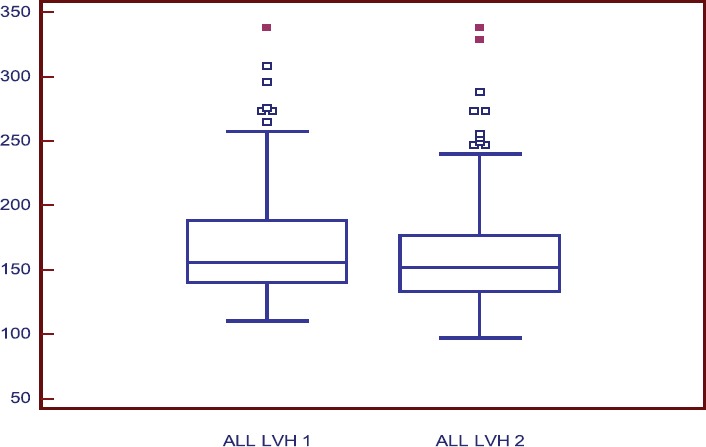
Changes in left ventricular mass index (g/m2) of patients with LVH Legend ALL LVH 1 - left ventricular mass index of all patients with LVH, first measure; ALL LVH 2 - left ventricular mass index of all patients with LVH, second measure
TABLE 4.
Echocardiography results of men with LVH included in trial (n=77) Legend: SD - standard deviation, *P<0,05.
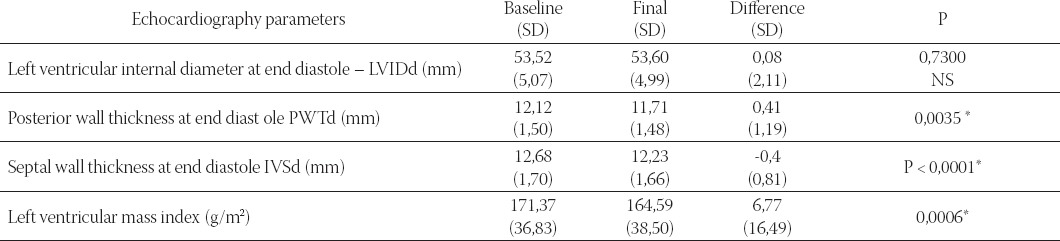
FIGURE 3.
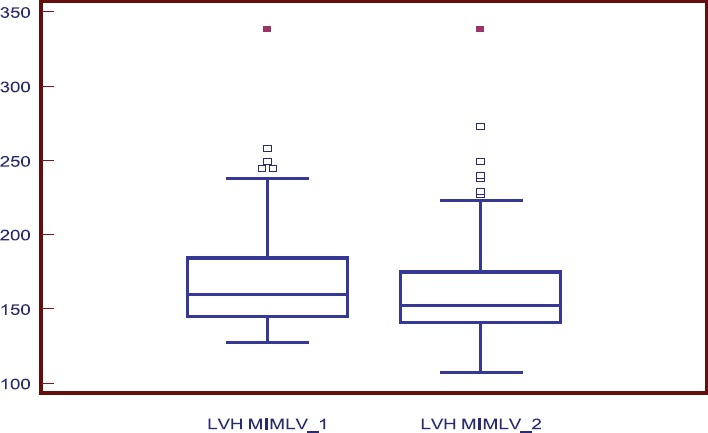
Changes in left ventricular mass index (g/m2) of men with LVH Legend LVH MIMLV1 - left ventricular mass index of men with LVH, first measure; LVH MIMLV 1 - left ventricular mass index of men with LVH, second measure
TABLE 5.
Echocardiography results of women with LVH included in trial (n=109) Legend: SD - standard deviation, *P<0,05.
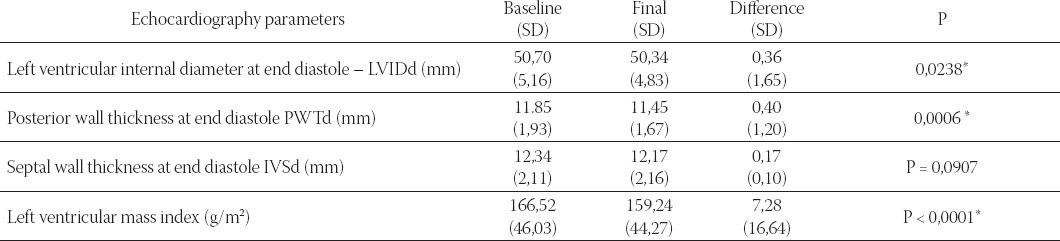
FIGURE 4.
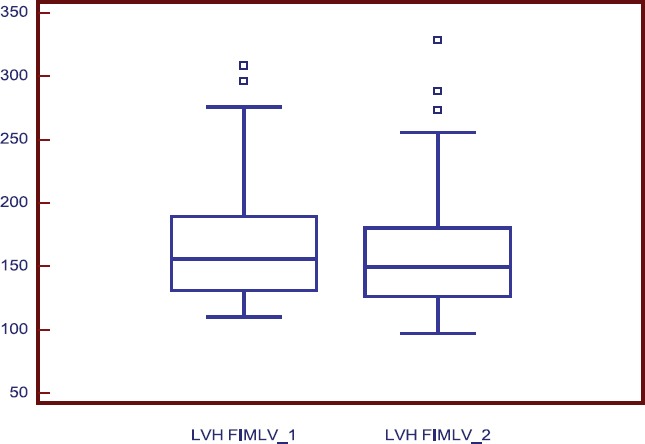
Changes in left ventricular mass index (g/m2) of women with LVH Legend: LVH FIMLV1 - left ventricular mass index of women with LVH, first measure; LVH FIMLV 1 - left ventricular mass index of men with LVH, second measure
DISCUSSION
LV hypertrophy is an important determinant of cardiovascular morbidity and mortality (2, 3), and reduction of LV hypertrophy with antihypertensive therapy reduces the number of cardiovascular events (4, 5). One of the most important prognostic factors in hypertension is electrocardiographic or echocardiographic left ventricular hypertrophy, with the latter already present in as many as 25% of patients with newly diagnosed hypertension. In a multicenter observational study of hypertensive patients with no prior history of cardiovascular or renal disease, echocardiographic left ventricular hypertrophy at baseline was accompanied by a three-fold increase in the cumulative 4-year incidence of cardiovascular events (6). Because of the firmly established prognostic significance of left ventricular hypertrophy, numerous studies have examined the ability of antihypertensive therapy to cause regression of left ventricular hypertrophy. Meta-analyses estimate that left ventricular mass can be reduced by 11 to 12% with an ACE inhibitor, ARB, or CCB; 8% with a thiazide diuretic; but only 5% with a β-blocker. In contrast, in patients undergoing valve replacement for aortic stenosis, nearly complete surgical normalization of systolic load results in a rapid and dramatic 35% reduction in left ventricular mass. The comparatively disappointing effects of the antihypertensive drug trials are likely to be related to the incomplete normalization of systolic load in monotherapy trials (6). Despite the impressive body of randomized clinical trial data, it remains to be determined whether even intensive antihypertensive therapy can completely normalize the excessive risks of cardiovascular and renal disease associated with untreated hypertension. In a large hypertensive referral clinic in Gothenburg, Sweden, treatment of hypertension in initially middle-aged men to a goal of 160/90 to 95 mm Hg with diuretics and β-blockers for 20 years did not completely normalize the risk of myocardial infarction. The persistently elevated risks in the treated patients were related to the existence of associated risk factors, such as cigarette smoking and elevated blood lipid levels, and emphasize the need for global risk reduction and larger reductions in blood pressure. Randomized trials have not yet established whether even lower blood pressure goals than those presently endorsed would produce further reductions in cardiovascular morbidity and mortality and in the risk of end-stage renal disease. Because of their relatively short duration (typically less than 5 years), randomized trials underestimate the life-time protection against premature disability and death afforded by several decades of antihypertensive therapy in clinical practice. In the Framingham Heart Study, treatment of hypertension for 20 years in middle-aged adults reduced total cardiovascular mortality by 60%, which is considerably greater than the results of most randomized trials despite the less intense treatment guidelines when therapy was initiated in the 1950s to 1970s (6). We used fixed combination of two antihypertensives lisinopril and hydrohlorthiazid (Lopril H, Bosnalijek dd, Bosnia and Herzegovina). The efficacy can be seen in the reduction of systolic and diastolic pressure, and this research has proved regression of LVH in more than 53% patients after using fixed combination of lisinopril plus hydrochlorothiazide.
CONCLUSION
This research has proved good efficacy and tolerability of fixed combination of lisinopril plus hydrochlorothiazide (Lopril H, Bosnalijek dd, Bosnia and Herzegovina) and in more than 53% patients recorded regression of left ventricular hypertrophy.
Separate
This trial is supported by pharmaceutical company Bosnalijek dd, Jukićeva 53, Sarajevo, Bosnia and Herzegovina.
REFERENCES
- 1.Devereux RB, Reichek N. Echocardiographic determination of left ventricular mass in man: anatomic validation of the method. Circulation. 1977;55:613–618. doi: 10.1161/01.cir.55.4.613. [DOI] [PubMed] [Google Scholar]
- 2.Casale PN, Devereux RB, Milner M, Zullo G, Harshfield GA, Pickering TG, et al. Value of echocardiographic measurement of left ventricular mass in predicting cardiovascular morbid events in hypertensive men. Ann. Intern. Med. 1986;105:173–178. doi: 10.7326/0003-4819-105-2-173. [DOI] [PubMed] [Google Scholar]
- 3.Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP. Prognostic implications of echocardiographically determined left ventricular mass in the Framingham Heart Study. N. Engl. J. Med. 1990;322:1561–1566. doi: 10.1056/NEJM199005313222203. [DOI] [PubMed] [Google Scholar]
- 4.Muiesan ML, Salvetti M, Rizzoni D, Castellano M, Donato F, Agabiti Rosei E. Association of change in left ventricular mass with prognosis during long-term antihypertensive treatment. J. Hypertens. 1995;13:1091–1095. doi: 10.1097/00004872-199510000-00003. [DOI] [PubMed] [Google Scholar]
- 5.Verdecchia P, Schillaci G, Borgioni C, Ciucci A, Gattobigio R, Zampi I, et al. Prognostic significance of serial changes in left ventricular mass in essential hypertension. Circulation. 1998;97:48–54. doi: 10.1161/01.cir.97.1.48. [DOI] [PubMed] [Google Scholar]
- 6.Ronald GV. Arterial Hypertension. Cecil medicine. In: Goldman L, Ausiello DA, editors; Lee Goldman, Dennis Ausiello., editors. enhanced online features and print) 23rd ed. Elsevier Science Pub; 2007. pp. 430–450. [Google Scholar]