

Abstract
Bronchopleural fistula (BPF) with prolonged air leak (PAL) is most often, though not always, a sequela of lung resection. When this complication occurs post-operatively, it is associated with substantial morbidity and mortality. Surgical closure of the defect is considered the definitive approach to controlling the source of the leak, but many patients with this condition are suboptimal operative candidates. Therefore there has been active interest for decades in the development of effective endoscopic management options. Successful use of numerous bronchoscopic techniques has been reported in the literature largely in the form of retrospective series and, at best, small prospective trials. In general, these modalities fall into one of two broad categories: implantation of a device or administration of a chemical agent. Closure rates are high in published reports, but the studies are limited by their small size and multiple sources of bias. The endoscopic procedure currently undergoing the most systematic investigation is the placement of endobronchial valves. The aim of this review is to present a concise discussion on the subject of PAL and summarize the described bronchoscopic approaches to its management.
Keywords: Air leak, pneumothorax, bronchopleural fistula (BPF), bronchial valves, bronchoscopy
Introduction
Prolonged air leak (PAL) is a dreaded post-operative complication of thoracic surgery and a major clinical problem in patients with pneumothorax of a medical etiology. Although surgical management is considered the definitive approach, bronchoscopic techniques have been part of the toolkit for decades because many of these patients are suboptimal surgical candidates. These endoscopic interventions have evolved from crude occlusion devices and primitive glues to sophisticated valves and resorbable hemostatic sealants. The tools most widely used in current practice can all be applied using flexible bronchoscopy. Procedural success is typically defined as cessation (or at least reduction) of air leak. Whether the chemical or device route is chosen, published experience indicates that repeat procedures are common owing to incomplete initial response. It should be recognized that the body of evidence supporting bronchoscopic treatment of PAL is limited to, at best, small prospective studies and is subject to numerous forms of bias. When the largest series reporting results of endoscopic interventions for post-pneumonectomy PAL were systematically reviewed in 2007, an overall cure rate of only 30% was obtained (1). An additional cautionary note is that a systematic review of randomized controlled trials on intra-operative sealant application for prevention of air leak after lung cancer resectional surgery found that only a small minority of these trials showed benefit and therefore firm recommendations were withheld (2). This article begins with an overview of important definitions and clinical considerations pertaining to PAL followed by a discussion of the individual bronchoscopic modalities.
Definitions
Air leak into the pleural space originating either from an airway or lung parenchyma is one of the most common complications of thoracic procedures ranging from transbronchial biopsy to pneumonectomy, in which case the resultant pneumothorax is iatrogenic (3,4). Air leak can also give rise to primary spontaneous pneumothorax in patients with no grossly evident lung pathology as well as secondary spontaneous pneumothorax (SSP) in those with underlying pulmonary disease (e.g., emphysema, cystic fibrosis, infection, etc.). Another etiology of air leak is chest trauma. When the source of air entering the pleural space is at the level of a segmental bronchus or more proximal, the lesion is termed a bronchopleural fistula (BPF); a more distal origin implies the presence of an alveolopleural fistula (APF) (5). The preponderance of the literature on the subject of air leak is of a surgical nature and therefore post-operative BPF dominates the discourse, as it will in the present review.
The presence of an air leak is indicated by the detection of bubbles in the water seal chamber of the collection system connected to the pleural drain. This is a common phenomenon during the first 2 days after pulmonary resection but persists beyond that only in a small minority of patients (6). The severity of air leak is typically classified according to the phase of the respiratory cycle during which the bubbles appear, and it increases along the following continuum: escape of air during forced exhalation maneuver only (i.e., cough), during quiet exhalation only (spontaneous breathing), during inspiration only (positive pressure breathing), and during both inhalation and exhalation (7). Drainage systems equipped with digital flow meters capable of quantifying the leak are now also available (8). Conventionally, an air leak is considered prolonged if it persists beyond 5 days after the precipitating event. It is the BPF complicated by PAL that poses the most serious threat to the patient and the greatest clinical challenge. Bronchoscopic interventions to be discussed herein are best viewed in the context of this extreme of the disease spectrum.
Epidemiology and clinical features
The most common cause of BPF is resectional thoracic surgery, especially pneumonectomy (right more than left) (9) and lung volume reduction surgery (LVRS) (10). The reported incidence of post-resection BPF varies from as low as 2% (11) to as high as 90% (10) depending on multiple variables such as type of operation and surgical technique. Residual cancer at the resection margin (12) and post-operative positive pressure ventilation (13) has also been shown to increase the risk. Several patient factors predisposing to the development of post-operative BPF have been identified; notable among them are low forced expiratory volume in 1 second (FEV1) (14), emphysema (15), diabetes (16), chronic systemic steroid use (17), and neoadjuvant chemotherapy and/or radiation (18). In the immediate post-operative period, BPF implies stump dehiscence and can present as an acute decompensation related to the possibility of empyema, aspiration of pleural space contents into one or both lungs, wasted ventilation, and tension pneumothorax (19). Delayed (>30 days) post-surgical BPF is a more indolent illness characterized by fever and constitutional symptoms reflective of chronic reciprocal soilage of the pleural and alveolar spaces. Besides its morbidity and attendant resource utilization, post-resectional BPF is associated with a significant crude in-hospital mortality rate, reported to be in excess of 70% in one study (12). The basic tenets of the care of the BPF patient are to ensure adequate ventilatory support, initiate drainage of empyema if present, administer appropriate antibiotics, and optimize nutritional status. The definitive means of addressing a post-surgical BPF is operative closure. Historically, bronchoscopic management of BPF has been reserved for patients deemed to be poor candidates for re-operation.
Localization
Pinpointing the site of post-resectional BPF is generally straightforward as it is almost always located at the bronchial stump. Localization of non-operative BPF and APF can be more challenging. Chest computed tomography is capable of identifying the location of a peripheral fistula by demonstrating a communication between a bronchus and the pleural space (20) (Figure 1). The detection of bronchoscopically instilled methylene blue in the pleural collection chamber would indicate the presence of a fistula but would not establish its location. Retrograde administration (i.e., from the pleural side), on the other hand, can identify the culprit airway based on where the dye is encountered at subsequent bronchoscopy (21). The use of ventilation scintigraphy has also been described, which is predicated on abnormal focal accumulation of the inhaled tracer at the site of communication with the pleural space (Figure 2). Both radioisotope-labeled gas (e.g., 133Xe and 81mKr) and aerosol have been employed for this purpose (22). Inhalation of the latter, in the form of 99mTc-tagged diethylenetriamine pentaacetate (DTPA), was performed to detect air leaks of various etiologies in a study of 28 patients, which it did with an overall sensitivity of 78% and a specificity of 100% (23). Fusion of scintigraphy with concomitant single photon emission computed tomography (SPECT) could enable more precise localization.
Figure 1.
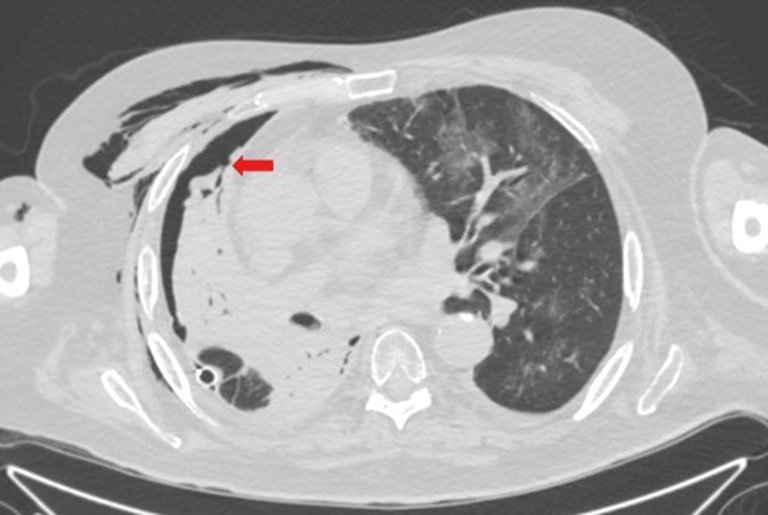
CT chest showing a communication between a peripheral branch of the right middle lobe medial segment bronchus and the pleural space (arrow) in a patient with a BPF due to erosive lung cancer.
Figure 2.
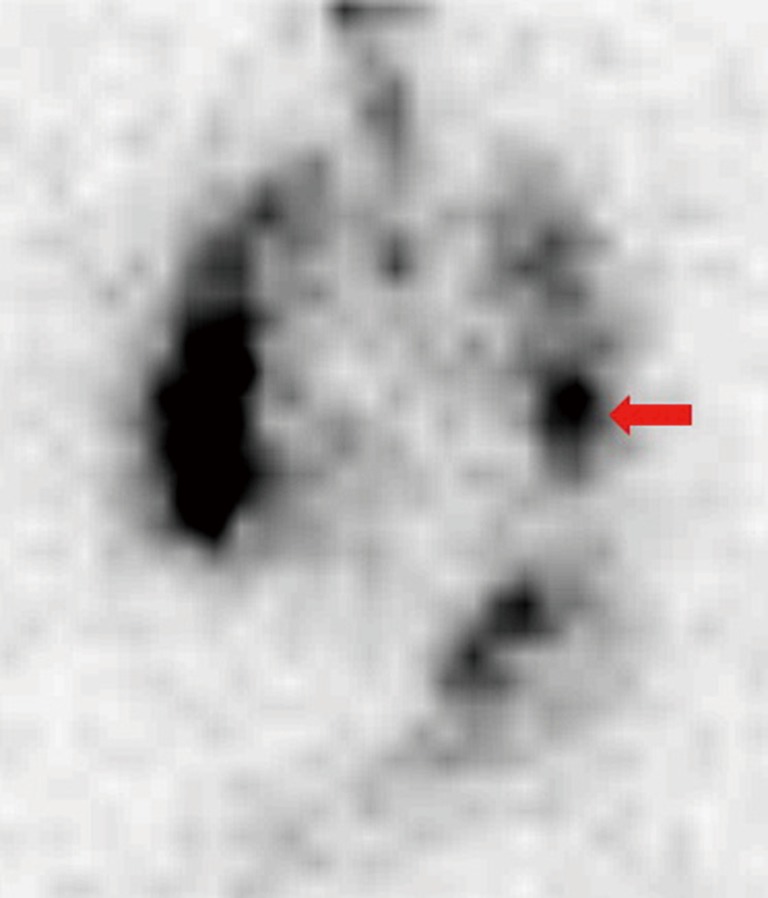
99mTc-DTPA ventilation scintigraphy image showing focal radiotracer accumulation in the lower left hemithorax (arrow) corresponding to the site of PAL in a patient with left secondary spontaneous pneumothorax in the setting of idiopathic pulmonary fibrosis.
For the purpose of bronchoscopic intervention, real-time confirmation of the airway feeding the air leak is of fundamental importance. Currently, the balloon occlusion method described by Ratliff and colleagues in 1977 is the most widely used approach (24). This technique involves passing a Fogarty® balloon catheter (Edward Lifesciences Corp., Irvine, CA, USA) through the instrument channel of a flexible bronchoscope, which is then sequentially inflated in the lobar bronchi. The cessation or significant diminution of air leak following balloon occlusion of a given lobar bronchus, which could take up to 2 minutes to manifest, identifies it as leading to the fistula. The balloon is then similarly inflated in the segmental bronchi and, if feasible, the sub-segmental bronchi within the target lobe to localize the culprit airway at those generations. Frequently, more than one candidate bronchus will be identified. In the case of endobronchial valve placement (see below), this balloon occlusion test can be performed with an included kit that allows for simultaneous sizing of the airway for valve selection. Another option is the commercially available Chartis® system (Pulmonx, Redwood City, CA, USA) designed to assess for the presence of collateral ventilation (25). This system provides a balloon catheter that is equipped with a flow and pressure sensor. A persistently negative pressure after inflation and elimination of air flow in an airway indicates communication with a BPF.
Valves
Endobronchial valves (EBV) are currently the most actively explored bronchoscopic modality for the management of PAL. They were originally developed and studied as a minimally invasive alternative to LVRS. EBVs are designed to function as removable one-way barriers that permit air and secretions to escape during exhalation but prevent air from passing through during inhalation. When applied to PAL, the hypothesis is that abolition by the EBV of airflow through the airway leading to the fistula will allow the defect to seal. Placement is envisioned to be temporary with removal after a period of tissue healing. Fann and colleagues inserted EBVs into the corresponding segmental bronchus of each of six sheep following creation of an air leak due to APF for which they first placed a pleural drain (26). They were able to achieve rapid resolution of the air leak in all animals. The first reported use of EBVs in humans to control air leak was published by Snell and colleagues in 2005 after successful treatment of a patient with intractable pleuro-cutaneous fistula (27).
Two types of EBVs are currently produced in the United States (US): the Emphasys Zephyr® Endobronchial Valve System (Pulmonx, Redwood City, CA, USA) and the Spiration® Valve System (Olympus Respiratory, Redmond, WA, USA). Both are constructed on a Nitinol (nickel-titanium) frame. The body of the Spiration® EBV is umbrella-shaped and made of polyurethane (Figure 3), whereas the Zephyr® EBV has a “duck bill” configuration and is made of silicone (Figure 4). The Spiration® EBV system comes in three different sizes corresponding to airway diameters of 5, 6, and 7 mm. The Zephyr® EBV system is manufactured in size 4.0 and 5.5 for use in airways measuring 4–7 mm and 5.5–8.5 mm, respectively. After the target airway is sized by means of the included balloon kit, the corresponding EBV is deployed via a flexible bronchoscope using the provided delivery catheter (Figure 5). When appropriate, valve removal is accomplished by grasping it with forceps passed through the instrument channel and then pulling out the bronchoscope and forceps together with the valve as one unit. As of this writing, only the Spiration® product is approved by the US Food and Drug Administration (FDA) and available exclusively under the Humanitarian Device Exemption Program for post-operative PAL complicating lung resectional surgery.
Figure 3.
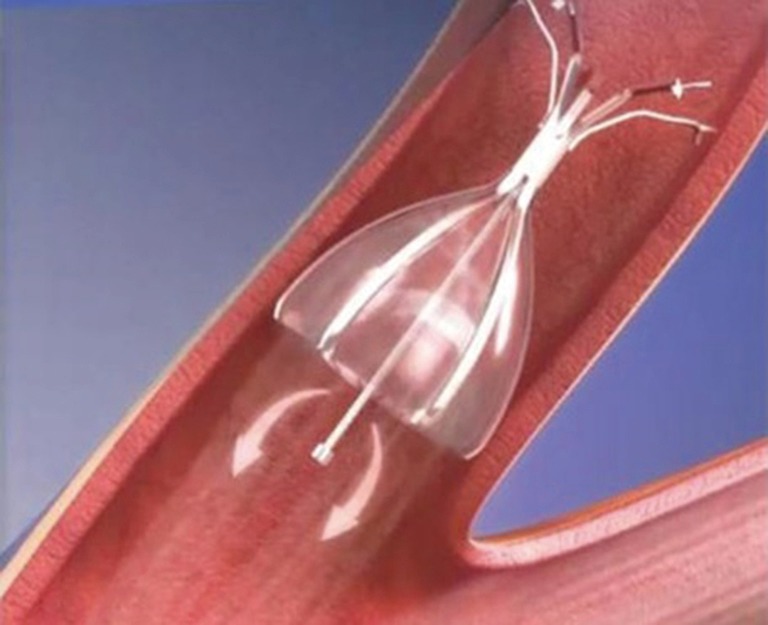
Diagram of the Spiration® endobronchial valve. Image courtesy of Olympus Respiratory.
Figure 4.

Depiction of the Zephyr® endobronchial valve. Image courtesy of Pulmonx, Inc.
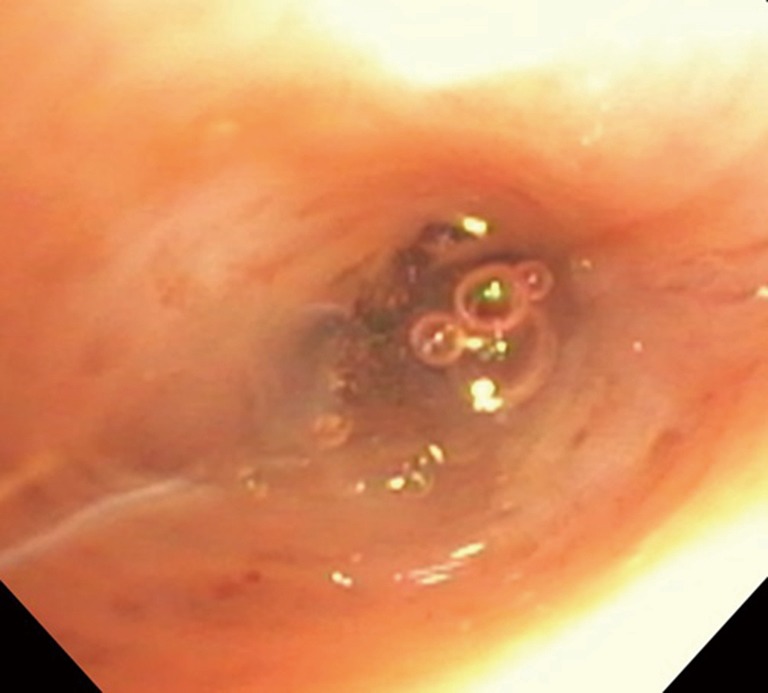
Figure 5.
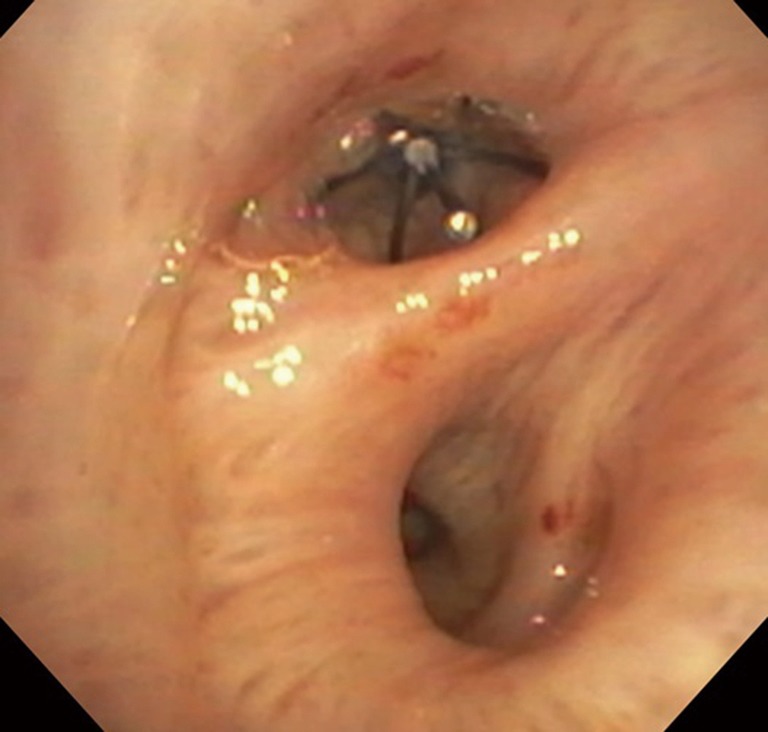
Appearance of the Spiration® endobronchial valve in the proximal right middle lobe bronchus as viewed from the bronchus intermedius. Image courtesy of Dr. Kassem Harris.
In contrast to the other bronchoscopic interventions covered in this review, the literature regarding EBV placement for PAL includes not only a number of robust retrospective series but also prospective observational data (Table 1). The earliest series dates to 2009 and reports the results of 40 cases of predominantly non-surgical PAL managed with Zephyr® EBV insertion (28). The air leak was abolished or reduced in 37/40 patients (92.5%), allowing pleural drain discontinuation after a median of 7.5 days. A maximum of 9 valves was placed in any given patient. In 8 of the 40 patients (20%), the valves were subsequently removed without recurrence. Six patients (15%) developed complications, among them valve expectoration and malpositioning as well as pneumonia. Subsequent smaller case series (29,33) reported similarly high control rates with Spiration® EBV in a population of mixed surgical and medical PALs, some of which were refractory to prior operative interventions. A median of approximately three valves per patient were implanted, allowing pleural drain removal after about 2 weeks in cured cases. No procedural adverse events were reported, and all attempted valve extractions were successful. Dooms and colleagues prospectively studied 10 patients with post-resectional PAL, 9 of whom underwent treatment with a median of 4 Spiration® EBV (31). Six of the 9 experienced durable total or near total cessation of air leak while the other 3 had recurrence, albeit at a lower flow rate, attributable to valve displacement. Median time to chest drain removal was 4 days, including the 3 non-responders who were discharged with Heimlich valves and ultimately had their drains discontinued at 14 days post-procedure. All patients underwent uneventful valve removal and no complications occurred that were attributable to the valves. In an analogous prospective study, Firlinger and colleagues used both EBV systems and were able to successfully remove the pleural drains of 10 out of 13 patients (77%) with PAL of mostly malignant and infectious etiology (30). Most recently, Gilbert and colleagues compiled the experience of multiple EBV centers consisting of 75 patients (out of a total of 112 evaluated for the procedure) who received a median of 2.6 valves (32). The rate of air leak resolution varied depending on cause of PAL: 100% in those with iatrogenic injury versus 58% in the presence of underlying lung disease (i.e., SSP). Overall median time to cessation of air leak was 4 days, but that number was over 2 weeks in successful cases of SSP. Two patients (3%) experienced complications deemed related to the valves, namely empyema and contralateral pneumothorax.
Table 1. Summary of the major studies of EBV insertion for PAL.
| Lead author, year | Study design | Number of patients receiving EBVa | Valve type | Valves/patient (mean ± SD or median) | Procedural success rate (%)b | Time to pleural drain removalc (mean ± SD or median days) | Valve retrieval rate (% of subjects) | Procedural complication rate (%) |
|---|---|---|---|---|---|---|---|---|
| Travaline 2009 (28) | Retrospective | 40 | Zephyr® | 2.9±1.9 | 93 | 7.5 | 20 | 15 |
| Gillespie 2011 (29) | Retrospective | 7 | Spiration® | 3.5 | 75 | 16 | 71 | 0 |
| Firlinger 2013 (30) | Prospective | 13/19 | Both | 1.4±0.7 | 77 | 7.6±5 | 83 | 0 |
| Dooms 2014 (31) | Prospective | 9/10 | Spiration® | 4 | 67 | 4 | 100 | 0 |
| Gilbert 2016 (32) | Retrospective | 75/112 | Spiration® | 2 | 56d | 4 | NR | 3 |
NR, not reported. a, total number of patients evaluated for EBV placement provided after slash where applicable; b, procedural success is generally defined as rapid resolution and/or diminution of air leak following the intervention; c, time following EBV implantation; d, data not available for all patients.
Spigots
Bronchial occlusion with silicone for the treatment of BPF was first reported over two decades ago (34). Subsequently, Watanabe and colleagues developed endobronchial Watanabe spigots (EWS®, Novatech, Grasse, France) made of silicone that they used to treat 60 patients with air leak of various etiologies, in 58 of whom (97%) they were able to achieve satisfactory positioning of the device. Elimination or reduction of air leak was achieved in nearly 80% of cases (35). These spigots are coated with barium sulfate for radiographic visibility; they have tapered ends and come in three sizes (Figure 6). They are grasped with forceps introduced through the working channel of the bronchoscope and then advanced within the bronchus until firmly wedged. The process is repeated if additional bronchi need to be occluded. The spigots are later removed when clinically feasible. Since the original publication by Watanabe, several case series have documented the successful use of EWS® in BPF management. The largest, by Kaneda and colleagues, reported 21 patients who had undergone endobronchial occlusion with a spigot (36). Complete resolution of air leak after the initial procedure was observed in 6/21 (29%) of patients while 12/21 (57%) had reduction in air leak. The latter group required additional spigots and/or pleurodesis to achieve complete cessation of air leak. Recently, based on work with a canine lung model, a new technique has been proposed for the placement of EWS® wherein a rotatable biopsy forceps (FB-19CR-1, Olympus USA, Central Valley, PA, USA) is used to grasp the spigot, which makes it more maneuverable and easier to position (37). In Japan, the spigots are an established and officially recognized device for the management of intractable pneumothorax. They are not listed as FDA-approved in the United States.
Figure 6.

Three sizes of endobronchial Watanabe spigots (EWS®). Image courtesy of Novatech.
Chemical and thermal occlusion
Tissue adhesives
Cyanoacrylate compounds (e.g., n-butyl-2-cyanoacrylate marketed as Histoacryl®, Tissue Seal, Ann Arbor, MI, USA) are best known for their use in minor laceration repair and surgical skin closure. In the 1980s, investigators instilled this substance via a flexible bronchoscope into a canine model of post-pneumonectomy BPF at the stump (38). When the four study dogs were sacrificed and their tracheas excised, the stumps were found to be sealed and covered by a layer of scar tissue. An early series from Norway describes successful closure of BPF with this compound following pneumonectomy for lung cancer in two patients (39). More recently, a group from Taiwan reported its use for a post-lung transplant BPF (40). In all three cases administration was through a flexible bronchoscope. Scappaticci et al. published their experience after accumulating 20 cases of BPF treated with instillation of cyanoacrylate (41). Almost all were complications of lung resection for carcinoma (18/20), and the majority (13/20) were small (<5 mm). Overall, successful closure was achieved in 14/20 patients (70%), predominantly when performed for small BPF (12/13). Chawla et al. applied this compound through a flexible bronchoscope using a transbronchial needle aspiration catheter for its delivery (42). They treated 9 patients, 4 of whom had non-surgical BPF. In those four cases, balloon occlusion was employed to localize the origin of the BPF. Durable closure occurred in 8 of the 9 patients with the only failure being a post-pneumonectomy BPF >8 mm in size. The pleural drain was removed a maximum of 4 days following successful procedures except for a case of tuberculous hydropneumothorax in which the drain remained in place for 14 days. Those with experience in endoscopic application of cyanoacrylates recommend withdrawing the delivery catheter immediately upon instillation to avoid gluing it to the airway tissue (43). They likewise caution about keeping the bronchoscope sufficiently far (i.e., at least 4 cm) from the catheter tip during administration to avoid inadvertent gluing of the instrument channel, which would require urgent rinsing of the channel with a solvent such as acetone to restore its patency (42).
Another substance in this category that has been described for BPF management is the adhesive formed by the combination of bovine serum albumin and glutaraldehyde (BioGlue®, CryoLife, Kennesaw, GA, USA). Two case series (44,45) include a total of four patients who underwent instillation through either a flexible or rigid bronchoscope, all achieving successful closure lasting as long as 5 months post-procedure.
Hemostatic agents as sealants
The most documented agent for the bronchoscopic treatment of BPF is fibrin glue (Tisseel®, Baxter, Deerfield, IL, USA), which is indicated for surgical hemostasis and bonding. Its effect is based on biological thrombogenesis that occurs when the two components—fibrinogen and thrombin—mix at the time of delivery. The fibrin plug thus created is ultimately degraded by endogenous plasmin, a process that is delayed for as long as 14 days by the incorporation of a plasmin inhibitor called aprotinin into the product (46). It is hoped that in the interim tissue approximation will have taken place by secondary intention. In a canine experiment conducted in the 1980s, direct application of fibrin glue to an artificially created APF significantly decreased the magnitude of air leak compared to no intervention (47). Multiple case reports (46,48) and series (49-51) describe the application of fibrin glue in various amounts (typically 2–5 mL) through both rigid and flexible bronchoscopes for the treatment of post-operative BPF. Of special interest is a review of 45 cases of post-surgical BPF by Hollaus and colleagues, 29 of which were managed with the introduction of fibrin glue via rigid bronchoscopy (52). Their sample represents one of the largest publications to date on the role of endoscopic BPF closure. This approach was restricted to BPF smaller than 8 mm with no associated empyema, and the fibrin plug was reinforced with spongy calf bone if the defect was greater than 3 mm in size. Towards the end of the study period, the procedure changed from endoluminal instillation to submucosal injection of the glue. Of the 29 patients treated endoscopically, 9 (31%) were cured and survived to discharge free of pleural drains. Seven had successful BPF closure (i.e., cessation of the air leak) but still required permanent pleural drainage for chronic empyema. Another 7 experienced failure of the closure attempt. The remaining 6 patients died in hospital. The rate of initial successful endoscopic BPF closure in this sample was therefore at least 16/29 or 55% depending on the response of the air leaks of those who did not survive to discharge (not reported). The authors note that eventual BPF recurrence was observed in 2 of the 16 cases discharged without an air leak (12%).
Coseal® (Baxter, Deerfield, IL, USA) is a polyethylene glycol-based hydrogel that closes tissue defects by crosslinking with native proteins. It is designed for leak repairs during reconstructive vascular surgery and is fully resorbed (Figure 7). Mehta and colleagues administered this product to 22 patients with PALs, most of them non-surgical, through the working channel of a flexible bronchoscope using a flexible catheter (53). Cessation of air leak was achieved in 19 patients (86%) an average of 2 days after completing treatment, and the average time to pleural drain removal was about 4 days. Three patients expectorated the plug without complications, whereas one required an emergent bronchoscopy to suction the plug from the trachea after developing hypoxemia.
Figure 7.
Appearance of Coseal® upon instillation into a lobar bronchus as it begins to congeal into a plug. Image courtesy of Dr. Kassem Harris.
A number of physical hemostatic materials have also been deployed through the flexible bronchoscope in individual cases to successfully obliterate BPF. One example is the insertion of strips cut from an absorbable sponge made from purified porcine skin gelatin (Gelfoam®, Pfizer, New York, NY, USA). Placement into two left upper lobe segmental bronchi was accomplished by feeding the moistened strips into the instrument channel with the aid of forceps and then flushing them out with saline once the bronchoscope was positioned in the desired location (54). In another report, organized regenerated cellulose (Surgicel®, Ethicon, Somerville, NJ, USA) was inserted in a similar fashion into the left mainstem bronchus of a mechanically ventilated patient whose BPF at that location was caused by an eroding mass (55). To prevent dislodgment of the Surgicel® patch by positive pressure ventilation, a Fogarty catheter was left in place with the balloon inflated at the closure site to keep the seal intact. Two days following the procedure, the patient was breathing spontaneously and had no air leak even with the balloon deflated. The catheter and pleural drains were removed, and the patient was discharged 6 days after the procedure.
Submucosal injections
In addition to the submucosal injection of fibrin glue as performed by Hollaus et al. (see above), the other substances that have been introduced through the flexible bronchoscope into the submucosa at the site of a BPF fit one of two categories: tissue expanders and sclerosing agents. Experience with the former is limited to a description of two cases in which a suspension of carbon-coated zirconium beads in a water-based gel matrix (Durasphere®, Carbon Medical Technologies, St. Paul, MN, USA) was injected submucosally using a transbronchial aspiration needle (56). In one of the two cases, subsequent cyanoacrylate instillation was required to abolish a residual air leak. Over time, Durasphere® is expected to promote collagen formation that would add to its tissue bulking effect. This substance is biocompatible but not biodegradable. The injection of sclerosing agents such as tetracycline (57), silver nitrate with (58) or without (59-61) an albumin suspension, pure ethanol (62), and ethanolamine (63) appears to initially produce BPF closure by causing local tissue edema, which is followed by an inflammatory reaction and then by granulation tissue that serves as the ultimate seal. Of these chemicals, silver nitrate delivered through a flexible bronchoscope is the best-described technique and has been >80% effective in recent series (61).
Varoli and colleagues have published their results of managing 35 post-resectional BPF with injections of polidocanol (Aethoxysklerol®, Kreussler, Wiesbaden, Germany), a pharmaceutical designed for sclerotherapy to treat spider and varicose veins (64). Successful closure was achieved in 23/35 cases (66%), including post-pneumonectomy BPF as large as 10 mm. Bronchoscopically injected ethanolamine, a related compound, achieved cessation of air leak in 12/15 (80%) predominantly medical patients.
Thermal therapy
Perhaps counterintuitively, the use of ablative energy delivered through the flexible bronchoscope for the management of BPF has also been described. The premise is to induce tissue inflammation that will heal by forming scar tissue that pulls the defect closed. While the use of argon plasma coagulation is limited to a single case report (65), Kiriyama and colleagues have published their experience with Nd:YAG laser (power 5–20 W in 0.5-second pulses) in 8 patients with post-surgical BPF, reporting successful and durable closure in 4 of them (66).
Miscellaneous
Metallic non-valvular devices
In this category, the most commonly employed item is vascular embolization coils, described in case reports and small series. Their insertion has been accompanied by the concomitant instillation of either cyanoacrylate (67,68) or fibrin glue (69,70). One of the most curious approaches to endoscopic BPF management described in the literature is the deployment of a lead split shot, otherwise known as a fishing weight, using a flexible bronchoscope (24). The scenario in which this technique was pioneered was that of a patient with acute respiratory distress syndrome complicated by barotrauma from positive pressure ventilation. The plug was threaded onto a guidewire positioned in the subsegmental bronchus identified as the culprit airway beforehand. It was then pushed forward by the tip of the bronchoscope following it along the guidewire until it was wedged in place. After this 1977 report, there have been no additional published articles documenting the placement of lead shots for BPF.
Septal defect closure devices
Amplatzer™ occluders (AO) are well-known in the field of cardiology for their use in septal defect closure, an application from which they have been adapted for management of BPF. They are made of Nitinol mesh with a polyester fabric, a combination that provides initial coverage and then promotes tissue growth over the device. There are two types of such devices that have been used for BPF: the AMPLATZER® Septal Occluder and the AMPLATZER® Duct Occluder II (St. Jude Medical, St. Paul, MN, USA). Both have a slim central waist with a disc on each end (Figure 8). The appropriate size for a given BPF depends on the dimensions of the stump and length of the fistula to be treated. For placement, a guidewire is passed via the instrument channel of a flexible bronchoscope and through the BPF followed by a sheath. Next, the AO and its distal disc are advanced past the fistula and positioned by pulling back so that the disc sits flush against the opening. The second disc is then delivered to the proximal side of the defect. In the largest series, Fruchter and colleagues were able to successfully close 9 of 11 (82%) mostly post-surgical BPF in mainstem and lobar bronchi with AOs without complications (71). The feasibility of this approach has since been corroborated by others (72). AMPLATZER® vascular plugs (St. Jude Medical, St. Paul, MN, USA), an analogous device functionally related to embolization coils, have also been applied to BPF treatment by the same group (73). These are likewise Nitinol-based, and the deployment principle is similar to that of AOs.
Figure 8.

An example of an Amplatzer occluder: AMPLATZER® Duct Occluder II. Image courtesy of St. Jude Medical.
Stents
Stents are the mainstay of bronchoscopic relief of central airway obstruction. They have also been used for the management of BPF as described in several case reports and series. Metallic stents are known to incite an inflammatory response that generates granulation tissue. When airway patency is the goal, this would be considered an untoward effect of stent placement, but when defect closure is desired, such overgrowth can be advantageous. In some instances, the shape of a stent has been modified to make it better suited for coverage of a particular fistula. The largest series by Cao and colleagues describes the use of a fully covered metallic stent (SigmaMed Industrial Co., Ltd., Huaian, China; CZES type) in 9 patients with fistulae, 7 of which were bronchopleural (74). Resolution of air leak was achieved in all 7, and only one patient required a repeat procedure for a complication, namely stent expectoration. In another review of 7 patients with large post-pneumonectomy BPF, Dutau and colleagues deployed custom-made fully covered, self-expandable metallic stents (SILMET® conical stent, Novatech, La Ciotat, France) via rigid bronchoscopy to treat the fistulae with an immediate success rate of 100% (75). Pre-procedure measurements of the area to be covered by the stent were taken so that the midpoint of the customized stent would coincide with the defect. The authors intentionally oversized the stents by 2mm in diameter to allow maximal apposition. Chae and colleagues used a custom-designed metallic, fully covered stent with its distal third constricted—giving it a “wine glass” appearance—in order to allow the thin stem to fit in the BPF tract (76). The distal end of stent (the base of the “wine glass”) was positioned on the outside of the stump in the post-pneumonectomy space while the proximal end (the bowl of the “wine glass”) occupied the intact portion of the mainstem bronchus. Bronchoscopic inspection 2 months after the procedure revealed complete closure of the BPF. An important drawback of customized stenting is the time required to obtain these devices, as this prolongs hospitalization and delays therapeutic intervention.
Silicone stents have also been placed using rigid bronchoscopy for the management of large post-pneumonectomy BPF. For instance, a customized Y-shaped silicone stent successfully occluded a left mainstem bronchus stump dehiscence after trimming the corresponding bronchial limb, pushing a cuff link-shaped prosthesis (DJ-FistulaTM, Bryan Corp., Woburn, MA) into the stent’s distal lumen, and suturing it with silk (77). Additionally, the stent was reinforced with Surgicel® and fibrin glue to prevent any residual leaks. Ferraroli and colleagues were also able to place a modified Dumon® Y stent (Tracheobronxane Y; Novatech SA, La Ciotat Cede, France) in a patient with a 2 mm right mainstem bronchus stump fistula. The stent’s right limb was occluded with silicone material taken from the same stent (78).
Blood patch
The instillation of autologous blood (blood patch) through a pleural drain for the successful management of PAL has been reported in case series (79). This approach relies both on the immediate sealing effect of clotted blood and on the resultant pleural inflammation and symphysis. Endoscopic, catheter-guided delivery of autologous blood has also been described. Wiaterek and colleagues reported a patient with necrotizing pneumonia complicated by pneumothorax and PAL. Using flexible bronchoscopy and forceps, several layers of a hemostatic agent were applied first (Surgicel®, Ethicon, Piscataway, NJ, USA) followed by instillation of 3 mL of autologous blood via a modified Fogarty® balloon catheter, resulting in immediate cessation of air leak (80). The pleural drain was removed after two days. In a case series of nine emphysema patients with PAL despite spigot placement (EWS®, Novatech, Grasse, France), bronchoscopic instillation of autologous blood plus thrombin was performed through a 2.45 mm catheter (PW-1L-1 and PW-5L-1, Olympus, Tokyo, Japan) passed into the gap between the spigot and the bronchial wall and directed peripherally under fluoroscopic guidance (81). The process was repeated if air leak persisted; the total amount of blood administered in each case did not exceed 25 mL. Air leak cessation was eventually achieved in 7/9 patients (77%) with diminution in the remaining 2. However, in 3 of the 7 successful cases, air leak was fully abolished only after subsequent pleurodesis.
Conclusions
Bronchoscopic interventions for PAL represent an evolving field within interventional pulmonology (Table 2). While they have yet to supplant operative management as the gold standard, particularly for larger defects, their place in the armamentarium may change over time as currently available techniques are refined and new ones are introduced. The endoscopic approach holds great appeal because of its relatively low invasiveness, which is of great value for the PAL patient who is at high surgical risk. This procedural category is sorely lacking comparative studies, but there is reason to believe that registry data and multicenter collaborations will help narrow the evidence gap in the not-too-distant future.
Table 2. Summary of the available non-valvular bronchoscopic approaches to PAL management described in case series of ≥5 patients. Data from references (35,36,41,42,52,53,61,64,66,71,74,75,81).
| Intervention | Type of bronchoscopy | Predominant fistula etiology | Number of series [cumulative patients] | Representative success rates (%)a |
|---|---|---|---|---|
| Devices | ||||
| Spigots | Flexible | Non-surgical | 2 [81] | 78–86 |
| Spigots + blood patch | Flexible | Emphysema | 1 [9] | 77 |
| Amplatzer™ occluders | Flexible | Surgical | 1 [10] | 82 |
| Metallic stents | Rigid | Surgical | 2 [14] | 100 |
| Tissue adhesives | ||||
| Cyanoacrylates | Flexible | Surgical | 2 [29] | 70–89 |
| Hemostatic agents | ||||
| Fibrin glue (Tisseel®) | Rigid | Surgical | 1 [29] | 55 |
| Hydrogel (Coseal®) | Flexible | Non-surgical | 1 [22] | 86 |
| Submucosal injections | ||||
| Polidocanol (Aethoxysclerol®) | Flexible | Surgical | 1 [35] | 66 |
| Silver nitrate | Flexible | Surgical | 1 [17] | 94 |
| Thermal therapy | ||||
| Nd:YAG laser | Flexible | Surgical | 1 [8] | 50 |
a, percentages reflect rates of complete cessation of leak, except for spigots wherein leak reduction is also included among the successes.
Acknowledgements
None.
Footnotes
Conflicts of Interest: The authors have no conflicts of interest to declare.
References
- 1.West D, Togo A, Kirk AJ. Are bronchoscopic approaches to post-pneumonectomy bronchopleural fistula an effective alternative to repeat thoracotomy? Interact Cardiovasc Thorac Surg 2007;6:547-50. 10.1510/icvts.2007.159319 [DOI] [PubMed] [Google Scholar]
- 2.Belda-Sanchís J, Serra-Mitjans M, Iglesias Sentis M, et al. Surgical sealant for preventing air leaks after pulmonary resections in patients with lung cancer. Cochrane Database Syst Rev 2010;(1):CD003051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Abolhoda A, Liu D, Brooks A, et al. Prolonged air leak following radical upper lobectomy: an analysis of incidence and possible risk factors. Chest 1998;113:1507-10. 10.1378/chest.113.6.1507 [DOI] [PubMed] [Google Scholar]
- 4.Wood DE, Cerfolio RJ, Gonzalez X, et al. Bronchoscopic management of prolonged air leak. Clin Chest Med 2010;31:127-33. 10.1016/j.ccm.2009.10.002 [DOI] [PubMed] [Google Scholar]
- 5.Cerfolio RJ. Recent advances in the treatment of air leaks. Curr Opin Pulm Med 2005;11:319-23. 10.1097/01.mcp.0000161056.85290.08 [DOI] [PubMed] [Google Scholar]
- 6.Singhal S, Ferraris VA, Bridges CR, et al. Management of alveolar air leaks after pulmonary resection. Ann Thorac Surg 2010;89:1327-35. 10.1016/j.athoracsur.2009.09.020 [DOI] [PubMed] [Google Scholar]
- 7.Cerfolio RJ. Advances in thoracostomy tube management. Surg Clin North Am 2002;82:833-48. 10.1016/S0039-6109(02)00026-9 [DOI] [PubMed] [Google Scholar]
- 8.Cerfolio RJ, Varela G, Brunelli A. Digital and smart chest drainage systems to monitor air leaks: the birth of a new era? Thorac Surg Clin 2010;20:413-20. 10.1016/j.thorsurg.2010.03.007 [DOI] [PubMed] [Google Scholar]
- 9.Darling GE, Abdurahman A, Yi Q-L, et al. Risk of a right pneumonectomy: role of bronchopleural fistula. Ann Thorac Surg 2005;79:433-7. 10.1016/j.athoracsur.2004.07.009 [DOI] [PubMed] [Google Scholar]
- 10.DeCamp MM, Blackstone EH, Naunheim KS, et al. Patient and surgical factors influencing air leak after lung volume reduction surgery: lessons learned from the National Emphysema Treatment Trial. Ann Thorac Surg 2006;82:197-206. 10.1016/j.athoracsur.2006.02.050 [DOI] [PubMed] [Google Scholar]
- 11.Panagopoulos ND, Apostolakis E, Koletsis E, et al. Low incidence of bronchopleural fistula after pneumonectomy for lung cancer. Interact Cardiovasc Thorac Surg 2009;9:571-5. 10.1510/icvts.2009.203646 [DOI] [PubMed] [Google Scholar]
- 12.Asamura H, Naruke T, Tsuchiya R, et al. Bronchopleural fistulas associated with lung cancer operations. Univariate and multivariate analysis of risk factors, management, and outcome. J Thorac Cardiovasc Surg 1992;104:1456-64. [PubMed] [Google Scholar]
- 13.Sirbu H, Busch T, Aleksic I, et al. Bronchopleural fistula in the surgery of non-small cell lung cancer: incidence, risk factors, and management. Ann Thorac Cardiovasc Surg 2001;7:330-6. [PubMed] [Google Scholar]
- 14.Deschamps C, Bernard A, Nichols FC, et al. Empyema and bronchopleural fistula after pneumonectomy: factors affecting incidence. Ann Thorac Surg 2001;72:243-7. 10.1016/S0003-4975(01)02681-9 [DOI] [PubMed] [Google Scholar]
- 15.Stolz AJ, Schützner J, Lischke R, et al. Predictors of prolonged air leak following pulmonary lobectomy. Eur J Cardiothorac Surg 2005;27:334-6. 10.1016/j.ejcts.2004.11.004 [DOI] [PubMed] [Google Scholar]
- 16.Li SJ, Fan J, Zhou J, et al. Diabetes mellitus and risk of bronchopleural fistula after pulmonary resections: a meta-analysis. Ann Thorac Surg 2016;102:328-39. 10.1016/j.athoracsur.2016.01.013 [DOI] [PubMed] [Google Scholar]
- 17.Zanotti G, Mitchell JD. Bronchopleural fistula and empyema after anatomic lung resection. Thorac Surg Clin 2015;25:421-7. 10.1016/j.thorsurg.2015.07.006 [DOI] [PubMed] [Google Scholar]
- 18.Martin J, Ginsberg RJ, Abolhoda A, et al. Morbidity and mortality after neoadjuvant therapy for lung cancer: the risks of right pneumonectomy. Ann Thorac Surg 2001;72:1149-54. 10.1016/S0003-4975(01)02995-2 [DOI] [PubMed] [Google Scholar]
- 19.Lois M, Noppen M. Bronchopleural fistulas: an overview of the problem with special focus on endoscopic management. Chest 2005;128:3955-65. 10.1378/chest.128.6.3955 [DOI] [PubMed] [Google Scholar]
- 20.Ricci ZJ, Haramati LB, Rosenbaum AT, et al. Role of computed tomography in guiding the management of peripheral bronchopleural fistula. J Thorac Imaging 2002;17:214-8. 10.1097/00005382-200207000-00006 [DOI] [PubMed] [Google Scholar]
- 21.Mendel T, Jakubetz J, Steen M, et al. Post-lobectomy bronchopleural fistula--a challenge for postoperative intensive care. Anasthesiol Intensivmed Notfallmed Schmerzther 2006;41:278-83. 10.1055/s-2006-925233 [DOI] [PubMed] [Google Scholar]
- 22.Gaur P, Dunne R, Colson YL, et al. Bronchopleural fistula and the role of contemporary imaging. J Thorac Cardiovasc Surg 2014;148:341-7. 10.1016/j.jtcvs.2013.11.009 [DOI] [PubMed] [Google Scholar]
- 23.Mark JB, McDougall IR. Diagnosis and localization of bronchopulmonary air leaks using ventilation scintigraphy. Chest 1997;111:286-9. 10.1378/chest.111.2.286 [DOI] [PubMed] [Google Scholar]
- 24.Ratliff JL, Hill JD, Tucker H, et al. Endobronchial control of bronchopleural fistulae. Chest 1977;71:98-9. 10.1378/chest.71.1.98 [DOI] [PubMed] [Google Scholar]
- 25.Herth FJ, Eberhardt R, Gompelmann D, et al. Radiological and clinical outcomes of using Chartis™ to plan endobronchial valve treatment. Eur Respir J 2013;41:302-8. 10.1183/09031936.00015312 [DOI] [PubMed] [Google Scholar]
- 26.Fann JI, Berry GJ, Burdon TA. The use of endobronchial valve device to eliminate air leak. Respir Med 2006;100:1402-6. 10.1016/j.rmed.2005.11.011 [DOI] [PubMed] [Google Scholar]
- 27.Snell GI, Holsworth L, Fowler S, et al. Occlusion of a broncho-cutaneous fistula with endobronchial one-way valves. Ann Thorac Surg 2005;80:1930-2. 10.1016/j.athoracsur.2004.06.037 [DOI] [PubMed] [Google Scholar]
- 28.Travaline JM, McKenna RJ, De Giacomo T, et al. Treatment of persistent pulmonary air leaks using endobronchial valves. Chest 2009;136:355-60. 10.1378/chest.08-2389 [DOI] [PubMed] [Google Scholar]
- 29.Gillespie CT, Sterman DH, Cerfolio RJ, et al. Endobronchial valve treatment for prolonged air leaks of the lung: a case series. Ann Thorac Surg 2011;91:270-3. 10.1016/j.athoracsur.2010.07.093 [DOI] [PubMed] [Google Scholar]
- 30.Firlinger I, Stubenberger E, Müller MR, et al. Endoscopic one-way valve implantation in patients with prolonged air leak and the use of digital air leak monitoring. Ann Thorac Surg 2013;95:1243-9. 10.1016/j.athoracsur.2012.12.036 [DOI] [PubMed] [Google Scholar]
- 31.Dooms CA, Decaluwe H, Yserbyt J, et al. Bronchial valve treatment for pulmonary air leak after anatomical lung resection for cancer. Eur Respir J 2014;43:1142-8. 10.1183/09031936.00117613 [DOI] [PubMed] [Google Scholar]
- 32.Gilbert CR, Casal RF, Lee HJ, et al. Use of one-way intrabronchial valves in air leak management after tube thoracostomy drainage. Ann Thorac Surg 2016;101:1891-6. 10.1016/j.athoracsur.2015.10.113 [DOI] [PubMed] [Google Scholar]
- 33.Reed MF, Gilbert CR, Taylor MD, et al. Endobronchial valves for challenging air leaks. Ann Thorac Surg 2015;100:1181-6. 10.1016/j.athoracsur.2015.04.104 [DOI] [PubMed] [Google Scholar]
- 34.Watanabe Y, Hiraki S, Araki M. Bronchial embolization using dental impression material in a case of pyelo-bronchial fistula with Candida fungemia. J Jpn Soc Bronchol 1991;13:607-10. [Google Scholar]
- 35.Watanabe Y, Matsuo K, Tamaoki A, et al. Bronchial occlusion with endobronchial Watanabe spigot. J Bronchology Interv Pulmonol 2003;10:264-7. [Google Scholar]
- 36.Kaneda H, Minami K-i, Nakano T, et al. Efficacy and long-term clinical outcome of bronchial occlusion with endobronchial Watanabe spigots for persistent air leaks. Respir Investig 2015;53:30-6. 10.1016/j.resinv.2014.09.002 [DOI] [PubMed] [Google Scholar]
- 37.Kida H, Muraoka H, Inoue T, et al. A novel technique for the placement of Endobronchial Watanabe Spigots into the bronchus: side-grasping method. J Bronchology Interv Pulmonol 2016;23:71-5. 10.1097/LBR.0000000000000213 [DOI] [PubMed] [Google Scholar]
- 38.Menard JW, Prejean CA, Tucker WY. Endoscopic closure of bronchopleural fistulas using a tissue adhesive. Am J Surg 1988;155:415-6. 10.1016/S0002-9610(88)80103-X [DOI] [PubMed] [Google Scholar]
- 39.Roksvaag H, Skalleberg L, Nordberg C, et al. Endoscopic closure of bronchial fistula. Thorax 1983;38:696-7. 10.1136/thx.38.9.696 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Chang CC, Hsu HH, Kuo SW, et al. Bronchoscopic gluing for post-lung-transplant bronchopleural fistula. Eur J Cardiothorac Surg 2007;31:328-30. 10.1016/j.ejcts.2006.11.002 [DOI] [PubMed] [Google Scholar]
- 41.Scappaticci E, Ardissone F, Ruffini E, et al. Postoperative bronchoplenral fistula: Endoscopic closure in 12 patients. Ann Thorac Surg 1994;57:119-22. 10.1016/0003-4975(94)90378-6 [DOI] [PubMed] [Google Scholar]
- 42.Chawla RK, Madan A, Bhardwaj P, et al. Bronchoscopic management of bronchopleural fistula with intrabronchial instillation of glue (N-butyl cyanoacrylate). Lung India 2012;29:11. 10.4103/0970-2113.92350 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Slade M, editor. Management of pneumothorax and prolonged air leak. Seminars in respiratory and critical care medicine. Thieme Medical Publishers, 2014. [DOI] [PubMed] [Google Scholar]
- 44.Lin J, Iannettoni MD. Closure of bronchopleural fistulas using albumin-glutaraldehyde tissue adhesive. Ann Thorac Surg 2004;77:326-8. 10.1016/S0003-4975(03)00750-1 [DOI] [PubMed] [Google Scholar]
- 45.Ranu H, Gatheral T, Sheth A, et al. Successful endobronchial seal of surgical bronchopleural fistulas using BioGlue. Ann Thorac Surg 2009;88:1691-2. 10.1016/j.athoracsur.2009.03.012 [DOI] [PubMed] [Google Scholar]
- 46.Finch CK, Pittman AL. Use of fibrin glue to treat a persistent pneumothorax with bronchopleural fistula. Am J Health Syst Pharm 2008;65:322-4. 10.2146/ajhp070101 [DOI] [PubMed] [Google Scholar]
- 47.McCarthy PM, Trastek VF, Bell DG, et al. The effectiveness of fibrin glue sealant for reducing experimental pulmonary air leak. Ann Thorac Surg 1988;45:203-5. 10.1016/S0003-4975(10)62438-1 [DOI] [PubMed] [Google Scholar]
- 48.Onotera RT, Unruh HW. Closure of a post-pneumonectomy bronchopleural fistula with fibrin sealant (Tisseel). Thorax 1988;43:1015. 10.1136/thx.43.12.1015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Jessen C, Sharma P. Use of fibrin glue in thoracic surgery. Ann Thorac Surg 1985;39:521-4. 10.1016/S0003-4975(10)61991-1 [DOI] [PubMed] [Google Scholar]
- 50.Glover W, Chavis T, Daniel T, et al. Fibrin glue application through the flexible fiberoptic bronchoscope: closure of bronchopleural fistulas. J Thorac Cardiovasc Surg 1987;93:470-2. [PubMed] [Google Scholar]
- 51.York EL, Lewall DB, Hirji M, et al. Endoscopic diagnosis and treatment of postoperative bronchopleural fistula. Chest 1990;97:1390-2. 10.1378/chest.97.6.1390 [DOI] [PubMed] [Google Scholar]
- 52.Hollaus PH, Lax F, Janakiev D, et al. Endoscopic treatment of postoperative bronchopleural fistula: experience with 45 cases. Ann Thorac Surg 1998;66:923-7. 10.1016/S0003-4975(98)00589-X [DOI] [PubMed] [Google Scholar]
- 53.Mehta HJ, Malhotra P, Begnaud A, et al. Treatment of alveolar-pleural fistula with endobronchial application of synthetic hydrogel. Chest 2015;147:695-9. 10.1378/chest.14-0823 [DOI] [PubMed] [Google Scholar]
- 54.Jones DP, David I. Gelfoam occlusion of peripheral bronchopleural fistulas. Ann Thorac Surg 1986;42:334-5. 10.1016/S0003-4975(10)62748-8 [DOI] [PubMed] [Google Scholar]
- 55.Sprung J, Krasna MJ, Yun A, et al. Treatment of a bronchopleural fistula with a Fogarty catheter and oxidized regenerated cellulose (surgicel). Chest 1994;105:1879-81. 10.1378/chest.105.6.1879 [DOI] [PubMed] [Google Scholar]
- 56.García-Polo C, León-Jiménez A, López-Campos JL, et al. Endoscopic sealing of bronchopleural fistulas with submucosal injection of a tissue expander: a novel technique. Can Respir J 2010;17:e23-4. 10.1155/2010/385036 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Martin WR, Siefkin AD, Allen R. Closure of a bronchopleural fistula with bronchoscopic instillation of tetracycline. Chest 1991;99:1040-2. 10.1378/chest.99.4.1040 [DOI] [PubMed] [Google Scholar]
- 58.Andreetti C, D’Andrilli A, Ibrahim M, et al. Submucosal injection of the silver–human albumin complex for the treatment of bronchopleural fistula. Eur J Cardiothorac Surg 2010;37:40-3. 10.1016/j.ejcts.2009.07.006 [DOI] [PubMed] [Google Scholar]
- 59.Høier-Madsen K, Schulze S, Pedersen VM, et al. Management of bronchopleural fistula following pneumonectomy. Scandinavian journal of thoracic and cardiovascular surgery 1984;18:263-6. 10.3109/14017438409109905 [DOI] [PubMed] [Google Scholar]
- 60.Stratakos G, Zuccatosta L, Porfyridis I, et al. Silver nitrate through flexible bronchoscope in the treatment of bronchopleural fistulae. J Thorac Cardiovasc Surg 2009;138:603-7. 10.1016/j.jtcvs.2008.10.054 [DOI] [PubMed] [Google Scholar]
- 61.Boudaya MS, Smadhi H, Zribi H, et al. Conservative management of postoperative bronchopleural fistulas. J Thorac Cardiovasc Surg 2013;146:575-9. 10.1016/j.jtcvs.2013.04.023 [DOI] [PubMed] [Google Scholar]
- 62.Takaoka K, Inoue S, Ohira S. Central bronchopleural fistulas closed by bronchoscopic injection of absolute ethanol. Chest 2002;122:374-8. 10.1378/chest.122.1.374 [DOI] [PubMed] [Google Scholar]
- 63.Lim AL, Kim CH, Hwang YI, et al. Bronchoscopic ethanolamine injection therapy in patients with persistent air leak from chest tube drainage. Tuberc Respir Dis (Seoul) 2012;72:441-7. 10.4046/trd.2012.72.5.441 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Varoli F, Roviaro G, Grignani F, et al. Endoscopic treatment of bronchopleural fistulas. Ann Thorac Surg 1998;65:807-9. 10.1016/S0003-4975(97)01427-6 [DOI] [PubMed] [Google Scholar]
- 65.Aynaci E, Kocatürk CI, Yildiz P, et al. Argon plasma coagulation as an alternative treatment for bronchopleural fistulas developed after sleeve pneumonectomy. Interact Cardiovasc Thorac Surg 2012;14:912-4. 10.1093/icvts/ivs001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Kiriyama M, Fujii Y, Yamakawa Y, et al. Endobronchial neodymium: yttrium-aluminum garnet laser for noninvasive closure of small proximal bronchopleural fistula after lung resection. Ann Thorac Surg 2002;73:945-8. 10.1016/S0003-4975(01)03417-8 [DOI] [PubMed] [Google Scholar]
- 67.Hirata T, Ogawa E, Takenaka K, et al. Endobronchial closure of postoperative bronchopleural fistula using vascular occluding coils and n-butyl-2-cyanoacrylate. Ann Thorac Surg 2002;74:2174-6. 10.1016/S0003-4975(02)04170-X [DOI] [PubMed] [Google Scholar]
- 68.Watanabe S, Watanabe T, Urayama H. Endobronchial occlusion method of bronchopleural fistula with metallic coils and glue. Thorac Cardiovasc Surg 2003;51:106-8. 10.1055/s-2003-38981 [DOI] [PubMed] [Google Scholar]
- 69.Shimizu J, Takizawa M, Yachi T, et al. Postoperative bronchial stump fistula responding well to occlusion with metallic coils and fibrin glue via a tracheostomy: a case report. Ann Thorac Cardiovasc Surg 2005;11:104-8. [PubMed] [Google Scholar]
- 70.Sivrikoz CM, Kaya T, Tulay CM, et al. Effective approach for the treatment of bronchopleural fistula: application of endovascular metallic ring-shaped coil in combination with fibrin glue. Ann Thorac Surg 2007;83:2199-201. 10.1016/j.athoracsur.2007.01.005 [DOI] [PubMed] [Google Scholar]
- 71.Fruchter O, Kramer MR, Dagan T, et al. Endobronchial closure of bronchopleural fistulae using amplatzer devices: our experience and literature review. Chest 2011;139:682-7. 10.1378/chest.10-1528 [DOI] [PubMed] [Google Scholar]
- 72.Klotz LV, Gesierich W, Schott-Hildebrand S, et al. Endobronchial closure of bronchopleural fistula using Amplatzer device. J Thorac Dis 2015;7:1478-82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Fruchter O, Bruckheimer E, Raviv Y, et al. Endobronchial closure of bronchopleural fistulas with Amplatzer vascular plug. Eur J Cardiothorac Surg 2012;41:46-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Cao M, Zhu Q, Wang W, et al. Clinical application of fully covered self-expandable metal stents in the treatment of bronchial fistula. Thorac Cardiovasc Surg 2016;64:533-9. 10.1055/s-0034-1396681 [DOI] [PubMed] [Google Scholar]
- 75.Dutau H, Breen DP, Gomez C, et al. The integrated place of tracheobronchial stents in the multidisciplinary management of large post-pneumonectomy fistulas: our experience using a novel customised conical self-expandable metallic stent. Eur J Cardiothorac Surg 2011;39:185-9. 10.1016/j.ejcts.2010.05.020 [DOI] [PubMed] [Google Scholar]
- 76.Chae EY, Shin JH, Song H-Y, et al. Bronchopleural fistula treated with a silicone-covered bronchial occlusion stent. Ann Thorac Surg 2010;89:293-6. 10.1016/j.athoracsur.2009.05.068 [DOI] [PubMed] [Google Scholar]
- 77.Colt HG, Murgu SD. Closure of pneumonectomy stump fistula using custom Y and cuff-link-shaped silicone prostheses. Ann Thorac Cardiovasc Surg 2009;15:339-42. [PubMed] [Google Scholar]
- 78.Ferraroli GM, Testori A, Cioffi U, et al. Healing of bronchopleural fistula using a modified Dumon stent: a case report. Journal of cardiothoracic surgery 2006;1:16. 10.1186/1749-8090-1-16 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Manley K, Coonar A, Wells F, et al. Blood patch for persistent air leak: a review of the current literature. Curr Opin Pulm Med 2012;18:333-8. 10.1097/MCP.0b013e32835358ca [DOI] [PubMed] [Google Scholar]
- 80.Wiaterek G, Lee H, Malhotra R, et al. Bronchoscopic blood patch for treatment of persistent alveolar-pleural fistula. J Bronchology Interv Pulmonol 2013;20:171-4. 10.1097/LBR.0b013e31828f4de0 [DOI] [PubMed] [Google Scholar]
- 81.Mizumori Y, Nakahara Y, Kawamura T, et al. Intrabronchial Infusion of Autologous Blood Plus Thrombin for Intractable Pneumothorax After Bronchial Occlusion Using Silicon Spigots: A Case Series of 9 Patients With Emphysema. J Bronchology Interv Pulmonol 2016;23:199. 10.1097/LBR.0000000000000289 [DOI] [PMC free article] [PubMed] [Google Scholar]