

Abstract
A case is presented of severe abdominal pain around a healed scar following fracture of a heterotopically formed bone. This should be considered an unusual differential diagnosis in patients with acute pain of unknown origin who had open abdominal surgery in the past. To our knowledge, we have also reported the first case of hetertopic bone formation incorporating a prolene mesh.
Keywords: Abdominal pain, Fracture, Heterotopically formed bone, Prolene mesh
Bone formation within abdominal incisions is a recognised phenomenon. As most patients remain asymptomatic, the actual incidence is unknown. Presentation with acute abdominal pain due to fracture of the heterotopically formed bone is a rare occurrence with only two previously published cases.1,2 We also report the first instance of bone formation incorporating a prolene mesh.
Case history
A 42-year-old man was admitted with a 24-h history of sudden onset epigastric pain that woke him from sleep and was exacerbated by movement. On examination, he was guarding in the epigastrium over a mid-line incision extending to the umbilicus. He had undergone a laparotomy 17 years previously for a perforated peptic ulcer.
Apart from raised inflammatory markers (white cell count 14 ·109/l and C-reactive protein 15 mg/l), serum bio-chemistry was entirely normal including the amylase, calcium, phosphate and urea. His chest X-ray did not show air under the diaphragm and a contrast computed tomography (CT) abdomen showed a possible foreign body within the rectus sheath.
Due to diagnostic uncertainty, an exploratory laparotomy was performed. On exploring the mid-line incision, a prolene mesh was found between the posterior rectus sheath and peritoneum. Upon entering the abdominal cavity, a hard mass was palpated 3 cm left of the mid-line and superficial to the peritoneum. Further dissection revealed a macroscopically mature bone, irregular in shape with branches in the coronal plane measuring approximately 6 cm in maximal length. It incorporated the mesh and had a periosteal layer and a nutrient artery. The cranial border was more than 4 cm from the inferior border of the xiphisternum (Fig. 1).
Figure 1.
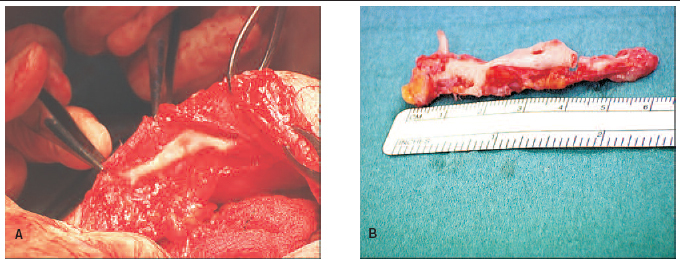
(A) Intra-operative finding of heterotopic bone on internal aspect of anterior abdominal wall, lateral to the previous midline incision, incorporating and surrounded by prolene mesh. (B) Dissected bone: note fracture of caudal branch, bone marrow cavity and orifice of nutrient artery.
Whilst dissecting out the bony fragment, the caudal limb was found to be fractured. No abnormalities of the stomach, proximal small bowel, liver or spleen were found during laparotomy.
Postoperatively, the patient made an uneventful recovery and was discharged after 2 days. Given the acute onset, the operative findings and resolution of symptoms following resection of the bone, we believe this to be a fractured hetero-topically formed bone presenting with acute abdominal pain.
Histological examination confirmed lamellar bone with embedded mesh. Bone marrow was present.
Discussion
Heterotopic ossification is the formation of bone anywhere outside the skeletal system, including within muscle, tendons and ligaments. Most commonly, it is encountered following operations for acetabular fractures. Mysoitis ossificans describes the subset of cases occurring within muscle. It can be further subdivided into myositis ossificans progressiva, a rare autosomal dominant genetic disorder and myositis ossificans traumatica (also known as myositis ossificans circum-scripta or fibrodysplasia ossificans circumpsripta) which describes the formation of bone within muscle following trauma, typically a contact sport injury such as a kick to the mid-thigh but also after surgical trauma involving the rectus muscle during laparotomy. The ossification in these instances resembles actual bone both histologically and radiologically, differentiating it from dystrophic calcification where there is disorganised calcification within soft tissues without the presence of osteoblasts or bone marrow components.3
Over 100 cases of heterotopic bone formation in abdominal incisions have been described since the first report by Askanazy in 1901. True incidence is difficult to ascertain as most patients remain asymptomatic. With a male to female ratio of 10:1, heterotopic bone formation has been reported exclusively in vertical incisions or in the vertical component of curved incisions.4 It can occur in any layer between the subcutaneous tissues and peritoneum and is usually not connected to the xiphoid.1 The size of the bone varies and the largest reported was 15 × 4.5 cm.5
Most patients complain of chronic regional pain or a palpable mass with loss of movement presenting within a year of the surgery.3,5 The literature identifies only two cases presenting with acute onset of pain following fracture of the bone. Both patients presented several years post-operatively.1,2
Differential diagnosis includes dystrophic calcification, neoplastic lesions and retained foreign body. Further investigation to exclude hypoparathyroidism is warranted.
Treatment is reserved for symptomatic patients and consists of surgical excision and primary closure. Recurrence has only been reported in three patients where NSAIDs or radiotherapy may be useful.3
We are not aware of any reported cases of heterotopic bone formation incorporating a polypropylene or polytetra-fluoroethylene mesh. In our patient, the bone was found 3–4 cm lateral to the initial mid-line incision, raising the possibility of the mesh acting as a matrix on which an ossification process commenced prior to migration from the mid-line. There are also no reports of a heterotopically formed bone with a nutrient artery.
References
- 1.Leis VM, Cotlar AM. Fractured heterotopic bone in a midline abdominal wound. Curr Surg 2003; : 193–5. [DOI] [PubMed] [Google Scholar]
- 2.Mestan MA, Bassano JM. Fractured heterotopic bone in myositis ossificans traumatica. J Manipul Physiol Ther 2001; : 296–9. [DOI] [PubMed] [Google Scholar]
- 3.Reardon MJ, Tillou A, Mody DR, Reardon PR. Heterotopic calcification in abdominal wounds. Am J Surg 1997; : 145–7. [DOI] [PubMed] [Google Scholar]
- 4.Jacobs JE, Birnbaum BA, Siegelman ES. Heterotopic ossification of midline abdominal incisions: CT and MR imaging findings. AJR Am J Roentgenol 1996; : 579–84. [DOI] [PubMed] [Google Scholar]
- 5.Degirmenci B, Acar M, Albayrak R, Haktanir A, Ycel A. Heterotopic bone formation in upper midline abdominal incision. Turk J Med Sci 2005; : 189–91. [Google Scholar]