

Abstract
A patient with phyllodes tumour of the breast is discussed. During follow-up, she presented with intestinal obstruction caused by ileocaecal intussusception. The cause of the intussusception was metastatic phyllodes tumour, which is a unique presentation.
Keywords: Phyllodes, Metastasis, Caecum, Intussusception
Phyllodes tumours of the breast are rare fibro-epithelial tumours. They form less than 1% of breast neoplasms.1 They are classified as benign, borderline or malignant. In most cases, phyllodes are benign and adequately treated by wide local excision.
Metastasis, however, can develop in up to 21% of patients.2 This can occur with or without local recurrence. Treatment of metastatic phyllodes should follow guidelines for sarcoma rather than breast cancer and the outcome is poor. The most common sites of metastasis are the lungs and bones.3 Other reported sites of metastasis, including the liver and brain, are rare. We report on a case of phyllodes tumour with metastasis to a site which has not been reported before, with an uncommon presentation.
Case history
A 52-year-old woman was referred with a locally advanced and neglected left breast phyllodes tumour. The tumour was 30 cm in diameter. It involved the entire left breast with impending skin ulceration. Pre-operative evaluation with chest and abdomen computed tomography (CT) scans did not reveal any distant metastasis.
The patient underwent a successful, wide, local excision, which included the entire breast with the underlying pectoralis major and minor muscles. The defect was reconstructed with a transverse rectus abdominis myocutaneous (TRAM) flap. The tumour was completely excised with negative margins.
Thirteen months later, she re-presented with abdominal pain associated with vomiting and constipation. Clinical examination revealed right-sided abdominal mass associated with severe localised tenderness. CT scan was done which suggested the presence of ileocolic intussusception (Fig. 1). Laparotomy was performed the same day. The operative findings were ileocolic intussusception reaching the transverse colon. She underwent right hemicolectomy. Her postoperative recovery was uneventful. The pathology report confirmed the presence of ileocaecal intussusception secondary to metastatic phyllodes tumour to the caecal wall, just adjacent to the ileocaecal valve (Fig. 2). The histological features of the tumour were similar to the resected breast tumour, with abundant mitoses (80 MF/10 HPF). The cells were negative for CK, S100, SMA, desmin, CD34 and C-kit. Unfortunately, the patient went on to develop other metastases to the lungs and limbs (soft tissues) during the following months, and finally succumbed to her metastatic disease 18 months later.
Figure 1.
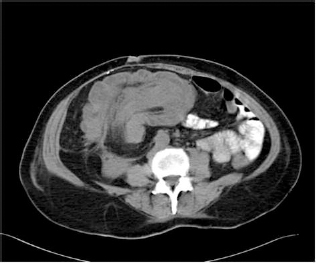
CT scan showing ileocaecal intussusception.
Figure 2.

Phyllodes tumour in the colonic wall (haematoxylin and eosin stain ×100).
Discussion
Phyllodes tumour metastasis is an uncommon event, occurring in up to 21% of cases.2 Most commonly, metastases occur to the lungs (84.5%) and bones (39%). Less common sites include the liver (5%), brain and soft tissues. Treatment of metastasis is usually with chemotherapy. However, in some cases of visceral metastasis, surgical excision might be indicated, especially with a localised and resectable disease. Nevertheless, the prognosis remains very poor.
The gastrointestinal tract is very rarely involved by metastatic phyllodes tumours. We found only five cases reported in the literature of metastasis to the gastrointestinal tract (excluding the liver).4–8 It is interesting to note that four of those cases had metastasis to the region of the pancreas and duodenum. Most presented with upper gastrointestinal bleeding. One patient presented with obstructive jaundice. The fifth case had metastasis to the ileum causing partial intestinal obstruction.8 Our patient had metastasis to the caecum. In our literature review, we could not find any case of metastasis to the colon from phyllodes tumour of the breast.
Intussusception in adults is usually caused by tumours,9 either primary or secondary. Primary tumours include adenocarcinomas, polyps and hamartomas. Secondary tumours are rare and include melanomas, kidney tumours and lymphomas. To our knowledge, this is the first case of intussusception caused by a metastatic phyllodes tumour.
Surgical resection is the mainstay of treatment of adult intussusception. It is indicated to identify and relieve the cause of obstruction. However, the prognosis depends mainly on the pathological cause of intussusception. Metastatic phyllodes tumours usually have a dismal prognosis. Our patient underwent right hemicolectomy with good immediate outcome and palliation. Nevertheless, she developed metastases in other organs during the ensuing months and succumbed to her metastatic disease about 18 months later.
References
- 1.Rowell MD, Perry RR, Hsiu JG, Barranco SC. Phyllodes tumours. Am J Surg 1993; : 376–9. [DOI] [PubMed] [Google Scholar]
- 2.Cedermark GC, Rutqvist LE, Rosendahl I, Silfversward C. Prognostic factors in cystosarcoma phyllodes. A clinicopathologic study of 77 patients. Cancer 1991; : 2017–22. [DOI] [PubMed] [Google Scholar]
- 3.Kapiris I, Nasiri N, A’Hern R, Healy V, Gui GP. Outcome and predictive factors of local recurrence and distant metastases following primary surgical treatment of high-grade malignant phyllodes tumours of the breast. Eur J Surg Oncol 2001; : 723–30. [DOI] [PubMed] [Google Scholar]
- 4.Yu PC, Lin YC, Chen HM, Chen MF. Malignant phyllodes tumour of the breast metastasizing to the pancreas: case report. Chang Gung Med J 2000; : 503–7. [PubMed] [Google Scholar]
- 5.Wolfson P, Rybak BJ, Kim U. Cystosarcoma phyllodes metastatic to the pancreas. Am J Gastroenterol 1978; : 184–7. [PubMed] [Google Scholar]
- 6.Asoglu O, Karanlik H, Barbaros U, Yanar H, Kapran Y, Kecer M et al. Malignant phyllodes tumor metastatic to the duodenum. World J Gastroenterol 2006; : 1649–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ang TL, Ng VWL, Fock KM, Teo EK, Chong CK. Diagnosis of a metastatic phyllodes tumor of the pancreas using EUS-FNA. J Pancreas (Online) 2007; : 35–8. [PubMed] [Google Scholar]
- 8.Kelly RJ, Barrett C, Swan N, McDermott R. Metastatic phyllodes tumor causing small-bowel obstruction. Clin Breast Cancer 2009; ; 193–5. [DOI] [PubMed] [Google Scholar]
- 9.Haas EM, Etter EL, Ellis S, Taylor TV. Adult intussusception. Am J Surg 2003; : 75–6. [DOI] [PubMed] [Google Scholar]