

Abstract
Multiple fractures of the humerus are a rare injury and usually associated with high-energy trauma. We report an unusual injury with co-existing fractures of the proximal humerus and humeral shaft without shoulder dislocation. We discuss our experience in the diagnosis and treatment of a 39-year-old man with co-existing fractures of proximal humerus and ipsilateral humeral shaft with radial nerve deficit. He was successfully managed with open reduction and fixation of the fractures. At follow-up 1 year after injury, he is back at work and has a good range of shoulder movements. The radial nerve injury is showing signs of recovery. In high-energy trauma to the shoulder, unusual fracture patterns with associated neurovascular deficits may be seen and this case report describes our experience with one such rare injury.
Keywords: Multiple fractures, Humerus
The incidence of injuries to the proximal humerus is 3–5%.1 There are rare occasions when a humeral shaft fracture is associated with injury to the proximal humerus. In the few case reports that have been published describing this injury, the proximal humerus fracture is invariably associated with a shoulder dislocation.2
We report a case of a 39-year-old man who suffered high-energy trauma to his shoulder that resulted in co-existing fractures of the proximal humerus and humeral shaft without shoulder dislocation. The fracture was successfully managed with open reduction and rigid internal fixation.
To the best of our knowledge, this pattern of injury has never been described in the published English literature. We discuss our experience with diagnosis and management.
Case report
A 39-year-old salesman who performs quad biking as a hobby sustained this injury when he attempted a front end stand with his bike at 40 mph speed. The mechanism of injury was a direct fall.
He was brought to the emergency department where he underwent an initial trauma assessment (ATLS) that revealed no life-threatening injuries. He complained of pain and loss of movement in his left shoulder. Clinical examination revealed a swollen, deformed, left arm with no open wounds. A neurovascular assessment of his left upper limb revealed palpable distal pulses and no nerve deficit.
Plain radiographs of his shoulder and humerus showed a transverse fracture of the mid-shaft of humerus and a two-part fracture of the proximal humerus. There was no evidence of glenohumeral dislocation (Fig. 1).
Figure 1.
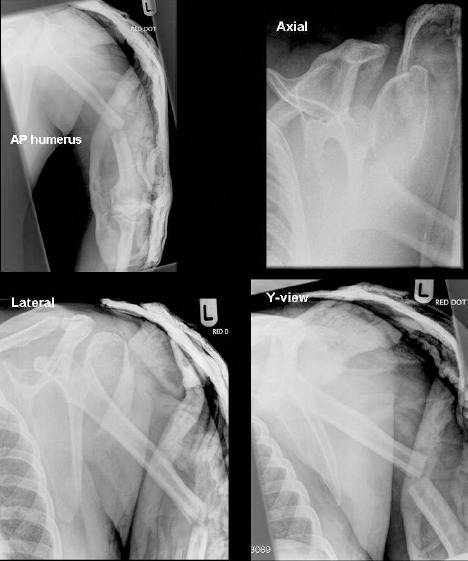
Initial plain radiographs (multiple views), left shoulder and arm.
Subsequent clinical examination revealed that he had developed sensory loss in the first dorsal web space and limited extension of fingers corresponding to radial nerve neuropathy. Therefore, a definitive management plan was made to perform an open reduction and fixation of the fracture.
He successfully underwent an open reduction and fixation of the proximal fragment with a Philos® plate (Stratec, UK), and lateral humeral plate (Synthes, UK) to stabilise the humeral shaft fracture. Intra-operatively, the radial nerve was found to be intact in its entirety. There were no immediate complications following the procedure and he was discharged home at 1 week with a wrist splint and shoulder immobiliser (Fig. 2). He was followed up in the out-patient clinic at regular intervals. Physiotherapy was initiated after 6 weeks to progress from protected passive to active range of movement exercises. At follow-up, 1 year after injury, the patient had made a good recovery and has returned to work. He has good range of movement in his shoulder with abduction of 130º and forward flexion up to 140º. The radial nerve injury is showing signs of recovery clinically and on EMG study.
Figure 2.
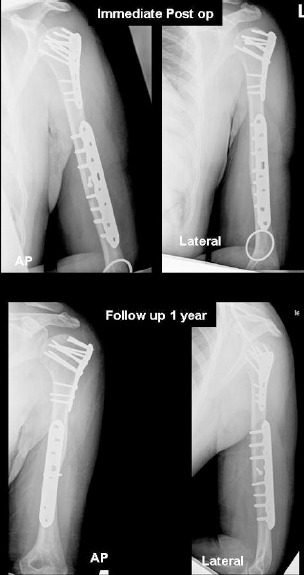
Postoperative plain radiographs, anteroposterior and lateral views.
Discussion
Fractures of the proximal humerus are a common injury in osteoporotic bone.1 However, in young adults, it is usually due to high-energy trauma with devastating resultant injuries. This case report describes a rare combination of proximal and mid-shaft humerus fracture without shoulder dislocation.
The common injury forces that result in shoulder fractures include tension, axial compression, torsion, bending or axial compression with bending.3 In high-energy trauma, multiple forces are involved and the fracture pattern depends on the most predominant force. Kontakis et al.2 reported dislocation of the shoulder and ipsilateral fractures of the humeral shaft, a combination of forces have been implicated to explain the mechanism of this injury. Similarly, in our patient, the fracture resulted from a combination of complex forces. The continuing momentum of his body as he was thrown off the quad bike and landed on the ground must have caused shearing and axial compression across the proximal humerus. There must have been a concomitant bending force if he fell on an outstretched hand to result in the mid-shaft transverse fracture.
Fractures of the humerus are also associated with a high incidence of neurovascular injuries with an incidence ranging from 3–34%.2,4 It is, therefore, important to perform an initial neurovascular assessment and to repeat this after application of a plaster. In the current case, we think the radial nerve injury was neuropraxia.
In the treatment of unstable fractures, open reduction and stabilisation is recommended for good outcome. Although shoulder dislocation with ipsilateral shaft fractures have been treated with open or closed methods with good results,2 we think in our case that anatomical reduction was necessary to achieve satisfactory results. There is a risk of avascular necrosis in severely displaced fractures but, in a recent prospective study of the natural history of complex fractures of the proximal humerus, this was a rare complication.5
One of the challenges in management of this injury was definition of the fracture pattern and identifying an appropriate fixation device. This was an unstable fracture pattern and we believed that the relative stability provided by intramedullary nailing devices would not satisfactorily address the complex nature of both proximal and distal fractures.
Our other option was to use the proximal humerus locking plate (Philos®) which provides a biological fixation with anatomical reduction. However, pre-operative templating highlighted the lack of a suitably long plate and there would have been inadequate distal fixation beyond the distal end of the fracture. This raised the concern of stress risers by using two separate plate fixation devices to fix the proximal and shaft fracture. However, since we had to address the issue of the neurological deficit, a radial nerve exploration was paramount. Therefore, the decision to attempt an open reduction and rigid internal fixation was made. We were able to achieve a stable, rigid fixation which allowed early mobilisation and we did not encounter any complications related to the implants during the 1-year follow-up.
Conclusions
It is important to recognise that high-energy trauma to the shoulder can result in unusual fracture patterns and has a high risk of associated neurovascular injuries. This association of proximal humerus fracture (with or without dislocation) and ipsilateral humeral shaft fracture should be recognised and probably should be included in future classification systems. This injury requires an early referral to an orthopaedic surgeon for definitive management.
Acknowledgement
The authors dedicate this work to the late Mr J Dufosse FRCS, Consultant Orthopaedic Surgeon, University Hospital of North Tees.
References
- 1.Rose SH, Melton LJ III, Morrey BF, Ilstrup DM, Riggs BL. Epidemiologic features of humeral fractures. Clin Orthop 1982; (): 24–30. [PubMed] [Google Scholar]
- 2.Kontakis GM, Galanakis IA, Steriopoulos KA. Dislocation of the shoulder and ipsilateral fracture of the humeral shaft: case reports and literature review. J Trauma 1995; : 990–2. [DOI] [PubMed] [Google Scholar]
- 3.Neer CS. Displaced proximal humeral fractures: part I. Classification and evaluation. J Bone Joint Surg Am 1970; : 1077–89. [PubMed] [Google Scholar]
- 4.Ring D, Chin K, Jupiter JB. Radial nerve palsy associated with high-energy humeral shaft fractures. J Hand Surg Am 2004; : 144–7. [DOI] [PubMed] [Google Scholar]
- 5.Edelson G, Safuri H, Salami J, Vigder F, Militianu D. Natural history of complex fractures of the proximal humerus using a three-dimensional classification system. J Shoulder Elbow Surg 2008; : 399–409. [DOI] [PubMed] [Google Scholar]