

Abstract
Situs inversus totalis (SIT) is a rare defect of genetic predisposition. It may cause difficulties in the diagnostic and therapeutic management of abdominal pathology due to the mirror-image anatomy. We report the management of a case of symptomatic cholelithiasis with emphasis on its surgical technique combined with a review of the literature.
Keywords: Situs inversus totalis, Cholelithiasis, Laparoscopic cholecystectomy
Case history
A 53-year-old man with known situs inversus totalis (SIT) presented to out-patients with pains in his left upper quadrant. He was a diet-controlled diabetic. An upper abdominal ultrasound scan confirmed a left-sided liver and gallbladder containing numerous calculi. Liver function tests were normal and a laparoscopic chole-cystectomy was performed.
Operative technique
The patient was placed in the supine position with slight head-up and right tilt to improve visualisation. Two surgeons, both right-handed, were positioned to the right of the patient. The monitor was at the head of the patient on his left side. Four ports were used in total. A 10-mm camera port was inserted infra-umbilically and an additional 10-mm port in the subxiphoid area in the mid-line. A 30-degree camera was used. Two 5-mm ports were inserted in the left subcostal region at the mid-clavicular and the anterior axillary lines (Fig. 1).
Figure 1.
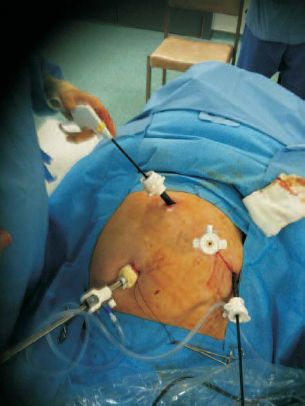
Port site positioning (head end at top of image).
Initial laparoscopy confirmed SIT. The caecum was positioned on the left, the spleen on the right and liver on the left together with the gallbladder (Fig. 2). The left anterior axillary line port was used to grasp the gallbladder fundus and provide cephalic traction. Hartmann’s pouch was dissected using a grasper from the subxiphoid port and hook diathermy via the left mid-clavicular line port (Figs 3 and 4).
Figure 2.

Initial laparoscopy.
Figure 3.
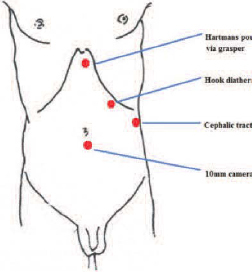
Port site positioning.
Figure 4.
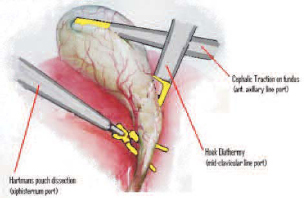
Gallbladder retraction.
Dissection of Calot’s triangle proved straightforward. The dissection was carried out through the left mid-clavicular line port with the dominant hand and clips were applied to the cystic artery and cystic duct through the subxiphoid port. There was no associated aberrant biliary anatomy encountered. The gallbladder was delivered through the subxiphoid port using an Endocatch® retrieval bag.
The duration of the operation was 65 min, a length slightly longer than our standard laparoscopic cholecystectomy. Recovery was uneventful and the patient was discharged the following day.
Discussion
Situs inversus was first describes by Scottish physician and pathologist Matthew Baillie. It is generally an autosomal recessive condition, although it can be X-linked. In the absence of congenital heart defects, individuals with situs inversus are phenotypically unimpaired. There is a 5–10% prevalence of congenital heart disease in individuals with SIT. Most commonly this is transposition of the great vessels and this must be assessed pre-operatively.
There is no evidence to suggest that symptomatic cholelithiasis is more frequent with SIT. Although the majority of patients with SIT describe the symptoms of gallbladder disease in the left upper quadrant, epigastric pain in 30% and right upper quadrant pain in 10% has been reported previously.1 It is thought that the central nervous system may not share in the visceral transposition.
Since Mouret performed the first laparoscopic cholecystectomy in 1987, it has become the standard treatment for gallbladder disease. In 2006, Bediou et al.2 reported the 13th case of laparoscopic cholecystectomy in SIT in the world. Previous reports have stated that SIT is not a contra-indication to laparoscopic cholecystectomy.3,4 Recognised difficulties are noted in the right-handed surgeon who must show care not to cross arms to retract Hartmann’s pouch for skeletalisation of Calot’s triangle. Previous authors have suggested that the assistant for optimal ergodynamics carries out such retraction. Others suggest operating between the legs with the patient in a Lloyd–Davis position.5
Conclusions
This case study confirms other authors’ reports that laparoscopic cholecystectomy can be performed safely in the patient with SIT if care is taken to familiarise one’s self with the mirror image anatomy.
Acknowledgement
Written consent was obtained from the patient in order to publish this case report.
References
- 1.Rao PG, Katariya RN, Sood S, Rao PL. Situs inversus totalis with calculus cholecystitis and mucinous cystadenomas of ovaries. J Postgrad Med 1977; : 89–90. [PubMed] [Google Scholar]
- 2.Bedioui H, Chebbi F, Ayadi S, Makni A, Fteriche F, Ksantini R et al. Laparoscopic cholecystectomy in a patient with situs inversus. Ann Chir 2006; : 398–400. [DOI] [PubMed] [Google Scholar]
- 3.Yaghan RJ, Gharaibeh KI, Hammori S. Feasibility of laparoscopic cholecystectomy in situs inversus. J Laparoendosc Adv Surg Tech 2001; : 233–7. [DOI] [PubMed] [Google Scholar]
- 4.Nursal TZ, Baykal A, Iret D, Aran O. Laparoscopic cholecystectomy in a patient with situs inversus totalis. J Laparoendosc Adv Surg Tech A 2001; : 239–41. [DOI] [PubMed] [Google Scholar]
- 5.Kumar S, Fusai G. Laparoscopic cholecystectomy in situs inversus totalis with left sided gall bladder. Ann R Coll Surg Engl 2007; : 186. [DOI] [PMC free article] [PubMed] [Google Scholar]