

Abstract
Background:
Circulating-Tumour-Cells (CTC) provide a blood biomarker for early carcinogenesis, cancer progression and treatment effectiveness. An increase in CTCs is associated with cancer progression, a CTC decrease with cancer containment or remission. Several technologies have been developed to identify CTC, including the validated Isolation-by-Size-of-Epithelial-Tumour (ISET, Rarecells) technology, combining blood filtration and microscopy using standard histo-pathological criteria.
Methods:
This observational study compared CTC count to cancer status and cancer risk, by monitoring treatment effectiveness in cancer patients and by screening for CTC in asymptomatic patients with risk factors, including family history of cancer.
Results:
Between Sept-2014 and Dec-2016 we undertook 600 CTC tests (542 patients), including 50% screening requests of patients without cancer diagnosis but with risk factors. CTC were detected in all cancer patients (n=277, 100%), and in half of the asymptomatic patients screened (50%, 132 out-of 265 patients). Follow-up tests including scans, scheduled within 1-10 months of positive CTC tests, found early cancerous lesions in 20% of screened patients. In 50% of male patients with CTC and normal PSA (prostate-specific-antigen) levels, PSMA-PET scans revealed increased uptake in the prostate, indicative of early prostate cancer. Other types of cancers detected by CTC screening and subsequent scans included early breast, ovarian, lung, or renal cancer. Patients with CTC were advised on integrative approaches including immune-stimulating and anti-carcinogenic nutritional therapies. CTC repeat tests were available in 10% of patients with detected CTC (40 out-of 409 patients, n=98 CTC tests) to assess treatment effectiveness, suggesting nutritional therapies to be beneficial in reducing CTC count.
Conclusions:
CTC screening provided a highly sensitive biomarker for the early detection of cancer, with higher CTC counts being associated with higher risk of malignancy. CTC monitoring over time indicated treatment effectiveness. Nutrients with anti-carcinogenic properties could reduce CTC count, and included curcumin, garlic, green tea, grape seed, modified citrus pectin, and medicinal mushroom extract.
Keywords: Circulating Tumour Cells (CTC), cancer screening, treatment effectiveness, integrative nutritional therapy
Introduction
Circulating Tumour Cells (CTC) provide a biomarker for cancer prognosis and treatment effectiveness, whereby an increase in CTC count is associated with cancer progression, shorter progression free survival, and shorter overall survival compared to a decrease in CTC count (Cristofanilli et al., 2004, Hayes et al., 2006). In a group of 177 women with metastatic breast cancer, CTC count was directly related to disease progression and survival, whereby a CTC count of less than 0.7 CTC/ml (5 CTC in 7.5 ml of whole blood) had a longer progression free survival and overall survival compared to a CTC count of more than 0.7 CTC/ml (median progression-free survival 2.7 months versus 7.0 months, p<0.001), and median overall survival (10.1 months versus >18 months, p<0.001) (Cristofanilli et al., 2004). Furthermore, the type of CTC cells, either single cells or CTC clusters, are a prognostic predictor of metastasizing potential and overall survival, with a hazard ratio of 14.5 (p<0.001) for ≥3-cell CTC clusters compared to no CTC (Wang et al., 2017).
Presence of CTC has also been associated with early carcinogenesis and risk of cancer (Ilie et al., 2014). In a study of cancer-free patients with chronic obstructive pulmonary disease (COPD), CTC were detected in 3% of the patients, who developed lung cancer within 1-4 years after CTC screening (Ilie et al., 2014).
Several technologies have been developed to identify CTC, including the Isolation-by-Size-of-Epithelial-Tumour (ISET) technique (Rarecells, France) which involves blood filtration, and analysis by microscopy using standard histo-pathological/ cyto-morphological criteria (Vona et al., 2000, Laget et al., 2017). Blood is treated to lyse red blood cells, and remaining rare cells, including CTC and inflammatory (white blood) cells, are then enriched on a filter, stained and analysed by standard cytological microscopy. The ISET technology allows direct identification of CTC, independent of the presence of tumour markers (Krebs et al., 2012). For example, the Cellsearch or Maintrac technologies use Epithelial-Cell-Adhesion Molecule (EpCAM) markers to detect CTC (Pachmann et al., 2011, Paterlini-Brechot and Benali, 2007). The ISET technology enables CTC to be detected in all types of cancer, including solid tumours, small-cell type cancers and blood cancers (Laget et al., 2017). Furthermore, blood type cancer cells don’t express the EpCAM markers, and in cancer cells undergoing normal morphogenetic processes, also known as epithelial mesenchymal transition (EMT), which can lead to loss or gain of tumour markers including EpCAM markers (Barriere et al., 2014).
In addition, the ISET technology allows observation of morphological changes of atypical cells, and therefore allows distinction between CTC with malignant features (3-4 criteria out of 4 for malignancy), ‘CTC’ with uncertain malignant features (2-3 criteria), and benign circulating epithelial cells and cell clusters (CEC), as well as reactive inflammatory cells (Hofman et al., 2011b). Changes of the normal morphology of cells into atypical cells are meaningful, and can be regarded as precursors in cancer development (Hofman et al., 2011a, Garcia et al., 2007).
Because of the morphological changes of cells during carcinogenesis, the identification of (atypical cells or) CTC by ISET technology may be superior to other indirect tumour marker dependent methodologies. For example, the CTC count was more accurate on average with the ISET methodology compared to the Cellsearch methodology in metastatic prostate and lung cancer patients (Farace et al., 2011).
The ISET technology has been validated in several published studies, providing high sensitivity (1 CTC/ml), and high specificity (0 CTC/ml in 600 healthy donors) in cancer patients with various types of cancer including liver, lung, pancreatic cancer, soft-tissue sarcoma, and melanoma (Hofman et al., 2012, Vona et al., 2004, Khoja et al., 2014, Khoja et al., 2012, Chinen et al., 2014, Hofman et al., 2011a, De Giorgi et al., 2010, Ilie et al., 2014, Lecharpentier et al., 2011, Hofman et al., 2014, Laget et al., 2017).
In this study we used the ISET technology for the detection of CTC in cancer patients and as screening tool in patients with higher risk of malignancy, e.g. family history, smoking, age (>50 years). Here we provide evidence that screening for CTC allows for early detection of cancer. We further summarise follow-up results by CTC repeat tests of patients with detected CTC who were advised on integrative approaches including immune-stimulating nutritional therapy.
Materials and Methods
Aims
The observational study aimed to compare CTC count to cancer status and cancer risk, by monitoring treatment effectiveness in cancer patients and to screen for CTC in patients with a family history of cancer or clinical indication but no tumour mass.
Study design and patients
For this observational study, patients were recruited from two medical clinics in Melbourne, Australia, the National Institute of Integrative Medicine ‘NIIM’ Clinic, and the Eng Medical Centre, between Sept 2014 and Dec 2016. A number of physicians at the clinics with experience in the care of patients with or of risk of cancer, including two of the authors (PE, AS) with >30 years’ experience each, referred to the CTC test. CTC testing was performed to monitor treatment effectiveness in cancer patients, and for early detection screening in patients with an increased risk of cancer, including patients with a family history of cancer, smoking habits, long term oral contraceptive use or hormone replacement therapy in women, advanced age (>50 years) in men, or other medical indication, as per referral of the their doctor.
The study was approved by the NHMRC-endorsed NIIM Human Research Ethics Committee. Participating patients provided written informed consent. No individual patient data is divulged in this article. The study has been registered on the Australian New Zealand Clinical Trial Registry, ANZCTR 12614001143617.
Circulating Tumour Cell (CTC) detection
In this study we used the Isolation-by-Size-of-Epithelial-Tumour (ISET) methodology combining blood filtration and analysis by microscopy using standard histo-pathological criteria (Hofman et al., 2011b, Hofman et al., 2012). We followed standardised validated protocols described previously (Vona et al., 2000).
Briefly, the ISET method is a blood filtration-based approach, which enriches rare cells on a polycarbonate membrane with 8 micron pores. Almost all CTC are larger than the filter pores of 8 microns, including solid tumour cells of 11.7-23.8 microns, small-cell type cancers (e.g. small cell lung carcinoma of 7.2-10 microns) and blood type cancers (e.g. leukemia cells of 8.9-15.3 microns) (Paterlini-Bréchot, 2014, Harouaka et al., 2013, Laget et al., 2017). 10 mL of peripheral blood was collected in buffered EDTA, maintained at room temperature and processed within 2 hours of collection. Blood was then diluted 1:10 with buffer containing 0.175% saponin, 0.2% paraformaldehyde, 0.0372% EDTA, and 0.1% bovine serum albumin, shaken for 10 minutes at room temperature, and filtered with the ISET filtration blocks and device (Vona et al., 2000).
The dried filter membrane was stained with May-Gruenwald-Giemsa for cytological analysis.
A certified and experienced cancer cytologist, with international and Australian cytology certification CT (IAC) and CT (ASC) and more than 20 years’ experience, conducted the analysis using a Leica DMLB microscope with 63 x 10 magnification and standard histo-pathological criteria to identify the degree of malignancy.
Circulating malignant cells were defined by the presence of 4 of the following criteria: a) anisonucleosis (ratio >0.5), b) nuclei larger than 1-3 calibrated pore sizes (8 microns) of the membrane (i.e. >8-24 microns), c) irregular nuclear borders, d) high nuclei-cytoplasmic ratio, and/or e) presence of three-dimensional sheets. Cells displaying 1-3 criteria were defined as atypical cells with uncertain malignant potential. Circulating benign cells were characterized by the absence of these criteria (Hofman et al., 2012).
Images of CTC and atypical cells were taken with a digital Leica EC3 camera, and all images were reviewed independently by a second cytologist and any discrepancies discussed. All images were added to a library of digital images for future cross-reference.
Patient follow-up
Patients with detected CTC were advised on follow-up tests by the consulting doctor, including PET, CT, or MRI scans provided by accredited imaging institutions and hospitals.
In addition, cell surface cancer markers and receptor expression testing was performed on CTC cell culture from blood by an external specialised laboratory. Asymptomatic men with detected CTC, and Ki-67, prostate-specific-antigen (PSA) or androgen-receptor (AR) expression from CTC cell culture (Buhmeida et al., 2006), and PSA blood levels in the normal range, had a pelvic PET scan using Ga-68 PSMA (Gallium-68 Prostate-Specific-Membrane-Antigens) (Afshar-Oromieh et al., 2013). The Ga-PSMA-PET/CT scan is a highly sensitive test detecting lesions of ≥2.4 mm short axis diameter (Mottaghy et al., 2016, Verburg et al., 2016, Giesel et al., 2015). Asymptomatic women with detected CTC, and endocrine receptor (HER2) positive expression, had an MRI scan of the breast. Symptomatic patients had a scan relevant to the area of their symptoms. CTC testing was repeated within 3-9 months in patients with detected CTC, and yearly for patient without CTC but increased risk of cancer.
All patients with or without cancer diagnosis but with detected CTC were advised about integrative lifestyle changes and immune-stimulating therapies following evidence-based protocols including nutrients with anti-carcinogenic properties.
Analysis
Descriptive analysis was used to compare CTC count and cancer status or cancer risk at baseline, the primary outcome and observational component of the study. Simple comparative analyses were conducted for the subgroups of patients who undertook a repeat CTC test after a variety of treatments as intervention.
Results
Between Sept-2014 and Dec-2016 we undertook 600 CTC tests in 542 patients, including 50% screening requests (n=286 tests) of patients without cancer diagnosis but with risk factors. CTC were detected in all cancer patients (n=277, 100%), and in half of the asymptomatic patients screened (50%, n=132 out of 265 patients). A subgroup of patients with detected CTC underwent interventions (n=161). CTC repeat tests were done for 10% of patients with detected CTC (40 out of 409 patients, n=98 CTC tests). Figure 1 summarises the trial flow, following the TREND statement (Des Jarlais et al., 2004) and STROBE statement (Strengthening the Reporting of Observational Studies) (Vandenbroucke et al., 2007).
Figure 1.
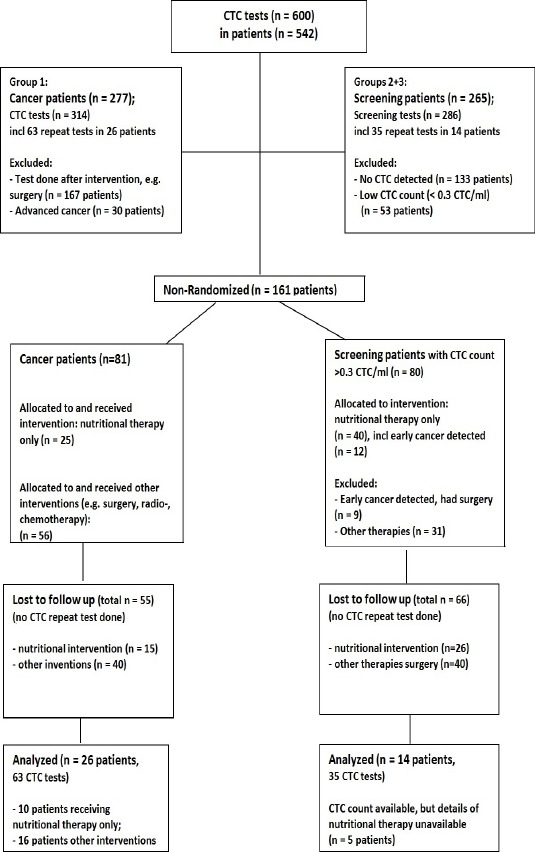
Trial Flow Chart. Cancer patients (group 1), asymptomatic patients (CTC screening, groups 2+3); CTC were detected in all cancer patients (group 1), and in 50% of asymptomatic patients (groups 2+3).
Cancer patients (group 1)
All patients with diagnosed cancer (group 1, Table 1) had a positive CTC count, detected with the ISET technology, including patients with solid tumours and blood type tumours (e.g. non-Hodgkin’s lymphoma, multiple myeloma). The CTC count ranged from 0.2 CTC/ml to 65.4 CTC/ml including single CTC and CTC clusters. CTC baseline count usually correlated to patient’s cancer status and symptoms, with higher CTC counts presented in more advanced cases. Our observational data derived from cancer patients suggests a count of less than 3 CTC/ml (0.1-2.9 CTC/ml) to be usually associated with mild risk of malignancy (Stage I), a count of 3-20 CTC/ml with moderate risk (Stage II and III), and >20 CTC/ml with high risk of malignancy (Stage IV), including metastasis, recurrence, and cancer progression. CTC count profile was similar in patients with different types of cancer. CTC testing was repeated after therapy within 3-9 months, usually in shorter intervals for higher CTC counts.
Table 1.
CTC Count by Type of Cancer (Group 1: Cancer Patients)
| CTC count1 | ||||
|---|---|---|---|---|
| Type of cancer | Number of patients | Stage 1 <3 CTC/ml | Stage 2-3 3-20 CTC/ml | Stage 4 >20 CTC/ml |
| N (% of type) | N (% of type) | N (% of type) | ||
| All | 277 | |||
| Breast | 81 | 52 (64) | 20 (25) | 9 (11) |
| Prostate | 69 | 54 (78) | 11(14) | 4 (5) |
| Colorectal, gastric | 37 | 26 (70) | 7 (19) | 4 (11) |
| Kidney, bladder | 19 | 11 | 6 | 2 |
| Blood type cancers: Lymphoma, NHL, HL, MCL, MM | 17 | 10 | 2 | 5 |
| Ovarian, endometrial, uterine, cervical | 15 | 10 | 4 | 1 |
| Lung | 6 | 2 | 1 | 3 |
| Melanoma | 9 | 9 | - | |
| Pancreatic | 3 | 2 | - | 1 |
| Thyroid | 5 | 5 | - | - |
| Other, e.g. tongue, brain, SCC | 16 | 9 | 6 | 1 |
CTC baseline count, CTC repeat tests of same patient not included in this table; Abbreviations, HL, Hodgkin’s lymphoma; MCL, mantle cell lymphoma; MM, multiple myeloma; NHL, Non-Hodgkin’s lymphoma; SCC, squamous cell carcinoma
Figure 2 illustrates examples of CTC detected with the ISET method using cyto-morphological criteria.
Figure 2.

Histo-Pathological/ Cyto-Morphological Detection of CTC Using the ISET Method. CTC are stained blue, filter pores of 8 microns appear black. Panel A: breast cancer, B: prostate cancer, C: colorectal cancer, D: renal/ bladder cancer
To monitor treatment effectiveness, CTC testing was repeated 3-4 weeks after conclusion of a treatment cycle around 5 months in 10% of cancer patients (n=26). Treatment could include surgery, chemotherapy, radiotherapy, hyperthermia, and nutritional therapies. CTC count correlated to patient’s cancer status (Table 1), with an increase in CTC count over time indicating cancer progression or metastases, and a decrease in CTC count over time indicating cancer remission (Table 2).
Table 2.
CTC Repeat Test Results of Cancer Patients Undergoing Treatment Incl. Surgery, Radio-, or FDA-Approved Chemotherapy (Group 1)
| Patient ID, age | Cancer type | Test ID | CTC test time points (A-D) | CTC count/ml | N months between CTC tests | Treatment details and comments |
|---|---|---|---|---|---|---|
| F1, 62 yrs | Colorectal | 292GL | A: Sep-15 | 0.4 | A: After surgery, radio, chemo | |
| 383GL | B: Jan-16 | 1.2 | 4 | |||
| 437GL | C: Mar-16 | 3.5 | 3 | C: Liver metastases detected | ||
| 595GL | D: Jul-16 | 1.9 | 4 | |||
| F2, 60 yrs | Colorectal | 338VD | A: Nov-15 | 0 | ||
| 405VD | B: Feb-16 | 0 | 3 | |||
| 592VD | C: Jul-16 | 21.1 | 5 | C: Lung metastases detected | ||
| F3, 41 yrs | Colorectal | 343NZ | A: Nov-15 | 2 | ||
| 609NZ | B: Jul-16 | 6.1 | 8 | B: Ongoing herbal therapy, details unknown | ||
| 782NZ | C: Dec-16 | 13.3 | 5 | |||
| F4, 33 yrs | Colorectal, sigmoid | 691GK | A: Oct-16 | 13.2 | ||
| 725GK | B: Nov-16 | 1 | 1 | B: After hyperthermia, IVC, IV-Curcumin | ||
| F5, 71 yrs | Breast | 171WS | A: May-15 | 0.6 | A: After surgery, radio | |
| 291WS | B: Sept-15 | 19.2 | 4 | B: Ongoing hormonal therapy, low Vit D level | ||
| 458WS | C: Apr-16 | 0.1 | 7 | C: After vitamin D, curcumin, relaxation | ||
| F6, 66 yrs | Breast | 296JWK | A: Sep-15 | 0.5 | A: After surgery | |
| 483JWK | B: Apr-16 | 2.5 | 7 | B: On chemo | ||
| F7, 65 yrs | Breast, bone, liver | 417SM | A: Feb-16 | 1.2 | A: Surgery 5 yrs ago | |
| 496SM | B:May-16 | 2.6 | 3 | B: Ongoing chemo | ||
| F8, 46 yrs | Breast | 255JB | A: Jul-15 | 0.1 | A: After surgery, chemo, radio a year earlier | |
| 497JB | B: May-16 | 6.6 | 10 | |||
| F9, 44 yrs | Breast | 153AB | A: May-15 | 2.6 | ||
| 390AB | B: Jan-16 | 0.7 | 8 | B: After surgery | ||
| F10, 42 yrs | Breast | 579DM | A: Jul-16 | 2.4 | ||
| 731DM | B: Nov-16 | 13 | 4 | B: After surgery, radio, chemo | ||
| F11, 63 yrs | Breast | 656DM | A: Aug-16 | 0.3 | 3 | |
| 763DM | B: Nov-16 | 3.2 | B: After radio, chemo, supplements | |||
| M12, 35 yrs | Gastric | 460MM | A: Apr-16 | 4.7 | A: Ongoing chemo | |
| 690MM | B: Oct-16 | 0.1 | 6 | B: Chemo + immunotherapy drug | ||
| F13, 57 yrs | Melanoma | 27EN | A: Nov-14 | 7.2 | A: Melanoma detected | |
| 449EN | B: Mar-16 | 1.1 | 16 | B: After surgery | ||
| M14, 51 yrs | Lung | 64SW | A: Nov-15 | 1.2 | 3 | A: After CTC screening 4 mm tumour detected, non-smoker, asbestos exposure |
| 427SW | B: Feb-16 | 0.9 | B: After surgery | |||
| F15, 48 yrs | Ovarian | 602GN | A: Jul-16 | 1.1 | 5 | |
| 775GN | B: Dec-16 | 1.1 | B: Ongoing chemo | |||
| M16, 65 yrs | Prostate | 534NM | A: May-16 | 6.2 | ||
| 757NM | B: Nov-16 | 0.8 | 6 | B: Sonotherapy, supplements |
F, female; M, male
Table 2 summarises the CTC count over time in cancer patients who underwent treatment other than nutritional therapies. In this group of patients, surgery treatment generally resulted in a decrease of CTC, standard chemo- and radiotherapy treatment did not.
Early detection screening (groups 2 + 3)
CTC screening tests were undertaken in mostly asymptomatic patients without diagnosed cancer but with increased cancer risk, including family history of cancer or advanced age (>50 years). No CTC were detected in half of the patients screened (n=132 out of 265, Figure 1), while in the other half the baseline CTC count ranged from 0.2-50 CTC/ml (mean=16 CTC/ml). For those patients with detected CTC (group 2), follow-up tests including scans and repeat CTC tests were scheduled within 0.5-10 months (mean = 3.5 months), and early cancerous lesions were detected by standard imaging technologies (scans) in about 20% (n=24 out of 133) of screened patients with a positive CTC count (Table 3).
Table 3.
Early Detection CTC Screening and Follow-Up Scans of Asymptomatic Patients without Detected Tumour at Time of CTC Testing (Group 2)
| Patient ID, age | CTC test method | Date CTC test | CTC number/ml | Receptor expression (%) | PSA ug/L | Date scan | N months between CTC and scan | Scan results/ Tumour detected | Results comments |
|---|---|---|---|---|---|---|---|---|---|
| F1, 37 yrs | Maintrac | Mar-15 | 2 | n/a | n/a | Apr-15 | 1 | Breast | MRI: 0.5 x 0.8 x 0.4 cm lesion right breast confirmed with FNA |
| F2, 37 yrs | ISET | May-15 | 0.8 | n/a | n/a | Jul-15 | 3 | Breast | CT scan: 0.7 x 0.6 x 0.7 cm tumour left breast, biopsy confirms neoplasm |
| F3, 44 yrs | ISET | May-16 | 101 | n/a | n/a | May-16 | 0.2 | Ovarian | Ultrasound: had ovarian cystectomy, ISET-CTC test after surgery: 0 CTC/ml |
| F4, 57 yrs | ISET | Nov-14 | 7.2 | n/a | n/a | Dec-14 | 1 | Melanoma | Biopsy, surgery |
| M5, 50 yrs | ISET | Dec-14 | 1.2 | n/a | n/a | Dec-14 | 0.5 | Lung | PET scan: 4mm right upper pulmonary tumour with radiotracer (FDG) uptake; non-smoker, non-smoker, asbestos exposure during renovations |
| M6, 54 yrs | ISET | Jun-16 | 7.2 | n/a | n/a | Jul-16 | 1 | Kidney | Nephrectomy in 12/16; CTC repeat after surgery 1/2017 1 CTC/ml |
| F7, 42 yrs | ISET | Jun-16 | 8.1 | n/a | n/a | Jun-16 | 0.5 | Lung, Mesothelioma | Symptoms at time of CTC test: Abdominal pain, pelvic fluid, bloating; Mesothelioma, non-smoker |
| M8a, 59 yrs M8b |
ISET; Maintrac |
Dec-14; Mar-15 |
2.6; 33.5 |
Ki67=19.3 |
1.44 |
Jun-15 |
6 |
Prostate | PSMA-PET: very mildly increased activity in the right side of the prostate |
| M9, 55 yrs | Maintrac | Oct-15 | 0.5 | Ki67=78.9 AR=95.2; PSA=68.4 |
0.87 | Nov-15 | 1 | Prostate | PSMA-PET: low volume, low grade carcinoma |
| M10, 73 yrs | Maintrac | Sep-15 | 11 | Ki67=77.1; PSA=31.8 |
1.5 | Oct-15 | 1 | Prostate | PSMA-PET: Moderate uptake right lobe, low grade left lobe |
| M11, 58 yrs | Maintrac | Sep-15 | 10 | Ki67=85.7; PSA=50 |
4.4 | Oct-15 | 1 | Prostate | PSMA-PET: low volume low Gleason score prostatic malignancy; minimally increased uptake base of prostate right posterior, bilaterally mid-prostate anterior right, mid left, apex right |
| M12a, 71 yrs M12b |
ISET; Maintrac |
Feb-15; Oct-15 |
3.1; 4.5 |
Ki67=74.1 PSA=63.5 AR=51.8 |
1.97 |
Oct-15 |
8 |
Prostate |
PSMA-PET: moderate grade prostate carcinoma, central aspect of the left lobe; linear low grade uptake in oesophagus most likely physiologic/salivary |
| M13a, 66 yrs | ISET; | Sep-15; | 1.1; | 0.33 | |||||
| M13b | Maintrac | Oct-15 | 3.5 | Ki67=83.3; PSA=59; AR=71 |
Oct-15 | 1 | Prostate | PSMA-PET: low grade prostate cancer | |
| M14a, 76 yrs | ISET; | Jan-15; | 4.9; | ||||||
| M14b | Maintrac | Sep-15 | 9 | Ki67=61.8; PSA=69; AR=65.2 |
2.19 | Oct-15 | 10 | Prostate | PSMA-PET: mild uptake in both lobes; likely to be true positive |
| M15, 65 yrs | Maintrac | Oct-15 | 5 | PSA=40 AR=40 |
2.74 | Nov-15 | 1 | Prostate | PSMA-PET: very low volume low grade prostate cancer |
| M16a, 53 yrs | ISET; | Feb-15; | |||||||
| M16b | Maintrac | Jun-15 | 4; 9 | Ki67=67.4 | 1.95 | Nov-15 | 10 | Prostate | MRI normal, but PSMA-PET abnormal |
| M17a, 69 yrs | ISET; | Sep-15; | 0.5 + inflammation; | 3.7 | PSMA-PET: no significant accumulation, no evidence of nodal or distant metastases; marked prostatomegaly, but no tumour; ISET-CTC: inflammation, atypical cells due to infection; | ||||
| M17b | Maintrac | Oct-15 | 3 | PSA=100; AR=46.2; Ki67=60 |
Nov-15 | 2.5 | Prostate – no uptake | Maintrac-CTC does not distinguish between CTC and atypical inflammatory cells; | |
| M18, 65 yrs | Maintrac | Oct-15 | 12 | Ki67=53.8; PSA=66.7; AR=53.8 |
14.2 | Sep-15 | -1 (MRI before CTC) | Prostate | MRI prostate: multiple lesions (1.7 cm; 0.7 cm); had surgery, CTC count dropped to M: 4.7 CTC/ml |
| M19, 71 yrs | Maintrac | Feb-16 | 2.5 | 1.63 | Apr-16 | 2.5 | Prostate | PSMA-PET: low grade uptake right prostatic base | |
| M20a, 68 yrs | Maintrac | Dec-15; Feb-16 |
6.5; 7.5 | Ki67=72.6 | <0.01 | Jan-16 | 1 | Prostate | Had bladder cancer in 2014; prostectomy Jan 16; minimal uptake non-specific; NIIM CTC + lipoblast masses |
| M20b | ISET | May-16 | 2.8 | ||||||
| M21b | Maintrac ISET |
Dec-15 Apr-16 |
3 5.4 |
Ki67=50; AR=45.9 |
1.21 | Mar-16 | 7 | Prostate | PSMA-PET: possible low-grade prostate cancer in left posterior peripheral zone, more concerning uptake in right hepatic lobe |
| M22a, 76 yrs M22b |
ISET; Maintrac |
Feb-16; Apr-16 |
0.7 atypical inflammatory cells; 2 | PSA=79; AR=88.6 |
normal normal |
May-16 | 3 | Prostatitis | PSMA=PET CT: mild prostatitis; ISET-CTC identified inflammatory condition, no CTC detected; Maintrac-CTC does not distinguish between CTC and atypical inflammatory cells |
| M23, 49 yrs | ISET; Maintrac |
May-16 May-16 |
65.4; 13 |
AR=62; PSA=0 |
normal | Apr-16 | 1 | Prostate | PSMA-PET: moderate uptake |
| M24, 66 yrs | ISET; Maintrac |
May-16 | 10.7; 11 |
PSA=79; AR=73; |
high normal | Jun-16 | 1 | Prostate | PSMA-PET: low to moderate uptake |
Early detection CTC screening was performed in patients with an increased risk of cancer, including those with a family history of cancer, smoking habits, long term oral contraceptive use or hormone replacement therapy in women, advanced age (>50 years) in men, or other medical indication, as per referral of the their doctor; ISET, ISET technology (Rarecells, France, www.rarecells.com); Maintrac technology (Germany, www.maintrac.com): Receptor expression and EpCAM marker based CTC testing. In our experience, the CTC count by Maintrac correlates to the ISET CTC count by a factor of 100. For comparison to ISET CTC counts Maintrac CTC counts have been divided by 100; Abbreviations: F, female; M, male, AR, androgen receptor; Ki67, the Ki-67 protein is a cellular marker for cell proliferation; PSA, prostate specific antigen; PSMA, prostate specific membrane antigen; FNA, fine needle aspiration; PET scan, positron emission tomography scan; n/a, not applicable
In up to 50% of male patients with normal PSA (prostate specific antigen) levels but with detected CTC, PET scans using PSMA (Ga-68 prostate-specific-membrane-antigens) revealed increased uptake in the prostate, which is indicative of early prostate cancer. In addition, early breast cancer, melanoma, ovarian, lung or renal cancer was detected during the study period in a small number of asymptomatic women and men (n=7) who had undergone the CTC screening test (Table 3).
Integrative approaches including nutritional therapies
A subgroup of patients with detected CTC was advised on lifestyle (e.g. diet, exercise), and evidence-based immune-boosting and anti-carcinogenic nutritional therapy by the consulting doctor. Treatment was tailored towards increasing natural killer cell count, inhibition of angiogenesis and metastasis. Supplements included curcumin, green tea, garlic extract, vitamin D, grape seed, lycopene, citrus pectin, medicinal mushroom extract, black cumin seed, artemisinin, and other immune stimulanting nutrients with anti-carcinogenic properties (Table 4).
Table 4.
Integrative Nutritional Treatment of Patients with Detected CTC (Group 1 and Group 3)
| Patient ID; (gender, age) | Group | Curcumin | Green tea | Garlic | Vit D | Grape Seed | Lycopene | Citrus Pectin | Mushroom extract | Nigella sativa | Artemisinin | Others (immune stimulants) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Group 1: Cancer patients with detected CTC, who did not undergo surgery, chemo- or radiotherapy during the intervention | ||||||||||||
| C10_TCC | 1 | √ | √ | √ | √ | √ | Vit E, Se, NK cell activator, reveratrol, astragalus | |||||
| C11_SCC (F, 68yrs) | 1 | √ | NK Cell activator, astragalus | |||||||||
| CJ12_prostate (M, 67 yrs) | 1 | √ | √ | √ | √ | √ | √ | √ | √ | Prostate formula: saw palmetto, lycopene, boswellia, pumpkin seed oil, boron, fish oil, Vit E, Se | ||
| C13_prostate (M, 71 yrs) | 1 | √ | √ | √ | √ | IVC, resveratrol, liver tonic, soy, Ca, Vit K2, phosphatidylserine, bromelain, salvestrol, p53, fish oil | ||||||
| CJ16_NHL & prostate (M, 65 yrs) | 1 | √ | √ | √ | √ | √ | Pomegranate, fish oil, Ca, Vit K2, | |||||
| CJ26_bladder (M, 53 yrs) | 1 | √ | √ | √ | √ | √ | Vit A | √ | √ | √ | NK cell activator, probiotic, salvestrol, astaxanthin, NAC | |
| J52_prostate, & bladder (M, 57 yrs) | 1 | √ | √ | √ | √ | √ | mistletoe, quercetin, bromelain, Se, soy, fucoidan (brown algae) | |||||
| C73_prostate (M, 49 yrs) | √ | Mg, Vit B12 | ||||||||||
| C100_breast (F, 56 yrs) | 1 | √ | √ | √ | √ | Fish oil, pomegranate, rosemary | ||||||
| Group 3: Asymptomatic patients without tumour but detected CTC | ||||||||||||
| Pt1 (F 51 yrs) | 3 | √ | √ | √ | √ | √ | √ | astragalus, probiotic, Vit C, boswellia, soy, liver tonics, NAC, Vit E, Se, Ca, Vit K2 | ||||
| Pt 2 (M, 50 yrs) | √ | Mg, Vit B12 | ||||||||||
| Pt3 (F 63yrs) | 3 | √ | √ | √ | √ | √ | √ | resveratrol, Vit C, NAC, Vit E, Se, Ca, Vit K2 | ||||
| Pt4 (F 56 yrs) | 3 | √ | √ | √ | √ | √ | broccoli, Vit A, CoQ10, NAC | |||||
| Pt5 (F 55 yrs) | 3 | √ | √ | √ | NK cell activator, astragalus, Se, Vit E, Se, Ca, Vit K2 | |||||||
| Pt7 (M 71 yrs) | 3 | √ | √ | √ | √ | √ | √ | √ | √ | Vit K2, reveratrol, broccoli, NAC, milk thistle, Vit C, Vit B12 | ||
| Pt9 (M, 66 yrs) | 3 | √ | √ | √ | √ | √ | √ | NK cell activator, salvestrol, glutathione, chlorophyll, broccoli, NAC, fish oil, Vit E, Se | ||||
| Pt10 (F, 63 yrs) | 3 | √ | √ | √ | √ | √ | √ | Nk cell activator | ||||
| Pt14 (F, 49 yrs) | 3 | √ | √ | √ | √ | resveratrol, salvestrol, broccoli, pomegranate, Vit B12, NAC, fish oil, Vit E, Se | ||||||
C, cancer; S, screening; F, female; M, male; Ca, Calcium; NAC, N-acetylcysteine; NK cell, natural killer cell; NK cell activator contains enzymatically modified rice bran; Pt, patient; Se, selenium; Vit, vitamin
Treatment effectiveness of evidence-based nutritional immune-stimulating and anti-carcinogenic therapy was assessed by repeat CTC testing, available for cancer patients with mild disease, who had not undergone surgery, chemo- or radiotherapy for a variety of reasons (group 1, n=9, Figure 3a), and asymptomatic patients without detected tumour but positive CTC count at baseline (n=14, group 3, Figure 3b). In all of these patients, CTC counts decreased over time (1-15 months) with integrative nutritional therapy (Figure 3). No adverse effects were reported.
Figure 3.
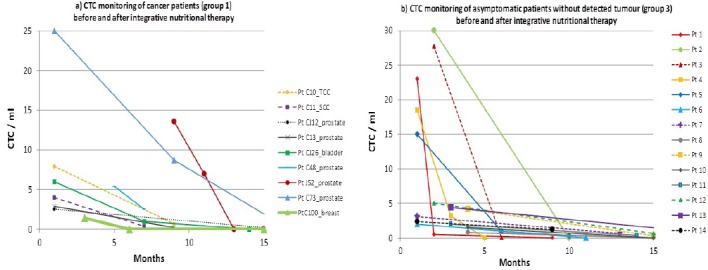
CTC Monitoring of a) cancer patients (group1) and b) asymptomatic patients without detectable tumour (group3) before and after integrative therapies including immune-stimulating nutrients. Cancer patients (group 1) with mild disease did not undergo surgery, chemo- or radiotherapy due to variety of reasons.
Discussion
Our study suggests testing for Circulating Tumour Cells (CTC) to be a useful screening tool for the early detection of cancer in patients with a higher risk profile, including those with a family history of cancer. CTC testing and CTC count can also assists with monitoring of treatment effectiveness in cancer patients. A positive CTC count was associated with cancer risk, whereby a low CTC count (< 3 CTC/ml) was correlated with mild malignant potential, 3-20 CTC/ml with moderate malignant potential, and a higher CTC count (>20 CTC/ml) with higher risk of malignancy, recurrence and metastasis, consistent with previous reports (Cristofanilli et al., 2004; Ilie et al., 2014, Hayes et al., 2006). In addition to the CTC number, the type of cells, single cells or clusters, provide valuable insights into the cancer prognosis (Ilie et al., 2014; Wang et al., 2017). In this study we employed the ISET technology (Rarecells) for CTC detection, which provides the advantage of a direct identification of malignant cells by cyto-morphological criteria (Vona et al., 2000; Laget et al., 2017), permitting distinction between precursor and malignant single cells and clusters, as well as reactive inflammatory atypical cells (Farace et al., 2011; Hofman et al., 2012; Paterlini-Brechot and Benali, 2007).
In our study, screening for CTC in asymptomatic individuals allowed the detection of early cancer, in about 20% of patients presenting with CTC. Importantly, in up to half of the men with detected CTC (25% of all men screened), but with normal PSA levels, subsequent positive PSMA-PET scans revealed early prostate cancer. This suggests CTC screening to be a more reliable measure for the detection of early prostate cancer than standard PSA testing (Thompson et al., 2004). In addition, early breast cancer, melanoma, ovarian, lung and renal cancer was detected in a small number of asymptomatic women and men with a positive CTC count. Early detection of cancer is associated with a greater range of treatment options and better prognosis (Cristofanilli et al., 2004; Hayes et al., 2006; Tol et al., 2010).
A strength of our study was to compare the CTC count to cancer status and cancer risk in a large cohort of 542 patients. While CTC repeat test results after treatment were available in only a small subgroup of patients (40 out of 409 patients, 10%, with detected CTC), early results provide a trend towards treatment effectiveness of different types of interventions. However, statistical analysis in this patient cohort was not feasible due the small sample size and variety of treatments, therefore limiting generalisability about effectiveness of interventions.
Our study provided early evidence for integrative nutritional therapy to have the potential to lower CTC count, which in turn is associated with a lower risk of malignancy. Nutritional therapy was highly tolerable, and tailored towards increasing natural killer cell count, enhancing apoptosis of cancer cells, inhibition of angiogenesis and metastasis.
Natural Killer (NK) cells are an important gatekeepers stalling the growth of atypical cells, including cancer cells. Low NK cell levels have been associated with an increased risk of death in breast cancer (Eichbaum et al., 2006). Additionally, reduced NK cell activity increased the risk of metastasis by 350% during a 31-month period (Koda et al., 1996).
Garlic, available in form of garlic extract or garlic powder, has shown to increase natural killer cells (Lamm and Riggs, 2001). Other anti-carcinogenic properties of garlic include reduced infection-induced carcinogenesis, and the induction of apoptosis (Kyo et al., 1998; Thomson and Ali, 2003).
Other nutrients with anti-carcinogenic properties include curcumin, green tea, grape seed extract, black cumin seed, artemisinin, modified citrus pectin, and mushroom extract.
Curcumin enhances apoptotic death, inhibits deregulated cellular proliferation, dedifferentiation and progression towards the neoplastic phenotype by altering key signaling molecules required for cell cycle progression, in addition to inhibiting H-Ras oncogene expression (Sa and Das, 2008; Limtrakul et al., 2001; Kim et al., 2001).
Green tea with its polyphenols has been shown to inhibit several pathways and enzymes engaged in carcinogenesis, including the nuclear factor-κB (NF-κB), epidermal growth factor receptor (EGFR), insulin-like growth factor (IGF)-I, urokinase-plasminogen activator (uPA), matrix metalloproteinases (MMPs) involved in oncogene expression, and proteasome activities, and contributing to apoptosis and cell cycle arrest (Jankun et al., 1997, Khan and Mukhtar, 2008).
Grape seed extract inhibits advanced tumour growth and angiogenesis and upregulates insulin-like growth factor binding protein (Singh et al., 2004), and can induce apoptosis and cell cycle arrest (Kaur et al., 2009).
Black cumin seed (Nigella sativa), with its main active ingredient thymoquinone, has shown promise in inducing tumour cell death, and inhibiting proliferation, angiogenesis, invasion and metastasis (Randhawa and Alghamdi, 2011). Artemisinin triggers apoptosis in human cancer cells (Singh and Lai, 2004).
Modified citrus pectin, containing the main active ingredient galectin-3, has numerous anti-metastatic properties through anti-adhesion and apoptosis-promotion, and has shown promise in several clinical studies by halting cancer progression (Glinsky and Raz, 2009; Azémar et al., 2007).
Medicinal mushroom extracts, including species of Auricularia, Flammulina, Ganoderma, Grifola, Hericium, Lentinus (Lentinula), Pleurotus, Trametes (Coriolus), Schizophyllum, and Tremella mushrooms, contain polysaccharides or polysaccharide–protein complexes, which enhance innate and cell-mediated immune responses, and inhibit proteins and enzymes involved in carcinogenesis, including NF-κB, protein-kinases, aromatase and sulfatase, and cyclooxygenase (Zaidman et al., 2005).
Additionally, a number of nutrients are essential for an active healthy immune system, including vitamin D, which has also been shown to play a role in anti-carcinogenesis.
Calcitriol derived from Vitamin D decreases the expression of aromatase, the enzyme that catalyses estrogen synthesis in breast cancer, both by a direct transcriptional repression and indirectly by reducing inflammatory prostaglandins (Krishnan and Feldman, 2011).
Vitamin D, in addition to calcium, magnesium, Vitamin K, and boron, is also important for bone integrity (Schwarz et al., 2013), with bone always being affected in advanced breast and prostate cancer (Mundy, 2002; Lappe et al., 2007).
Lycopene, abundant particularly in tomatoes, has shown promise particularly in prostate cancer (van Breemen and Pajkovic, 2008; Hadley et al., 2002).
In conclusion, here we provide evidence that screening for Circulating Tumour Cells (CTC) allows detection of early cancer, while CTC monitoring over time allows assessment of treatment effectiveness, with higher CTC counts being associated with higher risk of malignancy. Our study suggests CTC count to be a more reliable predictor of early prostate cancer than standard testing of PSA levels, identifying early prostate cancer confirmed by PSMA-PET scan in 50% of asymptomatic men with detected CTC. Furthermore, our study provides evidence that a combination of immune-stimulating nutritional supplements can reduce CTC count, and therefore risk of malignancy. Nutrients with anti-carcinogenic properties include curcumin, garlic, green tea, grape seed, black cumin seed, artemisinin, modified citrus pectin, and medicinal mushroom extract.
List of abbreviations
CTC, Circulating Tumour Cells
EDTA, Ethylene Diamine Tetra Acetic Acid
EpCAM, Epithelial Cell Adhesion Molecule
ISET, Isolation by Size of Epithelial Tumours
PET, Positron Emission Tomography
PSA, Prostate Specific Antigen
PSMA, Prostate Specific Membrane Antigen
Authors’ contributions
All authors conceived and designed the study. NIIM Director AS introduced CTC testing to the institute, and physicians PE and AS provided patients, patient data, and treatment plans for the study. KR established and oversaw ISET-CTC testing at the NIIM lab, collated and analysed the data, and wrote the manuscript, with contributions from co-authors. All authors read and approved the final version.
Acknowledgements
We are grateful to the team of technical and research assistants who made CTC testing at NIIM possible, including Nikolaj Travica, phlebotomist and research assistant, Viktor Svarcs, chief cancer cytologist, Renee DeBoer and Anna Cabrera, technical assistants. We would also like to thank the cytologist Adela Cretoiu, who helped establish the ISET-CTC technology at NIIM. We gratefully acknowledge Dr John Piesse, who also provided patients and patient data, and Dr Peter Fakler for valuable feedback on the manuscript.
References
- Afshar-Oromieh A, Malcher A, Eder M, et al. PET imaging with a [68Ga] gallium-labelled PSMA ligand for the diagnosis of prostate cancer: biodistribution in humans and first evaluation of tumour lesions. Eur J Nucl Med Mol Imaging. 2013;40:486–95. doi: 10.1007/s00259-012-2298-2. [DOI] [PubMed] [Google Scholar]
- Azémar M, Hildenbrand B, Haering B, Heim ME, Unger C. Clinical benefit in patients with advanced solid tumors treated with modified citrus pectin: a prospective pilot study. Clinical medicine insights Oncology. 2007;1:73. [Google Scholar]
- Barriere G, Fici P, Gallerani G, et al. Circulating tumor cells and epithelial, mesenchymal and stemness markers: characterization of cell subpopulations. Ann Transl Med. 2014;2:109. doi: 10.3978/j.issn.2305-5839.2014.10.04. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buhmeida A, Pyrhönen S, Laato M, Collan Y. Prognostic factors in prostate cancer. Diagn Pathol. 2006;1:4. doi: 10.1186/1746-1596-1-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chinen L, Mello C, Abdallah E, et al. Isolation, detection, and immunomorphological characterization of circulating tumor cells (CTCs) from patients with different types of sarcoma using isolation by size of tumor cells: a window on sarcoma-cell invasion. Onco Targets Ther. 2014;7:1609–17. doi: 10.2147/OTT.S62349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cristofanilli M, Budd GT, Ellis MJ, et al. Circulating tumor cells, disease progression, and survival in metastatic breast cancer. N Engl J Med. 2004;351:781–91. doi: 10.1056/NEJMoa040766. [DOI] [PubMed] [Google Scholar]
- De Giorgi V, Pinzani P, Salvianti F. Circulating benign nevus cells detected by ISET technique: warning for melanoma molecular diagnosis. Arch Dermatol. 2010;146:1120–4. doi: 10.1001/archdermatol.2010.264. [DOI] [PubMed] [Google Scholar]
- Des Jarlais DC, Lyles Crepaz N. Improving the reporting quality of nonrandomized evaluations of behavioral and public health interventions: the TREND statement. Am J Pub Health. 2004;94:361–6. doi: 10.2105/ajph.94.3.361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eichbaum MH, Kaltwasser M, Bruckner T, et al. Prognostic factors for patients with liver metastases from breast cancer. Breast Cancer Res Treat. 2006;96:53–62. doi: 10.1007/s10549-005-9039-1. [DOI] [PubMed] [Google Scholar]
- Farace F, Massard C, Vimond N, et al. A direct comparison of CellSearch and ISET for circulating tumour-cell detection in patients with metastatic carcinomas. Br J Cancer. 2011;105:847–53. doi: 10.1038/bjc.2011.294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Garcia JA, Rosenberg JE, Weinberg V, et al. Evaluation and significance of circulating epithelial cells in patients with hormone-refractory prostate cancer. BJU Int. 2007;99:519–24. doi: 10.1111/j.1464-410X.2007.06659.x. [DOI] [PubMed] [Google Scholar]
- Giesel FL, Fiedler H, Stefanova M, et al. PSMA PET/CT with Glu-urea-Lys-(Ahx)-[68Ga (HBED-CC)] versus 3D CT volumetric lymph node assessment in recurrent prostate cancer. Eur J Nucl Med Mol Imaging. 2015;42:1794–1800. doi: 10.1007/s00259-015-3106-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Glinsky VV, Raz A. Modified citrus pectin anti-metastatic properties: one bullet, multiple targets. Carbohydr Res. 2009;344:1788–91. doi: 10.1016/j.carres.2008.08.038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hadley CW, Miller EC, Schwartz SJ, Clinton SK. Tomatoes, lycopene, and prostate cancer: progress and promise. Exp Biol Med. 2002;227:869–80. doi: 10.1177/153537020222701006. [DOI] [PubMed] [Google Scholar]
- Harouaka RA, Nisic M, Zheng S-Y. Circulating tumor cell enrichment based on physical properties. J Lab Autom. 2013;18:455–68. doi: 10.1177/2211068213494391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hayes DF, Cristofanilli M, Budd GT, et al. Circulating tumor cells at each follow-up time point during therapy of metastatic breast cancer patients predict progression-free and overall survival. Clin Cancer Res. 2006;12:4218–24. doi: 10.1158/1078-0432.CCR-05-2821. [DOI] [PubMed] [Google Scholar]
- Hofman V, Ilie M, Long E, et al. Detection of circulating tumor cells from lung cancer patients in the era of targeted therapy: promises, drawbacks and pitfalls. Curr Mol Med. 2014;14:440–56. doi: 10.2174/1566524014666140414205455. [DOI] [PubMed] [Google Scholar]
- Hofman V, Ilie MI, Long E, et al. Detection of circulating tumor cells as a prognostic factor in patients undergoing radical surgery for non-small-cell lung carcinoma: comparison of the efficacy of the cell search assay and the isolation by size of epithelial tumor cell method. Int J Cancer. 2011a;129:1651–60. doi: 10.1002/ijc.25819. [DOI] [PubMed] [Google Scholar]
- Hofman V, Long E, Ilie M, et al. Morphological analysis of circulating tumour cells in patients undergoing surgery for non-small cell lung carcinoma using the isolation by size of epithelial tumour cell (ISET) method. Cytopathology. 2012;23:30–8. doi: 10.1111/j.1365-2303.2010.00835.x. [DOI] [PubMed] [Google Scholar]
- Hofman VJ, Ilie MI, Bonnetaud C, et al. Cytopathologic detection of circulating tumor cells using the isolation by size of epithelial tumor cell method: promises and pitfalls. Am J Clin Pathol. 2011b;135:146–56. doi: 10.1309/AJCP9X8OZBEIQVVI. [DOI] [PubMed] [Google Scholar]
- Ilie M, Hofman V, Long-Mira E, et al. “Sentinel” circulating tumor cells allow early diagnosis of lung cancer in patients with chronic obstructive pulmonary disease. PLoS One. 2014;9:e111597. doi: 10.1371/journal.pone.0111597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jankun J, Selman SH, Swiercz R, Skrzypczak-Jankun E. Why drinking green tea could prevent cancer. Nature. 1997;387:561. doi: 10.1038/42381. [DOI] [PubMed] [Google Scholar]
- Kaur M, Agarwal C, Agarwal R. Anticancer and cancer chemopreventive potential of grape seed extract and other grape-based products. J Nutr. 2009;139:1806–12. doi: 10.3945/jn.109.106864. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khan N, Mukhtar H. Multitargeted therapy of cancer by green tea polyphenols. Cancer Lett. 2008;269:269–80. doi: 10.1016/j.canlet.2008.04.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khoja L, Backen A, Sloane R, et al. A pilot study to explore circulating tumour cells in pancreatic cancer as a novel biomarker. Br J Cancer. 2012;106:508–16. doi: 10.1038/bjc.2011.545. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khoja L, Shenjere P, Hodgson C, et al. Prevalence and heterogeneity of circulating tumour cells in metastatic cutaneous melanoma. Melanoma Res. 2014;24:40–6. doi: 10.1097/CMR.0000000000000025. [DOI] [PubMed] [Google Scholar]
- Kim M-S, Kang H-J, Moon A. Inhibition of invasion and induction of apoptosis by curcumin in H-ras-transformed MCF10A human breast epithelial cells. Arch Pharm Res. 2001;24:349–54. doi: 10.1007/BF02975105. [DOI] [PubMed] [Google Scholar]
- Koda K, Saito N, Takiguchi N, e al. Preoperative natural killer cell activity: correlation with distant metastases in curatively research colorectal carcinomas. Int J Surg. 1996;82:190–3. [PubMed] [Google Scholar]
- Krebs MG, Hou JM, Sloane R, et al. Analysis of circulating tumor cells in patients with non-small cell lung cancer using epithelial marker-dependent and -independent approaches. J Thorac Oncol. 2012;7:306–15. doi: 10.1097/JTO.0b013e31823c5c16. [DOI] [PubMed] [Google Scholar]
- Krishnan AV, Feldman D. Mechanisms of the anti-cancer and anti-inflammatory actions of vitamin D. Annu Rev Pharmacol Toxicol. 2011;51:311–36. doi: 10.1146/annurev-pharmtox-010510-100611. [DOI] [PubMed] [Google Scholar]
- Kyo E, Uda N, Suzuki A, et al. Immunomodulation and antitumor activities of aged garlic extract. Phytomedicine. 1998;5:259–67. doi: 10.1016/S0944-7113(98)80064-0. [DOI] [PubMed] [Google Scholar]
- Laget S, Broncy L, Hormigos K, et al. Technical insights into highly sensitive isolation and molecular characterization of fixed and live circulating tumor cells for early detection of tumor invasion. PLoS One. 2017;12:e0169427. doi: 10.1371/journal.pone.0169427. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lamm DL, Riggs DR. Enhanced immunocompetence by garlic: role in bladder cancer and other malignancies. J Nutr. 2001;131:1067–70. doi: 10.1093/jn/131.3.1067S. [DOI] [PubMed] [Google Scholar]
- Lappe JM, Travers-Gustafson D, Davies KM, Recker RR, Heaney RP. Vitamin D and calcium supplementation reduces cancer risk: results of a randomized trial. Am J Clin Nutr. 2007;85:1586–91. doi: 10.1093/ajcn/85.6.1586. [DOI] [PubMed] [Google Scholar]
- Lecharpentier A, Vielh P, Perez-Moreno P, et al. Detection of circulating tumour cells with a hybrid (epithelial/mesenchymal) phenotype in patients with metastatic non-small cell lung cancer. Br J Cancer. 2011;105:1338–41. doi: 10.1038/bjc.2011.405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Limtrakul P-N, Anuchapreeda S, Lipigorngoson S, Dunn FW. Inhibition of carcinogen induced c-Ha-ras and c-fos proto-oncogenes expression by dietary curcumin. BMC Cancer. 2001;1:1. doi: 10.1186/1471-2407-1-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mottaghy FM, Behrendt FF, Verburg FA. 68-Ga-PSMA-HBED-CC Pet/CT: where molecular imaging has an edge over morphological imaging. Eur J Nucl Med Mol Imaging. 2016;43:394–6. doi: 10.1007/s00259-015-3212-5. [DOI] [PubMed] [Google Scholar]
- Mundy GR. Metastasis: Metastasis to bone: causes, consequences and therapeutic opportunities. Nat Rev Cancer. 2002;2:584–93. doi: 10.1038/nrc867. [DOI] [PubMed] [Google Scholar]
- Pachmann UA, Hekimian K, Carl S, et al. Comparing sequential steps for detection of circulating tumor cells: more specific or just less sensitive? WebMedCentral. 2011 WMC001490. [Google Scholar]
- Paterlini-Bréchot P. Circulating tumor cells: Who is the killer? Cancer Microenviron. 2014;7:161–76. doi: 10.1007/s12307-014-0164-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Paterlini-Brechot P, Benali NL. Circulating tumor cells (CTC) detection: clinical impact and future directions. Cancer Lett. 2007;253:180–204. doi: 10.1016/j.canlet.2006.12.014. [DOI] [PubMed] [Google Scholar]
- Randhawa MA, Alghamdi MS. Anticancer activity of Nigella sativa (black seed)-a review. Am J Chin Med. 2011;39:1075–91. doi: 10.1142/S0192415X1100941X. [DOI] [PubMed] [Google Scholar]
- Sa G, Das T. Anti cancer effects of curcumin: cycle of life and death. Cell Div. 2008;3:1. doi: 10.1186/1747-1028-3-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwarz EC, Qu B, Hoth M. Calcium, cancer and killing: the role of calcium in killing cancer cells by cytotoxic T lymphocytes and natural killer cells. Biochim Biophys Acta. 2013;1833:1603–11. doi: 10.1016/j.bbamcr.2012.11.016. [DOI] [PubMed] [Google Scholar]
- Singh NP, Lai HC. Artemisinin induces apoptosis in human cancer cells. Anticancer Res. 2004;24:2277–80. [PubMed] [Google Scholar]
- Singh RP, Tyagi AK, Dhanalakshmi S, Agarwal R, Agarwal C. Grape seed extract inhibits advanced human prostate tumor growth and angiogenesis and upregulates insulin-like growth factor binding protein-3. Int J Cancer. 2004;108:733–40. doi: 10.1002/ijc.11620. [DOI] [PubMed] [Google Scholar]
- Thompson IM, Pauler DK, Goodman PJ, et al. Prevalence of prostate cancer among men with a prostate-specific antigen level≤4.0 ng per milliliter. N Engl J Med. 2004;350:2239–46. doi: 10.1056/NEJMoa031918. [DOI] [PubMed] [Google Scholar]
- Thomson M, Ali M. Garlic [Allium sativum]: a review of its potential use as an anti-cancer agent. Curr Cancer Drug Targets. 2003;3:67–81. doi: 10.2174/1568009033333736. [DOI] [PubMed] [Google Scholar]
- Tol J, Koopman M, Miller M, et al. Circulating tumour cells early predict progression-free and overall survival in advanced colorectal cancer patients treated with chemotherapy and targeted agents. Ann Oncol. 2010;21:1006–12. doi: 10.1093/annonc/mdp463. [DOI] [PubMed] [Google Scholar]
- Van Breemen RB, Pajkovic N. Multitargeted therapy of cancer by lycopene. Cancer Lett. 2008;269:339–51. doi: 10.1016/j.canlet.2008.05.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vandenbroucke JP, Von Elm E, Altman DG, et al. Strengthening the reporting of observational studies in epidemiology (STROBE): explanation and elaboration. PLoS Med. 2007;4:e297. doi: 10.1371/journal.pmed.0040297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Verburg FA, Pfister D, Heidenreich A, et al. Extent of disease in recurrent prostate cancer determined by [68Ga] PSMA-HBED-CC PET/CT in relation to PSA levels, PSA doubling time and Gleason score. Eur J Nucl Med Mol Imaging. 2016;43:397–403. doi: 10.1007/s00259-015-3240-1. [DOI] [PubMed] [Google Scholar]
- Vona G, Estepa L, Béroud C, et al. Impact of cytomorphological detection of circulating tumor cells in patients with liver cancer. Hepatology. 2004;39:792–7. doi: 10.1002/hep.20091. [DOI] [PubMed] [Google Scholar]
- Vona G, Sabile A, Louha M, et al. Isolation by size of epithelial tumor cells : a new method for the immunomorphological and molecular characterization of circulatingtumor cells. Am J Pathol. 2000;156:57–63. doi: 10.1016/S0002-9440(10)64706-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang C, Mu Z, Chervoneva I, et al. Longitudinally collected CTCs and CTC-clusters and clinical outcomes of metastatic breast cancer. Breast Cancer Res Treat. 2017;161:83–94. doi: 10.1007/s10549-016-4026-2. [DOI] [PubMed] [Google Scholar]
- Zaidman B-Z, Yassin M, Mahajna J, Wasser SP. Medicinal mushroom modulators of molecular targets as cancer therapeutics. Appl Microbiol Biotechnol. 2005;67:453–68. doi: 10.1007/s00253-004-1787-z. [DOI] [PubMed] [Google Scholar]