

Abstract
Peroneal palsy with loss of active dorsal flexion in foot can be surgically treated by anterior transfer of tibialis posterior tendon. Two techniques are available, classic and modified Barr’s technique of the anterior transfer of tibialis posterior tendon, with different place of tendon’s reinsertion. The aim of the study is evaluation of the degree of active dorsal flexion in foot, and appearance of varus position and hipercorrection of the foot, by comparing the results of the two operative techniques. The study included 40 patients with peroneal irreparable palsies, divided into two equally sized groups. The first group was treated by classic Barr’s technique. The other group of patients was treated by modified Barr’s technique. The group treated by modified Barr’s technique exhibited better functional results. Active dorsal flexion achieved between 95o (in 35% cases) and 90o (in 50% cases), while varus position and hipercorrection of the foot were absent. In the second group of 20 patients, treated by classic Barr’s technique, 80o (40%) and 90o (25%) of active dorsal flexion, indicated worse functional postoperative results. Active dorsal flexion of 70o achieved by this method in two cases (10%), represents unsatisfactory functional result. Varus position of the foot was recorded in 5 cases (25%) and hipercorrection in 4 cases (20%). Modified Barr’s technique is surgical method with better functional and postoperative results in treatment of irreparable peroneal palsy
Keywords: peroneal palsy, tendon transfer, active dorsal flexion
INTRODUCTION
Irreparable peroneal palsies, without possibility of functional recovery, can be treated by anterior transfer of tibialis posterior tendon. Absence of innervation in neuromuscular junction, with loss of function, may be an indication for tendon transfer (1). Functional recovery of injured nerve can be evaluated electromyographycaly, by interval tracking of Tinnel sign and by Hidgets method of evaluation of postoperative results in the sense of motor and sensory recovery (2). Electromyographic evaluation of reinnervation of neuromuscular junction is not a guarantee of functional recovery, because electomyography is rather functional than diagnostic test (3). The aim of anterior transfer of tibialis posterior tendon, in the case of irreparable peroneal palsy, is reestablishment of lost active dorsal flexion in foot (4). Anterior transfer of tibialis posterior tendon, which primary function is plantar flexion of the foot, with reinsertion on cuboid, or one of the cuneiform or metatarsal bones, is convenient type of tendon transfer in irreparable peroneal palsy (5). Indications for tibialis posterior anterior transfer (6):
Irreparable, central and peripheral, peroneal palsies
Pes equinovarus in children caused by poliomyelitis (peroneal musculature is seriously weakened or paralyzed, with intact tibialis posterior)
Dinamic varus deformity in spastic cerebral paralysis
Cavovarus deformity in Chartot-Mariae-Tooth disease
Duchenne muscular dystrophy
Recurrence of forefoot deformity in club foot
Other conditions that weaken dorsiflexion of the foot (e.g. traumatic injuries)
Anterior transfer of tibialis posterior tendon serves two purposes (7):
Removal of tibialis posterior tendon as deforming force
Establishment or augmentation of active dorsal flexion in foot.
Two operative techniques are available (6,8):
Transfer of the tendon through interosseus membrane
Routing the tendon around the medial side of tibia and through anterior compartment of leg to the dorsum of foot
Anterior transfer of tibialis posterior tendon could be performed by four variations of operative technique (9):
CLASSIC BARRS TECHNIQUE - reinsertion of tibialis posterior tendon on either second or third cuneiform bone, or at the base of either second or third metatarsal bone, after desinsertion from the navicular bone, with passage of the tendon through the interosseus membrane of the leg
MODIFIED BARR S TECHNIQUE-procedure identical to the classic Barrs technique, but with reinsertion on cuboid bone (The technique developed at the Clinic for Plastic and Reconstructive Surgery (University of Sarajevo Clinics Centre)
OBERS TECHNIQUE OF TIBIALIS POSTERIOR TRANSFER-routing of tibialis posterior tendon around the medial side of tibia and through anterior compartment of the leg, with reinsertion at the basis of the third metatarsal bone
HATT’S MODIFICATION OF OBER S TECHNIQUE - reinsertion of tibialis posterior tendon on the medial cuneiform bone
Anterior transfer of tibialis posterior tendon removes dynamic deformity of the foot, while establishing active dorsal flexion (10). The aim of the study is to compare success of classic and modified Barr’s techniques by evaluating the degree of active dorsal flexion after anterior transfer of tibialis posterior tendon and by observing unfavorable postoperative results in the form of varus position and hipercorrection of the foot.
MATERIAL AND METHODS
The study included 40 patients with irreparable peroneal palsies. The first group of 20 patients was treated by classic Barr’s technique while the modified technique was applied in the other group of 20 patients. Criteria for inclusion in the study:
-Patients of different sex
-Clinically and diagnostically verified lesion of peroneal nerve
-Patients treated by classic and modified Barrs technique
Criteria for exclusion from the study:
-Untreated peroneal palsies
-Peroneal palsies treated by other operative techniques of tibialis posterior transposition
Denervation of neuromuscular junction was verified electromyographycaly before the surgery. All the deforming changes in ankle joints were also corrected. Functional and full range of motions of joints before tendon transfer are essential for all types of tendon transfers. Postoperative results were evaluated by:
-Clinical examination
-Degree of active dorsal flexion of the foot
-Presence of varus position and hipercorrection of the foot
RESULTS AND DISCUSSION
We have evaluated the results of operative treatment of 40 patients with irreparable peroneal palsies, loss of active dorsal flexion in foot and functional range of motion in the ankle joint. The patients were divided in two identically sized groups. The first group was treated by classic Barr’s technique and the second group was treated by modified Barr’s technique.
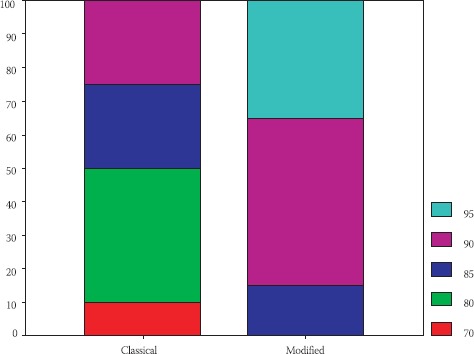
The degree of active dorsal flexion, achieved by classic and modified Barr’s techniques is represented in Table 1. Comparison of these two techniques according to the achieved active dorsal flexion of the foot, is given in Table 2 and Figure 1. Varus position and hipercorrection of the foot, as unfavorable postoperative results, were observed only in the group of patients treated by classic Barrs technique, as illustrated in Tables 3 and 4 and Figures 2 and 3. Better functional results, with higher degree of active dorsal flexion of the foot - 95o (35%) and 90o (50%), were found in the group of patients treated by modified Barr’s technique. Also, varus position and hipercorrection were completely absent. In the group of patients treated by classic Barr’s technique, functional postoperative results were less successful. Active dorsal flexion of 95o was not achieved. The highest degree of the achieved active dorsal flexion was 90o (25%) while 85o was achieved in certain cases (25%). Active dorsal flexion of 70o was evaluated in 10% patients and is considered bed functional result. Varus position was found in 5 cases (25%) and hipercorrection in 4 cases (20%).
TABLE 1.
Parameter of active dorsal flexion evaluated by maximal, minimal, median and standard deviation

TABLE 2.
Absolute and relative frequencies of the treated patients according to the parameter of active dorsal flexion
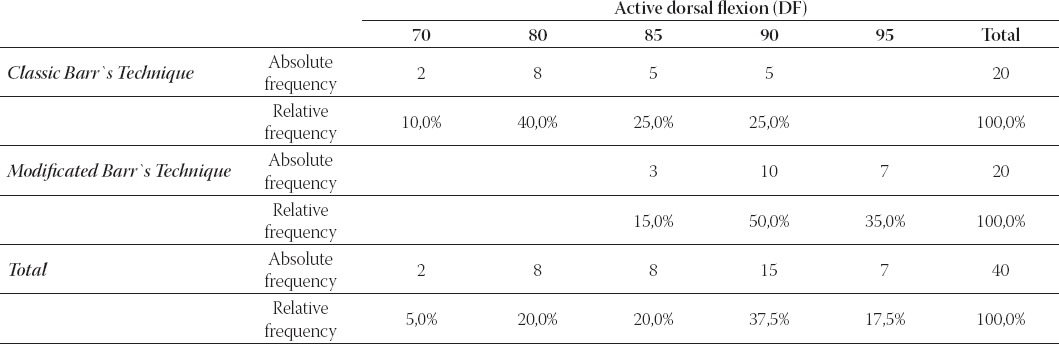
FIGURE 1.
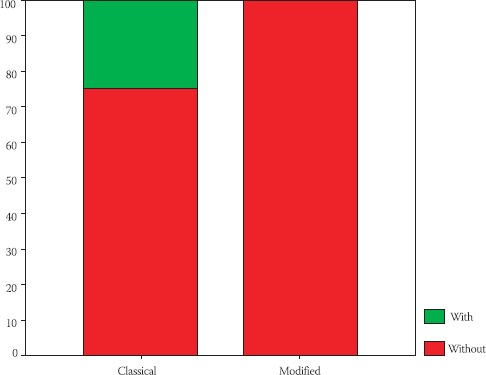
Relative frequencies of active dorsal flexion parameter according to the operative techniques
TABLE 3.
Absolute and relative frequencies of treated patients according to the varus position parameter
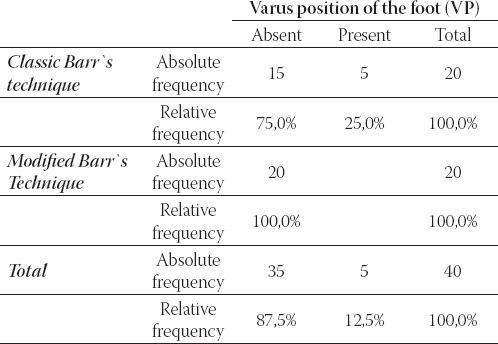
TABLE 4.
Absolute and relative frequencies of treated patients according to hypercorrection parameter
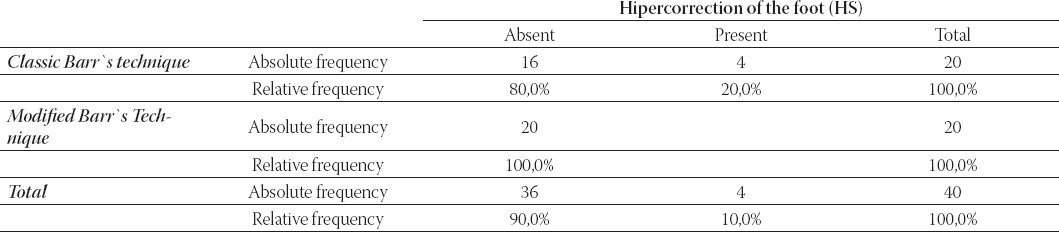
FIGURE 2.
Relative frequencies of the varus position parameter according to the operative techniques
FIGURE 3.
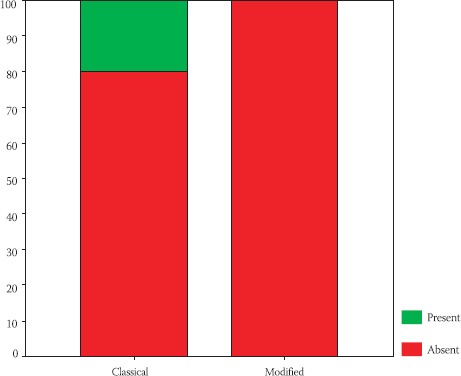
Relative frequencies of the hipercorrection parameter according to the operative techniques
CONCLUSION
Anterior transfer of tibialis posterior tendon in the cases of irreparable peroneal palsy removes dynamic deformity of the foot. Redirection of tendon in relation to medial malleolus diminishes the force of plantar flexion of the foot. Comparing the two methods of Barr’s technique of tibialis posterior transfer, statistical significance was found in differences in postoperative degree of active dorsal flexion of the foot and in frequencies of varus position and hipercorrection. We found correlation between operative technique and postoperative results. Better functional results were obtained by modified Barr’s technique, with complete absence of varus position and hipercorrection of the foot, and higher degree of active dorsal flexion. It implicates faster functional postoperative recovery and better walking stability. Tibialis posterior tendon has adequate length for reinsertion on cuboid bone, without angulation. According to our clinical experience, modified Barrs technique is the method of choice in the treatment of irreparable peroneal palsies.
REFERENCES
- 1.McCarthy J. G. The Hand. Part 2. Vol. 8. W.B. Saunders Company; 1998. Plastic Surgery. [Google Scholar]
- 2.Samardžić M, Antunović V, Grujičić D. Povrede i oboljenja perifernih nerava;Školska knjiga. Zagreb. 1990 [Google Scholar]
- 3.Omer G.E., Jr . Assessment of Peripheral nerve injuries. Vol. 3. St. Louis: CU Mosby; 1999. The technique and Timing of Tendon Transfers. [Google Scholar]
- 4.Beasly R. W. Mirror Company. Robert Hurley; 2000. Principles of Tendon Transfers in Campbell Times. [Google Scholar]
- 5.Kling T. F, Kaufer H, Hesinger R. N. Split posterior tibialis transfer in children with cerebral spastic paralysis and equinovarus deformity. J. Bone Joint Surgery. 1998;67A:186. [PubMed] [Google Scholar]
- 6.Morrisy R.T. Atlas of Pediatric Orthopaedics Surgery. Philadelphia: J. B. Lippincot Company; 2003. [Google Scholar]
- 7.Colemman S. S. Complex foot deformities in children. Philadelphia: Lea/Febiger; 1998. [Google Scholar]
- 8.Johnson W. L, Lester E. L. Transposition of Posterior Tibial Tendon. Raven Press, Ltd; 2003. [PubMed] [Google Scholar]
- 9.Lambrinudi C. The New operation of drop foot. Bone Joint Surgery. 1998 [Google Scholar]
- 10.Hoffer M. M, Lehmann M, Mitanni M. Long term follow-up on tendon transfers in patients with cerebral palsy. J. Hand Surgery. 1999;3:67B:432. doi: 10.1016/s0363-5023(86)80232-5. [DOI] [PubMed] [Google Scholar]