

Abstract
Background
Community-based walking programs represent a low-cost, accessible approach to increasing physical activity among inactive adults. However, recruiting participants from vulnerable and hard-to-reach groups remains a challenge. This study examined the reach, retention, sociodemographic and health characteristics, physical activity levels and motivators of participants in Heart Foundation Walking, a nationwide Australian community-based walking program.
Methods
Descriptive cross-sectional analyses were undertaken with data from 22,416 participants aged 15+ years in the Heart Foundation Walking registration database in December 2015, and from four surveys of participants in 2010 (n = 2400), 2011 (n = 3274), 2012 (n = 4158) and 2015 (n = 1890).
Results
Heart Foundation Walking reached participants in every geographic region of Australia, including remote and sparsely populated regions, and engaged sizeable proportions of the following at-risk participants: older than 60 years (>70%); with very low incomes (17–25%); who were overweight or obese (around 60%); and with one or more chronic disease or disease risk factors (57–81%). For all demographic groups, one-year retention rates were at least 75%. Seventy percent of participants met physical activity recommendations. Over 75% reported joining the program for health and fitness reasons while the most cited motivator for continuing was the social aspect (57–73%).
Conclusions
Volunteer-run, group-based walking programs can have substantial reach and retention, in particular among those at risk for physical inactivity. The provision of opportunities for social interaction appears to be a key program element in promoting long-term participation, including among high-risk groups.
Keywords: Walking, Community, Program, Reach, Retention, Socioeconomic
Background
Given the benefits of physical activity to overall health and well-being, high population levels of inactivity remain of concern, in particular in vulnerable groups such as older adults or those experiencing socioeconomic disadvantage [1, 2]. Community-based programs represent a promising approach for engaging large numbers of people in the settings in which they live [3]. Walking is an activity involving low cost, risk of injury, and skill requirements. Group-based walking programs have been shown to be effective in increasing physical activity [4, 5] and improving health [6]. However, recruitment into such programs, particularly from high-risk groups, is challenging [7], and low retention is often problematic [8, 9]. Little is known about reach, retention rates, participant characteristics, or successful implementation elements of walking programs. Evaluations of ‘real-world’ large-scale physical activity programs in the community are also scarce, and have been highlighted as a priority [5]. Evidence of elements of successful walking group programs would inform future community-based physical activity programs with potential broad and equitable reach and impact.
Heart Foundation Walking (http://walking.heartfoundation.org.au/) is a voluntary group-based community walking program rolled out across Australia in 2007 to facilitate regular physical activity in safe, supportive social environments. There were 1287 registered groups, with varying numbers of participants, as of December 2015. The aim of this study was to examine the reach, retention, sociodemographic and health characteristics, physical activity levels and motivations for joining and remaining in the program.
Methods
Participants
Data were drawn from the Heart Foundation Walking national registration database as of 13th December 2015 (n = 22,416 participants aged ≥15 years; 20,753 walkers, 1663 Walk Organisers), and from four surveys of participants registered at the time of each survey. These were undertaken in 2010 (n = 1984 walkers and 416 Walk Organisers, representing response rates of 33 and 30%); 2011 (2796 walkers, 478 Walk Organisers, 44 and 45%); 2012 (3585 walkers, 573 Walk Organisers, 33 and 32%) and 2015 (1601 walkers, 289 Walk Organisers, 15 and 25%). Surveys were sent by email or mail in 2010, 2011 and 2012; and email only in 2015. The research was performed in accordance with the Declaration of Helsinki, and an exemption from Ethics review (ref 2015–245) was granted by the Deakin University Human Research Ethics Committee for analysis of this routinely collected de-identified data.
Program
Heart Foundation Walking utilises local government and community health centre staff to support the program as part of their core business, with walks led by local volunteer Walk Organisers. It is promoted through low cost local media releases, posters and flyers in health and community centres, social media and limited digital advertising and bring a friend campaigns. Retention strategies, which are of no cost to participants and minimal cost to the organization, include a Walker Recognition Scheme which rewards participants upon reaching milestones; quarterly newsletters; group anniversary certificates; annual events such as large group walks and volunteer workshops; annual photo competitions and “golden shoe awards” for key supporters.
Measures and analyses
Upon registration, all participants reported their demographic data and how they heard about the program. Based on residential address, participants were classified into one of 88 geographic regions (known as Statistical Areas Level 4: SA4) of Australia. Reach rates were calculated as the numbers of SA4s in which participants were located, and the number of participants as a proportion of the population in each SA4. Residential address was also used to determine Socioeconomic Index for Areas (SEIFA) [10], a marker of neighbourhood socioeconomic disadvantage.
In each survey, using standard items participants reported their age, household structure, gross household income category, height and weight (for calculating body mass index [BMI]), and if they had any specified chronic diseases or risk factors. The Active Australia survey, which assesses the total time in the last week spent walking (for recreation, exercise, or to get from place to place); in vigorous gardening/yard work (not used in calculating physical activity in these analyses); in other vigorous-intensity activities; and in other moderate-intensity activities, was used to assess physical activity. The Active Australia survey has acceptable reliability [11] and criterion validity [12]. Data were treated according to standard protocols [13], with a dichotomous variable created to indicate participation in at least 150 min/week of at least moderate intensity physical activity in at least five sessions. Using questions developed for the study, participants were asked to select from a list of responses, the main reasons they joined the program; and a separate open-ended question on the main reasons they were still participating. They were also asked to rate on a 6-point Likert scale how important they perceived three elements: the Walker recognition scheme; quarterly newsletters; and special events.
Because numbers of participants responding to more than one survey were relatively low, and not all surveys were ID-linked, survey data are presented as serial cross-sectional data. Descriptive analyses were used to examine reach and participant characteristics, retention, and reasons for participation. Where available, comparisons with the general population were made to examine representativeness of participants. Linear regression was used to examine differences in retention time by recruitment mode.
Results
Reach and participant characteristics
Overall, walkers (n = 20,753) had participated in Heart Foundation Walking for an average 2.4 (SD = 2.7) years. Analysis of the national database indicated that Heart Foundation Walking participants were located in all 88 SA4 regions of Australia, with a median of 245 participants/region (range 8–804). The median number of participants as a proportion of the total population in each region was 148.4/100,000 residents (range 3.8–1000/100,000). Remote and sparsely populated regions were over-represented in those with high participation rates (Fig. 1).
Fig. 1.
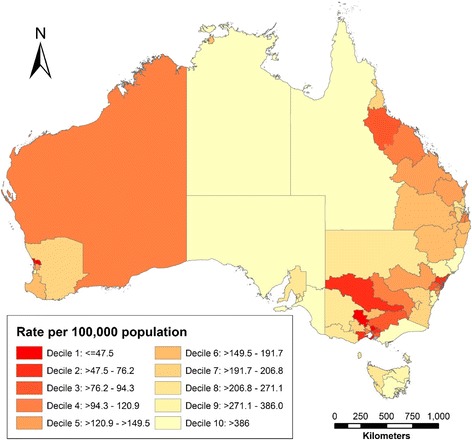
Participation rates per 100,000 population of Heart Foundation Walking across Australia (note Australia’s population reside predominantly in coastal cities, particularly in the east and south east, with sparser populations in other regions and inland)
For the years survey data were available, walkers had an average age of 64 years, and more than three-quarters were women (Table 1). Around a quarter lived alone, a figure substantially higher than that for the general population (9%) [14]. The income distribution of walkers was skewed towards low income categories. A sizeable proportion had an average annual household income of less than $25,000, a very low income threshold (for example, the mean household income in 2013–14 was $107,276) [15].
Table 1.
Socioeconomic characteristics of walkers participating in each surveya
| 2010 (n = 1984) | 2011 (n = 2796) | 2012 (n = 3585) | 2015 (n = 1601) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| All | Female | Male | All | Female | Male | All | Male | Female | ||
| Age (Mean, SD) | Data not available | 63.9 (11.9) | 62.9 (12.2) | 67.5 (9.9) | 64.3 (11.8) | 63.5 (12.0) | 67.3 (10.6) | 64.6 (10.0) | 63.6 (9.9) | 68.4 (9.1) |
| Age group (%) | Data not available | |||||||||
| 15–29 | 1.6 | 1.9 | 0.2 | 2.0 | 2.2 | 1.2 | 0.9 | 1.1 | 0.0 | |
| 30–39 | 3.3 | 3.6 | 2.3 | 2.6 | 3.1 | 0.6 | 1.9 | 1.9 | 2.1 | |
| 40–49 | 6.2 | 7.0 | 3.0 | 5.3 | 5.5 | 4.3 | 5.0 | 5.9 | 1.5 | |
| 50–59 | 16.1 | 18.0 | 8.9 | 16.0 | 17.5 | 10.7 | 14.3 | 15.9 | 8.0 | |
| 60–69 | 39.9 | 39.2 | 42.5 | 40.8 | 41.5 | 38.0 | 48.3 | 50.0 | 41.9 | |
| 70–79 | 27.3 | 25.0 | 35.8 | 27.1 | 24.6 | 36.2 | 26.3 | 23.0 | 39.1 | |
| 80+ | 5.6 | 5.1 | 7.3 | 6.3 | 5.6 | 9.0 | 3.3 | 2.2 | 7.3 | |
| Sex (%) | Data not available | |||||||||
| Female | 79.2 | 78.5 | 79.5 | |||||||
| Male | 20.8 | 21.5 | 20.5 | |||||||
| Household structure (%) | ||||||||||
| Person living alone | 25.7 | 27.6 | 30.4 | 17.1 | 26.7 | 28.7 | 19.3 | 25.7 | 27.4 | 19.3 |
| Couple only | 50.7 | 51.9 | 47.3 | 69.1 | 51.8 | 48.2 | 65.0 | 54.0 | 50.9 | 66.4 |
| Couple living with their child(ren) | 11.0 | 11.9 | 12.2 | 10.6 | 11.2 | 11.7 | 9.4 | 10.6 | 11.5 | 7.3 |
| Single person living with their child(ren) | 2.6 | 2.7 | 3.4 | 0.3 | 2.6 | 3.0 | 1.1 | 2.6 | 3.0 | 1.2 |
| Adult living at home with parents | 1.3 | 1.0 | 1.1 | 0.7 | 1.1 | 0.9 | 1.7 | 0.7 | 0.7 | 0.6 |
| Group household | 1.8 | 1.4 | 1.7 | 0.3 | 1.3 | 1.3 | 1.3 | 1.3 | 1.3 | 1.2 |
| Other | 2.8 | 1.3 | 1.6 | 0.3 | 2.5 | 3.0 | 1.0 | 2.6 | 2.4 | 3.1 |
| Prefer not to say | 4.0 | 2.2 | 2.4 | 1.4 | 2.9 | 3.3 | 1.1 | 2.4 | 2.8 | 0.9 |
| Household Income (%) | ||||||||||
| Below $25,000 | 24.2 | 25.5 | 25.8 | 24.2 | 22.6 | 22.7 | 22.5 | 17.0 | 16.7 | 18.0 |
| $25,000–$40,000 | 18.5 | 19.2 | 16.9 | 27.5 | 19.1 | 17.9 | 23.6 | 15.9 | 15.5 | 17.4 |
| $40,001 to $55,000 | 7.2 | 9.0 | 8.5 | 10.9 | 8.9 | 8.7 | 9.6 | 9.5 | 9.1 | 10.7 |
| $55,001 to $70,000 | 5.2 | 5.8 | 6.1 | 4.8 | 6.1 | 5.6 | 8.1 | 7.1 | 6.8 | 8.3 |
| $70,001 to $85,000 | 3.5 | 3.6 | 3.3 | 4.8 | 4.8 | 4.9 | 4.3 | 4.9 | 4.8 | 5.2 |
| $85,001 to $100,000 | 2.1 | 3.1 | 3.2 | 2.5 | 3.4 | 3.3 | 3.5 | 4.2 | 4.3 | 3.7 |
| $100,001 to $120,000 | 2.2 | 3.2 | 3.4 | 2.3 | 2.8 | 2.9 | 2.5 | 2.2 | 2.0 | 3.1 |
| Over $120,000 | 2.8 | 3.4 | 3.5 | 3.0 | 3.6 | 3.4 | 4.5 | 4.6 | 4.6 | 4.6 |
| Prefer not to say | 34.4 | 27.2 | 29.1 | 19.9 | 28.7 | 30.6 | 21.4 | 34.8 | 36.2 | 29.1 |
aTable indicates the numbers included in each set of analyses
Retention
Three month program retention rate was 95%; 6 month retention was 88%; 1 year retention 75%; and 3 year retention 36%. Until December 2014, 11% of withdrawals from the program were due to ill health or death.
Walker retention time according to socioeconomic characteristics in the entire registration database (n = 20,750 walkers, excluding 3 with no retention date data) is presented in Table 2. Participants from all SEIFA deciles were represented. Overall 14.5% of walkers reported a first language other than English, which is slightly higher than the population estimate of 10% [16]. The proportion of registrants who reported being Aboriginal or Torres Strait Islander (ATSI: 1.4%) was slightly lower than the population estimate of 3% [17]. Retention time was slightly lower among participants who were unemployed than among those who reported their employment status as other or home duties; but did not differ markedly according to gender, first language or ATSI status.
Table 2.
Walker retention time by socioeconomic characteristics amongst current walker participants in Heart Foundation Walking (n = 20,750)a
| 0-3mo (n = 5270) % | 3-6mo (n = 1094) % | 6-12mo (n = 1978) % | 1-3 yr. (n = 6145) % | 3 + yr. (n = 6263) % | All (n = 20,750) % | Years retention | |
|---|---|---|---|---|---|---|---|
| M (SD) | |||||||
| Gender | |||||||
| Female | 83.3 | 79.5 | 82.0 | 79.4 | 78.5 | 80.4 | 2.3 (2.7) |
| Male | 16.7 | 20.5 | 18.0 | 20.6 | 21.5 | 19.6 | 2.5 (2.7) |
| SEIFA decile | |||||||
| 1: Most disadvantaged | 7.3 | 5.4 | 6.3 | 12.0 | 8.8 | 9.1 | 2.6 (2.3) |
| 2 | 9.7 | 9.8 | 6.6 | 8.5 | 11.2 | 9.5 | 2.7 (2.6) |
| 3 | 6.6 | 7.8 | 6.9 | 8.6 | 8.2 | 7.9 | 2.5 (2.3) |
| 4 | 11.3 | 10.6 | 12.2 | 13.6 | 10.3 | 11.8 | 2.4 (2.4) |
| 5 | 10.4 | 13.7 | 10.2 | 12.2 | 9.8 | 10.9 | 2.3 (2.3) |
| 6 | 10.2 | 9.9 | 14.9 | 10.4 | 9.3 | 10.4 | 2.5 (2.7) |
| 7 | 16.3 | 10.3 | 12.1 | 9.3 | 9.0 | 10.9 | 2.1 (2.5) |
| 8 | 9.6 | 8.6 | 9.4 | 9.3 | 14.5 | 11.0 | 3.3 (3.3) |
| 9 | 9.3 | 13.6 | 11.1 | 8.2 | 9.0 | 9.3 | 2.4 (2.6) |
| 10: Least disadvantaged | 9.4 | 10.1 | 10.2 | 7.9 | 9.9 | 9.2 | 2.9 (3.2) |
| Occupation | |||||||
| Employed | 22.3 | 22.3 | 21.7 | 21.0 | 18.8 | 20.8 | 2.2 (2.5) |
| Self-employed | 3.0 | 3.8 | 4.6 | 4.2 | 3.6 | 3.7 | 2.2 (2.2) |
| Semi-retired | 4.8 | 5.5 | 5.4 | 5.2 | 4.1 | 4.8 | 2.0 (2.0) |
| Retired | 48.9 | 46.9 | 44.2 | 47.0 | 47.7 | 47.4 | 2.3 (2.6) |
| Student | 1.5 | 2.4 | 3.0 | 2.0 | 1.7 | 1.9 | 2.0 (2.0) |
| Home duties | 5.9 | 8.6 | 11.0 | 10.0 | 10.4 | 9.1 | 2.8 (2.9) |
| Unemployed | 4.6 | 3.2 | 3.8 | 3.5 | 2.5 | 3.5 | 1.7 (2.1) |
| Other | 9.1 | 7.3 | 6.3 | 7.2 | 11.2 | 8.8 | 3.1 (3.5) |
| English first language | |||||||
| Yes | 75.5 | 92.0 | 87.4 | 91.9 | 85.8 | 85.5 | 2.3 (2.5) |
| No | 24.5 | 8.0 | 12.6 | 8.1 | 14.2 | 14.5 | 2.5 (3.6) |
| Aboriginal or Torres Strait Islander | |||||||
| Yes | 1.4 | 0.7 | 0.8 | 1.1 | 1.9 | 1.4 | 2.6 (2.3) |
| No | 98.6 | 99.3 | 99.2 | 98.9 | 98.1 | 98.6 | 2.4 (2.7) |
aTable indicates the numbers included in each set of analyses
Most participants (42%) heard about the program via word of mouth, 18% via traditional media (TV, radio, newspaper, flyer), 11% from a health professional, and 9% internet/social media. Retention duration was longer among those who initially joined as the result of word of mouth (2.5y, SD 2.6) and traditional media (2.5y, SD 2.5) than among those recruited via a health professional (2.1y, SD 1.8) or internet/social media (1.3y, SD 1.5), p < 0.01.
Health and physical activity levels
Table 3 presents the health characteristics and physical activity levels of participants. Approximately 60% of walkers were overweight or obese each year, which is close to the population estimate (62.8%) in the most recent Australian Health Survey [18]. Many walkers (69–81%) reported at least one chronic disease or risk factor, most commonly arthritis, high blood pressure, high cholesterol and back pain. In comparison with the general population, Australian Health Survey data for 2011–12 show lower population prevalences of comparable conditions. Almost 15% of the Australian population report arthritis, 13% back problems, 10% hypertensive disease, 10% asthma, 5% heart or vascular disease, or had suffered a stroke, and 4.6% diabetes [18, 19].
Table 3.
Weight and health characteristics of walkers participating in each Heart Foundation Walking surveya
| 2010 (n = 1984) | 2011 (n = 2796) | 2012 (n = 3585) | 2015 (n = 1601) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| All | All | Female | Male | All | Female | Male | All | Female | Male | |
| BMI (mean, SD) | 27.0 (5.7) | 27.1 (5.5) | 26.9 (5.5) | 28.1 (5.4) | 27.0 (5.5) | 26.8 (5.6) | 27.8 (5.2) | 26.9 (5.1) | 26.6 (5.0) | 27.7 (5.0) |
| BMI category (%)b | ||||||||||
| Not overweight | 41.1 | 39.8 | 42.9 | 27.9 | 39.6 | 42.6 | 29.2 | 40.5 | 43.0 | 31.7 |
| Overweight | 35.5 | 36.2 | 34.2 | 43.5 | 38.3 | 36.5 | 44.8 | 36.2 | 34.4 | 42.3 |
| Obese | 23.5 | 24.1 | 22.9 | 28.6 | 22.0 | 20.9 | 26.0 | 23.4 | 22.6 | 26.0 |
| Chronic disease (%) | ||||||||||
| Arthritis | 36.2 | 43.2 | 45.2 | 35.2 | 43.1 | 45.2 | 35.4 | 37.5 | 38.9 | 32.3 |
| Asthma | 12.3 | 12.5 | 12.8 | 10.8 | 11.9 | 12.1 | 11.4 | 11.1 | 11.6 | 9.0 |
| Back pain | 14.6 | 18.8 | 18.6 | 19.4 | 17.8 | 17.9 | 17.5 | 15.0 | 15.0 | 14.9 |
| Respiratory disease | 3.6 | 4.2 | 3.7 | 5.9 | 3.9 | 3.6 | 4.8 | 3.8 | 4.0 | 3.1 |
| High blood pressure | 31.3 | 35.3 | 33.9 | 40.3 | 36.0 | 35.1 | 39.6 | 28.1 | 26.6 | 33.9 |
| High cholesterol | 27.4 | 27.7 | 27.6 | 27.9 | 26.3 | 26.6 | 25.1 | 20.0 | 20.0 | 20.2 |
| Heart disease | 8.8 | 11.1 | 8.0 | 22.6 | 10.7 | 8.0 | 21.1 | 8.9 | 6.6 | 18.0 |
| Diabetes | 10.0 | 10.5 | 8.8 | 16.5 | 10.8 | 8.6 | 18.6 | 8.7 | 6.9 | 15.5 |
| Any one (or more) of the above conditions/risk factors (%)c | 73.5 | 79.5 | 78.4 | 83.1 | 80.9 | 80.2 | 83.5 | 69.3 | 67.8 | 74.8 |
| 2 or more conditions/risk factors | 41.6 | 46.9 | 45.7 | 50.8 | 45.9 | 44.9 | 49.9 | 38.1 | 37.9 | 39.1 |
| 3 or more conditions/risk factors | 18.4 | 23.0 | 21.9 | 26.8 | 21.8 | 21.2 | 24.2 | 17.3 | 16.4 | 20.5 |
| Physical activity min/week (mean, SD) | Not in survey | 537.6 (556.3) | 521.0 (536.8) | 597.4 (618.7) | 541.6 (532.6) | 532.6 (533.1) | 569.1 (532.2) | 541.7 (573.1) | 528.5 (556.0) | 592.2 (632.8) |
| Walking min/week (mean, SD) | Not in survey | 241.8 (257.5) | 241.3 (261.5) | 246.3 (244.5) | 229.7 (226.4) | 229.7 (232.3) | 229.4 (205.1) | 258.1 (262.4) | 254.9 (261.0) | 270.7 (267.8) |
| Meeting physical activity guidelinesd (%) | Not in survey | 70.2 | 69.7 | 72.3 | 70.9 | 70.1 | 73.0 | 71.3 | 70.8 | 73.2 |
aTable indicates the numbers included in each set of analyses
bBased on WHO cutpoints [31]
cCategories 1 or more, 2 or more and 3 or more not mutually exclusive and hence may sum to >100%
dDefined as the accumulation of at least 150 min of activity and at least 5 sessions of activity over 1 week
A separate analysis of the local community persons who organized the walks (data not shown) indicated that Walk Organisers had comparable sociodemographic profiles to those of participant walkers. The average BMI of Walk Organizers was also comparable to that of participant walkers at around 27 kg/m2 at every survey year. The proportions of Walk Organisers reporting at least one chronic disease or risk factor were slightly lower than those amongst walkers, though still high (57–69%), with around a third reporting two or more conditions or risk factors.
Walkers spent an average of about 9 h per week engaged in physical activity overall and 4 h per week walking. Approximately 70% of walkers met physical activity guidelines. Walk Organisers tended to have higher levels of physical activity (mean ~11 h/week), walking (~5 h/week), and adherence to guidelines (80%) (data not shown).
Motivators for joining and maintaining participation
Table 4 shows various reasons for joining Heart Foundation Walking. Though respondents were permitted to select numerous reasons, improving fitness, health and weight loss were some of the more popular initial motivational factors for joining. Meeting new people became a more important motivator for joining over the survey years. The main reason that participants reported maintaining participation was the social aspect, particularly among women. Commonly reported ‘other’ responses included to support/accompany a spouse/friend; to walk the dog; or for mental wellbeing. Across the survey years, the walker recognition scheme, newsletters and special events were perceived as somewhat or very important by on average 69, 70 and 70% of the sample respectively.
Table 4.
Main reasons walkers joined/still participate in Heart Foundation Walking by yeara
| 2010 (n = 1984) | 2011 (n = 2796) | 2012 (n = 3585) | 2015 (n = 1601) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| All | Female | Male | All | Female | Male | All | Female | Male | ||
| Main reasons JOINED (%)b | ||||||||||
| To manage my weight | 45.4 | 53.4 | 53.9 | 52.1 | 50.8 | 50.6 | 51.1 | 46.7 | 47.7 | 42.8 |
| To meet new people | 48.8 | 55.4 | 56.7 | 50.4 | 59.0 | 60.7 | 52.8 | 62.2 | 63.6 | 56.6 |
| To improve my fitness | 76.8 | 85.8 | 86.0 | 84.6 | 82.2 | 82.7 | 81.0 | 81.0 | 81.7 | 78.3 |
| To have time out from other commitments (at 2010 this was phrased as “to have time to myself”) | 8.3 | 19.9 | 21.2 | 14.6 | 20.4 | 21.5 | 15.6 | 17.4 | 18.5 | 13.1 |
| To look and feel good | 44.7 | 39.0 | 40.9 | 31.8 | 33.8 | 35.3 | 27.4 | 28.7 | 29.9 | 24.2 |
| To improve my health | 67.1 | 79.9 | 79.4 | 81.9 | 81.9 | 81.5 | 83.2 | 80.2 | 79.4 | 83.5 |
| To relieve and manage stress | 19.3 | 29.8 | 32.0 | 21.1 | 29.9 | 31.6 | 22.9 | 29.0 | 30.9 | 21.4 |
| For fun / enjoyment | 45.8 | 60.4 | 61.7 | 55.6 | 57.2 | 58.1 | 53.6 | 59.1 | 60.6 | 53.5 |
| To have more energy | 33.2 | 42.2 | 44.3 | 33.3 | 38.9 | 40.9 | 31.5 | 35.5 | 38.5 | 23.9 |
| Because a doctor / health professional recommended me | 8.3 | 13.7 | 12.0 | 19.8 | 12.3 | 11.0 | 16.4 | 8.8 | 8.1 | 11.6 |
| To balance other things I do (e.g. over-indulgence) | 4.8 | 11.9 | 11.5 | 13.2 | 10.8 | 10.8 | 10.5 | 8.1 | 7.9 | 8.9 |
| To spend time with others | 41.1 | 46.6 | 48.4 | 39.5 | 42.7 | 43.6 | 39.3 | 41.6 | 42.4 | 38.5 |
| Other | 6.8 | 2.6 | 2.7 | 2.1 | 3.7 | 3.7 | 3.7 | 4.7 | 4.6 | 5.2 |
| Unsure | 0.2 | 0.1 | 0.1 | 0.4 | 0.1 | 0.1 | 0.0 | 0.4 | 0.3 | 0.6 |
| Main reasons STILL PARTICIPATINGc (Not asked in 2010) (%) | ||||||||||
| Social aspect | – | 61.4 | 64.2 | 51.2 | 56.7 | 58.7 | 49.8 | 73.4 | 75.9 | 64.4 |
| Fitness / exercise | – | 54.7 | 54.9 | 54.9 | 53.5 | 54.1 | 52.0 | 55.0 | 53.7 | 59.5 |
| Health | – | 25.2 | 25.1 | 23.8 | 26.4 | 24.9 | 31.5 | 21.5 | 21.0 | 23.2 |
| Wellbeing | – | 2.7 | 2.9 | 1.4 | 7.1 | 7.0 | 6.8 | 2.0 | 1.9 | 2.5 |
| Manage weight / weight loss | – | 6.7 | 6.5 | 6.9 | 5.1 | 5.3 | 3.9 | 2.5 | 2.2 | 3.2 |
| Support / motivation | – | 9.0 | 9.2 | 8.6 | 10.0 | 10.8 | 7.3 | 12.3 | 13.4 | 8.5 |
| Walking locations and condition (e.g. safe, weather) | – | 7.3 | 7.1 | 7.9 | 6.8 | 7.7 | 3.8 | 7.8 | 8.6 | 4.9 |
| Enjoyment | – | 12.0 | 12.9 | 8.6 | 21.6 | 22.8 | 17.0 | 12.3 | 13.1 | 9.5 |
| Other | – | 6.7 | 6.7 | 7.2 | 2.6 | 2.4 | 3.4 | 7.9 | 7.5 | 9.2 |
aTable indicates the numbers included in each set of analyses
bPercentages reflect numbers reporting each reason; these do not sum to 100% since multiple reasons could be provided
cOpen-ended question with key responses coded into categories; again these do not sum to 100% since multiple reasons could be provided
Discussion
Heart Foundation Walking is a large, free, community walking program that is unique in its scale and population reach, engaging more than 22,000 registered participants at the time of this evaluation. The program reached and retained a large number of participants, including vulnerable groups. The program had particularly high reach in remote and sparsely populated regions where physical activity facilities and programs are likely to be limited. Retention rates compare favourably to others reported in the scientific literature [20, 21].
The recruitment success of walking groups is often measured by the numbers of participants joining, rather than the reach to those who stand to benefit most [22]. However, walking groups have the potential to widen health inequities if they are not sensitively targeted to reach and cater to the needs of these high-risk groups [7] including women, people who are socioeconomically disadvantaged, older adults, adults who are overweight or obese, and people with, or at risk of, chronic disease, for whom physical activity may be particularly beneficial, but who may face additional health-related barriers to being active [23]. The data show that the Heart Foundation Walking program had good impact in attracting women; older adults; those who are socioeconomically disadvantaged; and those who have one or more chronic diseases or risk factors. The program also attracted a higher than average proportion of participants who live alone. As not all walkers completed surveys, these data are illustrative rather than comprehensive. Given typically lower than average response rates in mail surveys among those who are socioeconomically disadvantaged [24, 25], for example, these data may under-estimate the true reach of the walking program to these individuals.
The repeat cross-sectional design and lack of a control group preclude strong conclusions regarding particular elements that contributed to the favourable reach and retention rates. Nonetheless, the data describe the elements of one successful model, and suggest some features that may be implemented in future programs. These include the sponsorship by a well-known national organisation; targeting regions that may lack services or comparable initiatives; the use of inexpensive wide-reaching recruitment modes; and facilitating social interactions, which appear to be of increasing importance to participants. Given the perceived importance of low-cost walker recognition schemes, communications and special events by the majority of participants, incorporating these elements into future programs would be warranted. Investigating the reasons for continued participation amongst those who did not rate these features as important could also add to our understanding of how future programs might enhance retention. Future programs could also adopt the volunteer model used here, which builds community capacity and reduces costs by engaging and supporting local volunteers as Walk Organisers. Organisers were more physically active but otherwise had comparable characteristics (sociodemographics, BMI) to participants, hence potentially serving as relatable role models. Analyses of retention times suggest that future programs might focus recruitment efforts on traditional media and encouraging existing participants to recruit others.
Typically, participant drop-out rates present a major concern in community health programs. Substantial heterogeneity makes it difficult to directly compare reach and retention rates across different programs. Despite data gaps, existing reports of broadly comparable programs show that 30–76% of people who begin a new exercise program will drop out within 1 year [20, 21, 26]. The greatest attrition typically occurs in the first 3 months (e.g., 36%) [21], and approximately 50% within 6 months [27]. Results from the present study, showing an average 6-month retention of 88%, 1-year retention of 75%, and average participation duration of 2.4 years among Walkers, compare favourably to the rates reported in the limited available literature. Importantly, voluntary attrition was even lower than the rates reported here, which include non-voluntary drop-out (due to illness or death).
A study of a similar community-based program reported by Jancey and colleagues [20] reported a 6 month retention of 65% (i.e. 35% attrition) among adults aged 65–74 years. Unlike Heart Foundation Walking, retention was poorer among those from disadvantaged areas, and those who were obese, or insufficiently active. Program differences that may explain the comparatively higher retention rates of Heart Foundation Walking include the fact that, unlike Jancey et al. [20], Heart Foundation Walking was designed as a long-term program, fostered word-of-mouth recruitment, and fostered community engagement via recruitment and ongoing investment in volunteers.
Around 70% of Walkers and 80% of Organisers were meeting physical activity recommendations. The most recent population prevalence data suggest that only 43% of Australian adults are meeting recommendations [2]. Notably, it was not possible to determine whether Heart Foundation Walking contributed to these high levels of physical activity or whether the program attracted participants who were more active. However, a previous evaluation of a state-based program suggested that participation for 12 months increased both walking and total physical activity, particularly among initially inactive participants [28].
The data presented suggest that the reasons participants joined Heart Foundation Walking were different from the reasons participants continued with the program. Improving fitness and health appeared to be the most important motivators for joining the program whereas the social aspect was the strongest motivator for continuing. Social engagement may be particularly relevant for walking, as opposed to more vigorous or structured group-based activity such as exercise classes, which typically do not offer the same opportunities to talk with other participants during the activity. These data corroborate findings from a meta-analysis showing the most consistent predictor of participation in physical activity programs among socioeconomically disadvantaged women was a social component [29]. This highlights the importance of focusing on building, strengthening and maintaining social networks that support behaviour change [3], particularly given the documented challenges in maintaining behaviour change [5]. In order to attract participants, future walking programs could implement tailored recruitment campaigns that promote benefits to fitness and health as well as opportunities to meet and spend time with others. In light of the finding that few participants were motivated to join as a result of a health professional recommendation, a ‘bring a friend’ initiative might be a more useful promotional approach. Considering the importance of social factors in retaining participants, programs might also consider activities that enhance opportunities for social engagement, such as walks linked with lunches or picnic days. With the increasing proliferation of mobile phone technology, provision of ‘virtual’ support could also be trialled, for example through online challenges and Facebook/social media support groups, to further facilitate social connectedness among participants. Mobile technology could also be used to provide motivational strategies, such as text message congratulations on significant milestones, or ‘we miss you’ messages for those who haven’t walked for some time. The impact and cost-effectiveness of such strategies could be evaluated in future studies.
Capitalising on the unique evaluation of a large, nationwide physical activity program in a real-world setting, this study utilised data from sizeable numbers of respondents over four survey points to explore reach, retention, participant characteristics and motivators for participation in a national walking group program. Notwithstanding these strengths, the study was limited by its reliance on self-report measures collected with tools that have not been tested for validity or reliability among this study population; and use of a repeat cross-sectional design which meant that temporal sequencing could not be determined. We also did not have access to data on frequency of attendance, and did not measure actual health benefits. It is possible that survey respondents were not representative of Heart Foundation Walking participants more generally. In particular the response rate at 2015 was low, potentially reflecting the shift to email-only administration, given typically lower responses to online than paper-based surveys [30].
Conclusions
| Elements of success |
|---|
| Auspiced by a well-established reputable national non-government organisation |
| Free for members |
| Large reach with groups established nationwide |
| Embedded in and supported by local community |
| Volunteer-led by community members |
| Capacity building |
| Social opportunities |
| Socially-based promotion (members recruiting members) |
| Retention strategies including member incentives |
Walking is a popular activity with health benefits and a low risk of injury that requires little skill or equipment. This study suggests that free group-based walking programs are a promising approach for increasing population levels of physical activity and attracting participants at high risk of inactivity. This study provides a model for such a program, with key elements (summarised in the Box) including backing of a well-known national non-government organisation; support of local government and community health staff; community capacity building via local volunteer Walk Organisers; low-cost and word of mouth promotion; retention strategies including walker recognition schemes, newsletters and annual/special events; and opportunities for social interaction. Though initial motivation factors may include health and fitness, programs should market social aspects as they appear to be an especially important component of group-based walking, particularly for continued participation.
Acknowledgements
Bill Stavreski of the Heart Foundation for assistance with data.
Funding
KB was supported by a NHMRC Principal Research Fellowship, ID 1042442. The contents of the manuscript are the responsibility of the authors and do not reflect the views of the NHMRC.
Availability of data and materials
The dataset analysed during the current study are not publicly available due to privacy and ethical restrictions, since they were collected by the Heart Foundation for the purpose of evaluation only and not for additional research or interrogation. Queries about data may be directed to the corresponding author who will liaise with the data custodian at the Heart Foundation.
Abbreviations
- ATSI
Aboriginal or Torres Strait Islander
- BMI
Body mass index (kg/m2)
- SA4
Statistical Areas Level 4
- SEIFA
Socioeconomic Index for Areas
Authors’ contributions
KB, MW, and MC were responsible for co-conception of the project; MC advised on design; MW was responsible for data collection; KB designed the analytical plan; GA conducted and interpreted statistical analyses; KB and SS interpreted results; KB and SS drafted the manuscript; and GA, MW, MC, and SS contributed to and revised the manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to participate
The Deakin University Human Research Ethics Committee granted an exemption from Ethics review (ref 2015-245) for analysis of this routinely collected de-identified data.
Consent for publication
Not applicable.
Competing interests
Two of the authors (MW, MC) were employees of the Heart Foundation, who oversaw the Walking Program, at the time of the evaluation. The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Kylie Ball, Phone: +61 3 9251 7310, Email: kylie.ball@deakin.edu.au.
Gavin Abbott, Email: gavin.abbott@deakin.edu.au.
Michelle Wilson, Email: Michelle.Wilson@heartfoundation.org.au.
Melanie Chisholm, Email: mchisholm777@gmail.com.
Shannon Sahlqvist, Email: shannon.sahlqvist@deakin.edu.au.
References
- 1.Lee IM, Shiroma EJ, Lobelo F, et al. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. 2012;380:219–229. doi: 10.1016/S0140-6736(12)61031-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Australian Bureau of Statistics . Australian health survey: physical activity, 2011–12. Canberra: Australian Bureau of Statistics; 2013. [Google Scholar]
- 3.Kahn EB, Ramsey LT, Brownson RC, et al. The effectiveness of interventions to increase physical activity. A systematic review. Am J Prev Med. 2002;22:73–107. doi: 10.1016/S0749-3797(02)00434-8. [DOI] [PubMed] [Google Scholar]
- 4.Kassavou A, Turner A, French DP. Do interventions to promote walking in groups increase physical activity? A meta-analysis. Int J Behav Nutr Phys Act. 2013;10:18. doi: 10.1186/1479-5868-10-18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ogilvie D, Foster CE, Rothnie H, et al. Interventions to promote walking: systematic review. BMJ. 2007;334:1204. doi: 10.1136/bmj.39198.722720.BE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hanson S, Jones A. Is there evidence that walking groups have health benefits? A systematic review and meta-analysis. Br J Sports Med. 2015;49:710–715. doi: 10.1136/bjsports-2014-094157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Foster CE, Brennan G, Matthews A, McAdam C, Fitzsimons C, Mutrie N. Recruiting participants to walking intervention studies: a systematic review. Int J Behav Nutr Phys Act. 2011;8:137. doi: 10.1186/1479-5868-8-137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Linke SE, Gallo LC, Norman GJ. Attrition and adherence rates of sustained vs. intermittent exercise interventions. Ann Behav Med. 2011;42:197–209. doi: 10.1007/s12160-011-9279-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Picorelli AM, Pereira LS, Pereira DS, Felicio D, Sherrington C. Adherence to exercise programs for older people is influenced by program characteristics and personal factors: a systematic review. J Physiother. 2014;60:151–156. doi: 10.1016/j.jphys.2014.06.012. [DOI] [PubMed] [Google Scholar]
- 10.Australian Bureau of Statistics . Census of population and housing: Socio-Economic Indexes for Areas (SEIFA), Australia, 2011. Canberra: Australian Bureau of Statistics; 2013. [Google Scholar]
- 11.Brown WJ, Trost SG, Bauman A, Mummery K, Owen N. Test-retest reliability of four physical activity measures used in population surveys. J Sci Med Sport. 2004;7:205–215. doi: 10.1016/S1440-2440(04)80010-0. [DOI] [PubMed] [Google Scholar]
- 12.Timperio A, Salmon J, Rosenberg M, Bull FC. Do logbooks influence recall of physical activity in validation studies? Med Sci Sports Exerc. 2004;36:1181–1186. doi: 10.1249/01.MSS.0000132268.74992.D8. [DOI] [PubMed] [Google Scholar]
- 13.Australian Institute for Health & Welfare . The active Australia survey: a guide and manual for implementation, analysis and reporting. Canberra: Australian Institute for Health & Welfare; 2003. [Google Scholar]
- 14.Australian Bureau of Statistics . Family characteristics and transitions, Australia, 2012–13. Canberra: Australian Bureau of Statistics; 2015. [Google Scholar]
- 15.Australian Bureau of Statistics . Household income and wealth, Australia, 2013–14. Canberra: Australian Bureau of Statistics; 2015. [Google Scholar]
- 16.Australian Bureau of Statistics . Reflecting a nation: stories from the 2011 census, 2012–2013. Canberra: Australian Bureau of Statistics; 2012. [Google Scholar]
- 17.Australian Bureau of Statistics . Estimates of aboriginal and Torres Strait Islander Australians, June 2011. Canberra: Australian Bureau of Statistics; 2013. [Google Scholar]
- 18.Australian Bureau of Statistics . Australian health survey: updated results, 2011–12. Canberra: Australian Bureau of Statistics; 2013. [Google Scholar]
- 19.Australian Bureau of Statistics . Australian health survey: first results, 2011–12. Canberra: Australian Bureau of Statistics; 2013. [Google Scholar]
- 20.Jancey J, Lee A, Howat P, Clarke A, Wang K, Shilton T. Reducing attrition in physical activity programs for older adults. J Aging Phys Act. 2007;15:152–165. doi: 10.1123/japa.15.2.152. [DOI] [PubMed] [Google Scholar]
- 21.Schmidt JA, Gruman C, King MB, Wolfson LI. Attrition in an exercise intervention: a comparison of early and later dropouts. J Am Geriatr Soc. 2000;48:952–960. doi: 10.1111/j.1532-5415.2000.tb06894.x. [DOI] [PubMed] [Google Scholar]
- 22.Matthews A, Brennan G, Kelly P, McAdam C, Mutrie N, Foster C. “Don’t wait for them to come to you, you go to them”. A qualitative study of recruitment approaches in community based walking programmes in the UK. BMC Public Health. 2012;12:635. doi: 10.1186/1471-2458-12-635. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Bauman AE, Reis RS, Sallis JF, et al. Correlates of physical activity: why are some people physically active and others not? Lancet. 2012;380:258–271. doi: 10.1016/S0140-6736(12)60735-1. [DOI] [PubMed] [Google Scholar]
- 24.Goodman A, Gatward R. Who are we missing? Area deprivation and survey participation. Eur J Epidemiol. 2008;23:379–387. doi: 10.1007/s10654-008-9248-0. [DOI] [PubMed] [Google Scholar]
- 25.Picavet HS. National health surveys by mail or home interview: effects on response. J Epidemiol Community Health. 2001;55:408–413. doi: 10.1136/jech.55.6.408. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Sallis JF, Haskell WL, Fortmann SP, Vranizan KM, Taylor CB, Solomon DS. Predictors of adoption and maintenance of physical activity in a community sample. Prev Med. 1986;15:331–341. doi: 10.1016/0091-7435(86)90001-0. [DOI] [PubMed] [Google Scholar]
- 27.Resnick B, Spellbring AM. Understanding what motivates older adults to exercise. J Gerontol Nurs. 2000;26:34–42. doi: 10.3928/0098-9134-20000301-08. [DOI] [PubMed] [Google Scholar]
- 28.Foreman R, van Uffelen JG, Brown WJ. Twelve month impact of the just walk it program on physical activity levels. Health Promot J Austr. 2012;23:101–107. doi: 10.1071/he12101. [DOI] [PubMed] [Google Scholar]
- 29.Cleland V, Granados A, Crawford D, Winzenberg T, Ball K. Effectiveness of interventions to promote physical activity among socioeconomically disadvantaged women: a systematic review and meta-analysis. Obes Rev. 2013;14:197–212. doi: 10.1111/j.1467-789X.2012.01058.x. [DOI] [PubMed] [Google Scholar]
- 30.Nulty DD. The adequacy of response rates to online and paper surveys: what can be done? Assess Eval High Educ. 2008;33:301–314. doi: 10.1080/02602930701293231. [DOI] [Google Scholar]
- 31.World Health Organization (WHO). Obesity: Preventing and Managing the Global Epidemic Geneva: WHO;1998. [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The dataset analysed during the current study are not publicly available due to privacy and ethical restrictions, since they were collected by the Heart Foundation for the purpose of evaluation only and not for additional research or interrogation. Queries about data may be directed to the corresponding author who will liaise with the data custodian at the Heart Foundation.